Epidural analgesia
Anatomy
The epidural space extends from the foramen magnum to the sacrococcygeal membrane. It lies anterior to the ligamentum flavum and posterior to the posterior longitudinal ligament.
It contains fat, veins (Batson's plexus), connective tissue, nerve roots, and the dural sac. The innervation for the uterus is derived from T10 to L1 nerve IndicationsEpidural analgesia is indicated primarily for pain relief in labour (7). It also has the advantage of providing pain relief for episiotomy and perineal suturing. Epidural anaesthesia can be used as an adjunct in the management of severe pre-eclampsia due to the vasoactive hypotensive effect of the sympathetic blockade resulting from epidural local anaesthetic administration. Epidural anaesthesia can also be performed de novo for operative intervention where spinal block may not be appropriate. A dose of concentrated local anaesthetic can be administered in order to ‘top up' a labour epidural for operative delivery. Anaesthesia to the T4 dermatome level bilaterally is necessary to minimize the chances of the parturient experiencing pain during a caesarean section.
Contraindications
• Patient refusal.
• Prophylactic low-molecular-weight heparin within 12 hours.
• Treatment dose low-molecular-weight heparin within 24 hours.
• Platelet count less than 100 ? 109/mL with an abnormal clotting screen.
• Platelet count less than 80 ? 109/mL.
• Systemic sepsis.
• Local skin infection.
Technique
A soft plastic catheter is introduced into the epidural space using a specially designed needle called a Tuohy needle. An intervertebral space is identified by palpating the spinous processes. Traditionally, the L3/4 interspace is chosen because the spinal cord ends at L1/2. In theory, an epidural may be inserted at any interspace but a spinal needle should only be inserted at a level below where the spinal cord ends to avoid injury to the spinal cord.
The L3/4 level can be identified by palpating the iliac crests. An imaginary line between the two crests transects the L3/4 interspace (Tuffier's line). A ‘loss of resistance to saline' technique is used to safely advance the needle into the epidural space. The catheter is introduced through the Tuohy needle, which is then removed, leaving the catheter in place (8). Between 3 and 5 cm of catheter is left in the epidural space, through which a local anaesthetic solution can be administered. A low-dose concentration of local anaesthetic is delivered in combination with an opioid which improves the quality and duration of analgesia. A typical regimen uses 0.1% levobupivacaine with 2 mcg/mL fentanyl. The anaesthetic solution can be administered as intermittent boluses, continuous infusion, or patient- controlled boluses (patient- controlled epidural analgesia).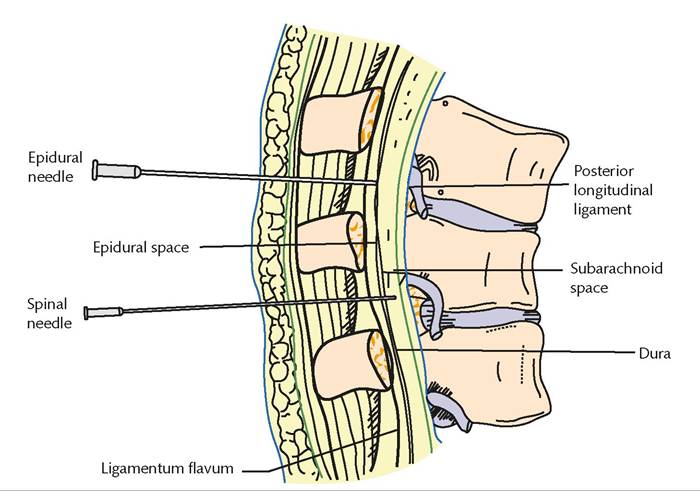
Figure 28.1 Subarachnoid and epidural spaces.
Reproduced from Allman KG, McIndoe A, Wilson I. (2011). Oxford Handbook of Anaesthesia, 3rd edn. With permission from Oxford University Press.
Risks and complications
Epidural analgesia is safe. The third national audit project of the Royal College of Anaesthetists reported an incidence of permanent harm of 0.6 per 100,000.
Other complications include:
• permanent nerve damage (1:100,000)
• temporary nerve damage (1:1000)
• increased likelihood of instrumental delivery (1:10)
• epidural abscess
• epidural haematoma
• postdural puncture headache (1:250).