32 Family Planning: Contraception, Sterilization, and Abortion
Sarah Oman
Anne E. Burke
Family planning is an integral part of the health care of women. By age 45 years, more than half of all American women will have had an unintended pregnancy and 3 in 10 will have had an abortion.
Recognition of the potential for improved access to family planning services presents an opportunity to improve maternal mortality rates, population growth, and the status of women in society.CONTRACEPTION
Contraceptive use is exceedingly common among women of reproductive age, although effective and consistent contraceptive use continues to pose challenges.
• Ninety-nine percent of women of reproductive age (15 to 44 years old) in the United States have used at least one contraceptive method and 62% are currently using contraception.
• Among women affected by unintended pregnancy, 60% report contraceptive use in the month prior to the pregnancy, suggesting incorrect or inconsistent use of their chosen method(s).
• Increasing the use of long-term, highly effective methods, such as intrauterine devices and implantable contraceptives, may reduce the number of unintended pregnancies.
• Contraceptive use is associated with improved health outcomes for women and children.
• Contraceptive use prevents obstetric complications by facilitating birth spacing and preventing unintended pregnancies at the extremes of reproductive age.
• Noncontraceptive benefits of hormonal contraception include improvement in menstrual and perimenstrual symptoms, bleeding patterns, and acne and decreased risk of developing ovarian and endometrial cancer.
• Physicians can optimize consistent long-term use of contraception among their patients through counseling that takes into account medical history, ethical and religious concerns, the patient's short- and long-term childbearing plans, and prior contraceptive use history.
• Table 32-1 lists contraceptive methods available in the Unites States, along with their perfect-use and typicaluse failure rates.
• Contraceptive methods can be considered in terms of “tiers of effectiveness” based on pregnancy rates with typical use.
P.422
TABLE 32-1 Efficacy of Various Contraceptive Methods
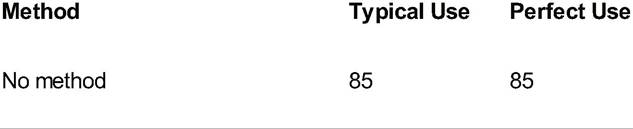
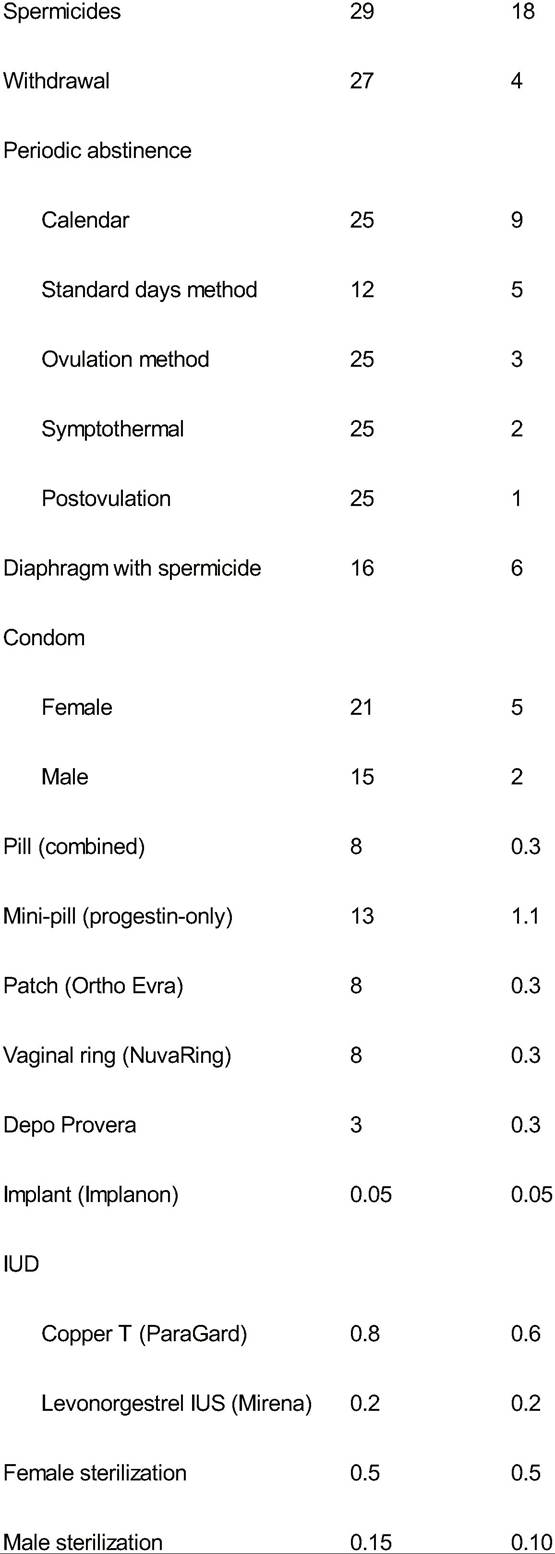
IUD, intrauterine device; IUS, intrauterine system.
• An example of a visual aid that can be used for patient counseling is shown in Figure 32-1.
• In this chapter, we will discuss methods in approximate descending order of effectiveness.
• Another useful resource is the Centers for Disease Control and Prevention’s (CDC's) U.S. Medical Eligibility Criteria for Contraceptive Use (US MEC), which can be consulted to determine safe contraceptive methods for women with medical comorbidities (T able 32-2).
• This resource, available online and as a downloadable “app,” provides guidance for safe use of contraceptives; it does not address comparative risks of pregnancy in women with medical conditions.
Most Effective Methods: Sterilization and Long-Acting Reversible Contraception
Bilateral Tubal Ligation
• Bilateral tubal ligation (BTL) is a surgical procedure in which the fallopian tubes are permanently occluded, preventing sperm from fertilizing the ovum. The procedure
P.423 can be performed postpartum (within 48 hours after vaginal delivery), at the time of cesarean delivery, or as an interval procedure (>6 weeks postpartum) via laparoscopic or transcervical hysteroscopic approach.
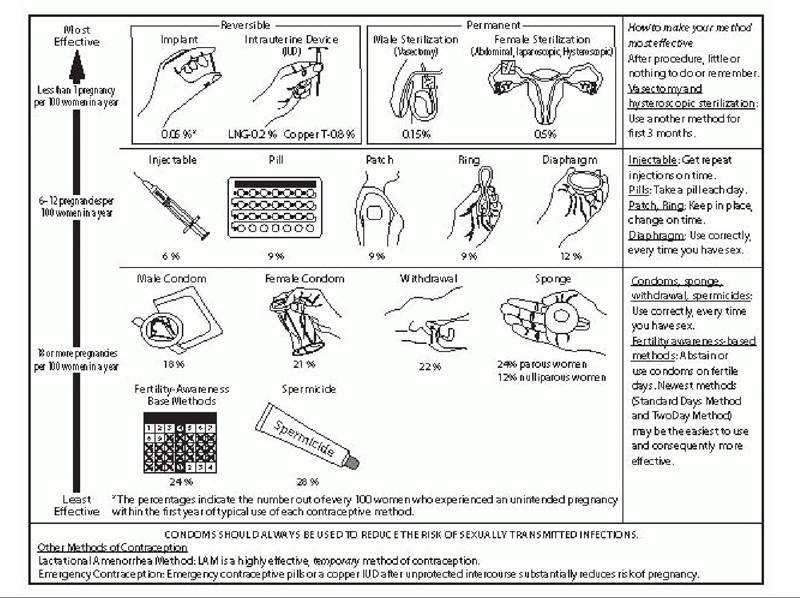
Figure 32-1. Contraceptive counseling tool: tiers of effectiveness.
[1] The Parkland and Pomeroy salpingectomies are the most common methods used for postpartum sterilization.
These involve ligating and excising portions of the tubes via an infraumbilical incision.Laparoscopic tubal ligation is performed via banding, clipping, or cauterizing the tubes.
The Collaborative Review of Sterilization (CREST) study, a landmark analysis of tubal sterilization, compared
the long-term effectiveness of numerous methods of sterilization and found a rate of 18.5 pregnancies per 1,000 procedures overall (Table 32-3).
• Advantages of transabdominal sterilization include the fact that these procedures offer highly effective, permanent contraception to women who desire no future childbearing. Sterilization may decrease the risk of ovarian cancer, possibly by blocking carcinogens from ascending through the fallopian tubes.
• Disadvantages include the need for anesthesia for sterilization via an abdominal approach, risk of surgical complications, and sterilization failure resulting in either intrauterine or ectopic pregnancy. Sterilization failure rates are higher for women younger than the age of 30 years because these women are more fertile at the time of sterilization.
• The reported 10-year cumulative probability of ectopic pregnancy for all sterilization methods in the CREST study was 7/1,000, with greater risk of ectopic
P.424
P.425 pregnancy in younger women. However, although the relative risk of ectopic pregnancy (chance that a pregnancy, once it occurs, may be ectopic) may be higher after sterilization, the absolute risk of ectopic pregnancy is lower than in noncontracepting women due to the high efficacy of sterilization. The risk of regret of sterilization is significantly higher in women sterilized prior to age 30 years.
TABLE 32-2 Contraindications to Estrogen-Containing Hormonal Contraception
Migraines without aura and age >35 yr
Symptomatic gallbladder disease
Undiagnosed vaginal bleeding
Non-breast-feeding to be removed, however, when cervical cancer or dysplasia is discovered and/or treated. Active pelvic infection is a contraindication; pelvic infection is further discussed in the following text.
Although HIV infection does not contraindicate IUD placement, AIDS is considered to be a contraindication.• Risks: Risks of IUD insertion include expulsion (2%), perforation (1:1,000), pregnancy (2 to 8:1,000), and infection (uncommon).
• Other considerations: Immediate postpregnancy (postpartum and postabortal) IUD placement is safe and may lead to a substantial decrease in unplanned pregnancy. Expulsion risk may be higher than when placement is not associated with pregnancy, but this risk can be balanced against other benefits and concerns.
• Pelvic infection: A woman's risk of pelvic inflammatory disease (PID) is not increased by IUD use. The progestin IUS (Mirena) may decrease risk by decreasing ascending infection due to thickening of the cervical mucus. The copper IUD does not affect risk. The historic association between IUDs and PID originated with the
P.427 Dalkon Shield, an IUD used in the 1970s that had a braided filament string that was associated with increased risk of PID. Modern IUDs have monofilament strings that do not share this risk.
• Placement of an IUD at the time of an active pelvic infection does increase risk of developing PID. Women with evidence of or high suspicion for active sexually transmitted infections should be screened for STDs and have these treated before having IUDs placed. Otherwise, patients with risk factors (as defined by the CDC) can be screened for chlamydia and gonorrhea at the time of placement. Women with no risk factors or symptoms need not receive additional screening prior to IUD insertion.
• History of PID or ectopic pregnancy is not a contraindication to IUD use. Diagnosis of uncomplicated chlamydia or gonorrhea infection does not necessitate IUD removal: Treatment can be offered with IUD in place. PID that is diagnosed with an IUD in place should be treated, and the IUD may be left in situ in many
cases.
• Postinsertion pregnancy: Although the relative risk of ectopic pregnancy is higher among pregnancies occurring with an IUD in place, the overall risk of ectopic pregnancy is reduced by an IUD because pregnancy risk is markedly decreased.
If a woman has a desired intrauterine pregnancy with an IUD in place, the IUD should be removed if possible.Progestin-Only Implants (Nexplanon)
• Implants are another form of highly effective, reversible contraception. The only implant currently available in the United States is Nexplanon (formerly Implanon) (Merck, New York, USA).
• It consists of a single rod, 4 cm ? 2 mm (the approximate size of a match), that releases a contraceptive dose of etonogestrel for 3 years. The dose is sufficient to suppress ovulation, as well as to prevent pregnancy through progestin-mediated cervical mucus thickening and endometrial atrophy (see the section “Progestin-Only Methods”).
• The implant is placed under the skin of the upper (usually nondominant) arm and injected from a preloaded insertion device. FDA-mandated training is required for clinicians who wish to provide or remove the implant. The implant is extremely effective and suitable for women who desire long-term reversible contraception and are comfortable with the side effect profile.
• Advantages: Implants provide highly effective protection against pregnancy and are relatively easy to insert and remove. Some women may experience decreased menstrual bleeding or amenorrhea. Return to fertility is rapid after removal.
• Side effects/disadvantages: Menstrual disturbances are common with Nexplanon use.
• Bleeding patterns can be unpredictable and may vary over time in the same individual. Intolerance of bleeding may lead to discontinuation and patients should be counseled appropriately.
• Interventions such as short-term estrogen, oral contraceptive pills, doxycycline, or scheduled NSAIDs have been studied for treatment of bothersome bleeding with the contraceptive implant, but evidence for their effectiveness is mixed at best.
• With no intervention, about 50% of women who continue contraceptive implant use despite unacceptable bleeding will experience improvement over time.
P.428
• There may be other hormonal side effects, such as headache and acne, which may be more likely to resolve within a few months of insertion, as etonogestrel levels decrease to their steady-state following the initial period of higher hormone release.
• Risks: Insertion is generally quite safe, but rare complications can include infection, injury to nerves, allergic reaction, or incorrect placement leading to complications of removal.
• Contraindications: There are few evidence-based contraindications to progestinonly methods. These are discussed in the following text in the review of shorter acting progestin-only methods.
Shorter Acting Methods of Hormonal Contraception
Hormonal contraceptives have been used routinely for over 50 years in the United States. These methods are extremely safe when provided appropriately. They can also be highly effective when used correctly and consistently. In addition to the longacting reversible contraception methods, hormonal contraception refers both to progestin-only methods (mini-pill, injection) as well as combined estrogen-progesterone methods (combined oral contraceptives [COCs], transdermal patch, and vaginal ring).
Progestin-Only Methods
• Synthetic progestin preparations prevent pregnancy without the use of estrogen.
• Some progestin-only methods prevent ovulation, but all act on the cervical mucus to thicken it and make it unfavorable to sperm penetration.
• Progestin-induced transformation of the endometrium creates an intrauterine environment unfavorable to fertilization and possibly implantation.
• There are few true contraindications, and these methods can be used in many women with contraindications to combined hormonal contraceptive use.
• Contraindications to progestin-only methods (implants, injections, and pills) include breast cancer, complicated diabetes, and severe active liver disease or cirrhosis.
• Most other women can safely use these methods of contraception.
• For further guidance, refer to the US MEC mentioned earlier in this chapter.
Injectable Contraceptives
• Depo medroxyprogesterone acetate (DMPA) is a progestin-only injectable contraceptive that is injected intramuscularly (IM) (150 mg) by a medical provider every 3 months.
• The World Health Organization recently released guidance indicating that the contraceptive effect likely persists up to 17 weeks.
• DMPA provides highly effective contraception, although its potential effectiveness is limited by a discontinuation rate of over 40% in the first year of use.
• There is also a subcutaneous formulation (DMPA-SC) containing 104 mg DMPA.
î Although similar in efficacy and side effect profile to DMPA-IM, it is less widely used.
• Advantages: effective contraception. Noncontraceptive benefits include reduction in menstrual blood loss, improvement of anemia, protection against endometrial cancer, reduced seizure frequency in some women with epilepsy, and reduced frequency of sickle crises.
P.429
• Side effects/disadvantages: Side effects include irregular bleeding, delayed return to fertility, and weight gain. DMPA has also been associated with hair loss in some patients. Although irregular bleeding is common after the first injection, 50% of women become amenorrheic after the first year of use.
• The average delay in return to ovulatory function is 6 to 10 months after the last injection but delay of up to 18 months is possible.
î Patients should be counseled on this potential delay, as it can impact future childbearing plans.
• There has long been concern about weight gain with DMPA.
• In many studies, this weight gain has not proven significant and may reflect overall weight change with age and the US obesity epidemic, especially in adolescents.
• Certain subpopulations may be more susceptible than others.
• Although this is an ongoing area of research, indications are that obese adolescents may be more likely than nonobese adolescents to gain weight on DMPA.
• The same link may not be true for adult women, however, women who gain weight rapidly following initiation of DMPA should be counseled that weight gain is likely to increase with continued use.
• A “black box” FDA warning states that DMPA may decrease bone mineral density (BMD), especially in adolescents.
î Studies have also shown this decrease in BMD is measurable after one injection and continues with each subsequent injection.
î This decreased bone density is reversible after DMPA discontinuation, is generally less than one standard deviation below the mean, is comparable in magnitude to that which occurs with breast-feeding, and has not been shown to correlate with an increased risk of fracture.
î The World Health Organization has affirmed that there need not be time restrictions on DMPA use due to bone density concerns.
î Nor does there appear to be a role for routine bone density screening in premenopausal DMPA users, and supplementation with estrogen is not advised.
Progestin-Only Pills (Micronor, Ovrette)
• POP are taken daily with no hormone-free interval.
• They contain lower doses of progestin than COCs.
• They are probably most effective after about 6 hours of ingestion, and contraceptive effect diminishes significantly after 24 hours.
• It is important for patients to take their pill at the same time each day and should be advised to use a backup method if their dose is delayed by more than 3 hours.
• POP available in the United States do not reliably suppress ovulation but rather prevent pregnancy through progestin-mediated effects on the cervical mucus and endometrium.
• Although traditionally suspected of having a higher failure rate than COC, POP are probably about as effective: Both types of pills have a typical-use failure rate of about 9% in the first year of use.
• POP are also safe for use by the vast majority of women; it has been suggested that they would be appropriate for over-the-counter use.
• Side effects include irregular bleeding and possible systemic hormonal effects (e.g., acne).
• Risks are few.
P.430
Combined Hormonal Contraceptives
• These methods contain both synthetic progestin and estrogen. Progestin contributes significantly to the contraceptive effect, whereas estrogen maintains the stability of the endometrium and contributes to ovulation inhibition.
• This allows for monthly withdrawal bleeding and decreases irregular vaginal bleeding. Available methods include oral contraceptives, the transdermal contraceptive patch, and the vaginal contraceptive ring.
• Advantages: Besides providing contraception, combined methods may be used to manage dysmenorrhea, menstrual dysfunction, premenstrual symptoms, ovarian cysts, and acne. Use of COCs is associated with a 40% to 80% reduced risk of ovarian cancer (greater effect seen with longer term use) and a 50% to 70% reduced risk of endometrial cancer. The cancer prevention benefits of COCs are robust enough for some public health experts to advocate counseling women on these benefits even when the contraceptive effects of such medications are not needed. Whether these benefits extend to the other combined methods has not been reported, but it may be possible to extrapolate based on similar components and physiologic effects.
• Side effects/disadvantages: Combined hormonal contraceptives are highly effective and generally well- tolerated, but side effects may include:
• Estrogen: bloating, headache, nausea, mastalgia, leukorrhea, hypertension, melasma, telangiectasias
• Progestin: mood changes, fatigue, mild weight gain, decreased libido
• Risks: Systemic use of estrogen increases the risk of thromboembolism. This must be considered in context, as the overall risk of thromboembolism in most candidates for hormonal contraception is very low, and the additional risk conferred by hormonal contraception is much lower than the risk associated with pregnancy.
• Risk of venous thromboembolism (VTE) in women per year is
î 4/100,000 at baseline
î 10/100,000 in women using COCs
î 20/100,000 in women using patch
î >100/100,000 in pregnant women
î 550/100,000 in postpartum women
• Contraindications: Many contraindications to combined methods are based on concerns for elevated risk of thrombotic events, which may become unacceptably high in the setting of medical conditions that predispose to such complications. These include cigarette smoking in women age 35 years and older, hypertension, personal history of VTE, migraine with aura, the presence of multiple risk factors for cardiac disease, and the presence of antiphospholipid antibodies. Known thrombogenic mutations would also preclude use of combined methods, although routine screening for these is not recommended. Breast and uterine cancer are also contraindications to combined methods. For further guidance, providers can refer to the US MEC mentioned earlier in this chapter.
Combined Oral Contraceptives (“The Pill”)
Current formulations of COCs contain daily peak in estrogen is approximately 25% less with the patch compared to pills.
• The clinical significance of this finding, particularly on the risk of VTE, is unclear, especially because studies have not shown an increased risk of fatal blood clots compared to COCs.
The Combined Hormonal Vaginal Ring (NuvaRing)
• The NuvaRing is a flexible plastic ring 5 cm in diameter and 4 mm in thickness that releases 15 μgZday of EE and 120 μgZday of etonogestrel (progestin).
• It is placed in the vagina for 3 weeks and removed for 1 week, during which withdrawal bleeding occurs.
• Alternatively, the ring can be kept in the vagina for 4 weeks followed by transition immediately to a new ring for women who desire to use this method continuously.
• Coital problems and expulsion of the device are rare.
• If patients desire, the ring may be removed for up to 3 hours, such as during intercourse, although doing this routinely is not recommended.
P.432
• If the ring is out of the vagina for >3 hours, backup contraception should be used until the ring has been back in place for 7 days.
• The ring achieves a lower steady-state level of estrogen compared to the patch and COCs, although it is not known if this difference is clinically significant.
Barrier Methods
Male Condom
• Most male condoms are made of latex, although nonlatex condoms are also available.
• They should be applied before vaginal penetration and should cover the entire length of the erect penis.
• They should not be applied too tightly or loosely and a reservoir should be left to retain the ejaculate.
• Adequate lubrication should be used on both the inside and outside of the condom, and the condom should be removed immediately after ejaculation.
• Condoms with spermicidal lubricant are more effective at preventing pregnancy.
î The CDC currently suggests that women who are at high risk for HIV infection should not use nonoxynol- 9 spermicides because this ingredient may increase the risk of HIV transmission.
• Condoms are highly effective in preventing sexual transmission of HIV and other infections (e.g., gonorrhea, chlamydia, trichomonas). However, because condoms do not cover all exposed areas, they may not be as effective in preventing infections transmitted by skin-to-skin contact (e.g., herpes simplex virus, HPV, syphilis, chancroid).
Female Condom
• Female condoms consist of a polyurethane sheath.
• One type has two flexible rings at either end.
• The closed end with the upper/inner ring is applied against the cervix and the open end with the lower/outer ring rests against the labia minora outside the introitus.
î Adequate lubrication is important for function and comfort.
• Like male condoms, this method decreases sexual transmission of HIV infection and other STDs.
• It also provides extra protection on the outside of the body that may decrease infections transmitted by skin- to-skin contact. There are other female condoms in development.
Diaphragm
• Diaphragms are barrier devices that are inserted into the vagina and prevent sperm from entering the upper genital tract.
• The diaphragm consists of a rubber or latex cup with a flexible ring.
• The edges of the diaphragm should lie just posterior to the symphysis pubis and deep into the cul-de-sac so that the cervix is completely covered behind the center of the diaphragm.
• The largest diaphragm that comfortably fills this space should be selected during an office exam and fitting.
î Diaphragms range in size from 50 to 105 mm in diameter, with the most commonly prescribed diaphragms measuring 65 to 75 mm.
P.433
• Although there is no definitive evidence to support the use of a spermicide with the diaphragm, this is a common recommendation in clinical practice.
î If spermicide is used, it should be applied to the inside of the rubber cup before each act of coitus.
• The diaphragm should be left in place for a minimum of 6 hours after the last coital act but not >24 consecutive hours. It may be placed hours before intercourse.
• Women with uterine prolapse or structural abnormalities of the reproductive tract may not be able to use a diaphragm.
• Patients relying on a diaphragm for contraception should inspect the diaphragm regularly for holes and should replace their diaphragm at least every 2 years.
• Diaphragms may offer some protection against STD transmission but their use increases the risk of urinary tract infection.
Cervical Cap
• A cervical cap is a dome-shaped rubber cap with an inside rim that fits snugly against the outer cervix adjacent to the vaginal fornix.
• This method has decreased efficacy in parous women.
Natural Family Planning
• Natural family planning (NFP) means that a couple voluntarily avoids or interrupts sexual intercourse during the fertile phase of the woman's menstrual cycle. Effectiveness varies significantly based on the individual, as this method relies on regular menses, cooperation of both partners, and abstinence at times. Methods of NFP include:
• Symptothermal: A woman must check her basal body temperature daily and avoid intercourse from the start of menses until 3 days after a spike occurs, indicating that ovulation has occurred and she is no longer at risk for pregnancy in that cycle.
• Cervical mucus: A woman must monitor the texture of her cervical mucus to detect a transition from tacky white-yellow into clear, slippery, stretchy discharge at ovulation. Intercourse is avoided from the onset of menses until 3 days after ovulation was predicted.
• Calendar: Menstrual cycles are charted for 6 months to detect the cycle length and this chart is used to calculate the patient's fertile days based on estimated day of ovulation.
Lactational Amenorrhea Method
• During breast-feeding, suckling causes hormonal changes at the level of the hypothalamus that interrupt the pulsatile release of gonadotropin-releasing hormone. This, in turn, impairs LH surge and ovulation does not occur.
• Lactation offers protection against pregnancy only if strict criteria are followed.
î Women must be exclusively or nearly exclusively breast-feeding and feedings must occur every 3 to 4 hours during the day and every 6 hours at night.
î Supplemental feedings should not exceed 5% to 10% of the total.
î This method is only reliable if the infant is younger than 6 months old.
î Once a woman has resumed menses, it can be assumed that lactation is no longer providing protection against pregnancy.
P.434
Postcoital (emergency) contraception
Emergency contraception (EC), or postcoital contraception, may be used after unprotected intercourse to prevent pregnancy. EC pills work mainly through ovulation prevention. EC via insertion of a copper IUD may disrupt implantation. EC does not affect a pregnancy that has already implanted and is therefore not an abortifacient.
Emergency Contraceptive Pills
• Two types of emergency contraceptive pills (ECP) are available in the United States: LNG (e.g., Plan B) and ulipristal acetate (UPA) (Ella).
• LNG-ECP includes a total of 1.5 mg LNG that may be taken in two doses (0.75 mg 12 hours apart) or one dose (1.5 mg). The single-dose regimen has better compliance with fewer side effects and increased efficacy. LNG-ECP is now available without a prescription for women of all ages. It is effective in preventing pregnancy up to 120 hours after intercourse but effectiveness is inversely related to time since intercourse; therefore, it is most effective when taken immediately after coitus. This regimen is 94% to 98% effective in preventing pregnancy with failure rates at the higher end of this spectrum observed in women who take the dose between 72 to 120 hours after unprotected intercourse. Failure rates may be increased in the obese population.
• Ulipristal acetate (Ella) is a progesterone receptor antagonist taken as a single 30 mg dose within 5 days (120 hours) of unprotected intercourse. It works by directly inhibiting follicle rupture and therefore maintains high efficacy even as ovulation nears. It appears to be at least as effective as LNG, and the efficacy is more consistent over time than seen with LNG. UPA is available by prescription only. UPA is 92% to 99% effective in preventing pregnancy when taken within 5 days of unprotected intercourse. Ulipristal appears to be effective over a wide variety of weights but loses efficacy in women who are morbidly obese.
• IUD as EC: The copper IUD may be inserted within 5 days of unprotected intercourse to decrease the chance of implantation. It is 99.8% to 99.9% effective if inserted within 5 days. According to a recent systematic review of all emergency contraceptive methods, the copper IUD was the most effective method; it is also the only option that addresses not only immediate but future contraception if left in place.
• There are no contraindications to use of EC. Use in pregnancy is not advised; however, the use will not cause termination of existing pregnancy and is not teratogenic. Use of EC is not an ideal method of routine contraception because it is less effective than other methods. However, repeated use is not dangerous. Irregular bleeding and delay of next menses are common after taking EC. Patients are encouraged to take a pregnancy test if menses have not resumed within 1 week after expected menstrual timing.
ELECTIVE PREGNANCY TERMINATION
Epidemiology and History
Forty-one million abortions occur each year worldwide. Half of these are unsafe, resulting in 67,000 maternal deaths from abortion and related complications around the world annually. This accounts for 13% of maternal mortality. Abortion is very safe in the United States, with a mortality rate of 0.6/100,000. Extensive study has P.435 shown that an abortion does not increase the risk of infertility, breast cancer, or future miscarriage. Abortion has not been shown to cause long-term negative psychological effects in the absence of risk factors.
Evaluation, Counseling, and Follow-up
• Providers caring for women with unplanned and undesired pregnancy should be able to counsel patients on
all the options available to them, including induced abortion.
• A nondirective counseling approach should be taken with the patient to ensure that she is confident in her decision. Those who do not provide this service should be able to counsel patients, make appropriate referrals, and manage postabortal complications.
• Prior to abortion, confirmation of intrauterine pregnancy and pregnancy dating should be performed. Maternal Rh status should be obtained, as Rh-negative women should receive RhoGAM at the time of induced abortion (see Chapter 21).
• Contraception should be discussed with all women, as fertility can return immediately. Women can ovulate within 10 days of abortion, and at least half of women will ovulate within 3 weeks of an abortion procedure.
• Pregnancy symptoms usually resolve within 1 week after abortion. Normal menses may take up to 6 weeks to return. Follow-up is traditionally recommended within 2 to 4 weeks to assess for complications, confirm resolution of pregnancy, and readdress contraception.
Surgical Abortion
Surgical Abortion in the First Trimester
Surgical abortion at 30 years. A specially designed handheld 60-mL syringe is attached to either a flexible or rigid cannula of a diameter appropriate for gestational age.
• After aspiration, the tissue should be inspected to verify that the POCs are consistent with the gestational age.
• Sharp curettage is generally not necessary. The use of sharp curettage increases the pain of the procedure. It may also contribute to bleeding and increased risk of uterine perforation.
• Antibiotics should be administered for infection prophylaxis. Doxycycline is a commonly used and costeffective choice.
Surgical Abortion in the Second Trimester
• The most commonly used surgical procedure for second trimester abortion is dilation and evacuation (D&E). D&E is considered the preferred method of secondtrimester termination when experienced personnel are available and autopsy of an intact fetus is not required.
• In experienced hands, D&E is the safest available method of second-trimester termination.
• The procedure for surgical termination between 14 and 22 weeks' gestation is different in several important ways from a first-trimester D&C. Instrumental removal of the POCs is usually required. It is essential to examine and account for all POCs consistent with gestational age.
• Preoperative cervical preparation is highly recommended. This can be accomplished via medications that ripen the cervix or by osmotic dilators.
î Choice of technique depends on provider experience, gestational age, and availability. Osmotic dilators, such as Dilapan (polyacrylonitrile) or laminaria (dried seaweed Laminaria japonica), absorb cervical moisture, and as they do, they enlarge and dilate the cervical canal.
î They also cause the release of prostaglandins, which ultimately disrupt the cervical stroma and soften the cervix.
î Osmotic dilators must be placed several hours before the procedure or overnight for maximum effect.
î For procedures later in the second trimester, dilation is often carried out over 1 to 2 days, and sequential insertion of osmotic dilators may be used.
• Ultrasonographic confirmation of gestational age is considered essential and has become standard in most practice environments.
î The procedure may also be carried out under ultrasound guidance to facilitate complete and efficient evacuation.
î Ultrasound guidance is not a substitute for competence, however, and does not eliminate risk of complications.
P.437
Medical Abortion
Medical Abortion in the First Trimester
• Evidence-based medical abortion regimens are safe and effective up to 63 days of gestation, with some recent research supporting use beyond 63 days. Medical abortion can be performed using mifepristone (RU-486) and misoprostol, or methotrexate and misoprostol. The latter has fallen out of favor, as it is less effective than mifepristone/misoprostol.
• Mifepristone is a progesterone antagonist. Its effects include alterations in the endometrial blood supply, blocking the support of pregnancy and softening the cervix.
• Methotrexate inhibits DNA synthesis and affects rapidly dividing cells, including trophoblast.
• Misoprostol is a prostaglandin that is used to induce uterine contractions after administration of either mifepristone or methotrexate, thus promoting expulsion of the POCs.
• Evidence-based recommendations support the use of mifepristone and misoprostol up to 63 days of gestation and with a lower mifepristone dose (200 mg vs. 600 mg) than the FDA-approved regimen, which was based on a gestational age limit of 49 days.
• Where access to other options is limited, misoprostol alone can be used in repeat 24-hour dosing intervals for medical abortion. Effectiveness may vary from 47% to 96%.
• Medical abortion is a different experience than surgical abortion, more akin to a miscarriage.
• The abortion may take several days to complete.
• A follow-up visit is generally required to confirm completion because surgical evacuation is advised in case of medication failure.
• It is important for patients to be counseled accordingly and be able to follow up.
• Side effects following administration of mifepristone and misoprostol consist primarily of pain, bleeding, and gastrointestinal (GI) upset.
Medical Abortion in the Second Trimester
• Medical second-trimester abortion may be the best alternative in some settings. It does not require anesthesia, a skilled operator is not required, and fetal examination can be performed on an intact fetus, such as in cases of genetic termination.
• However, as compared with D&E, the procedure can take 24 hours or longer, major complications and mortality are higher, and fever and severe GI side effects are common when prostaglandins are used.
• The overall goal is to administer medications that cause uterine contractions and lead to the expulsion of the
POCs. Medications include high-dose intravenous oxytocin and different preparations of vaginally administered prostaglandins (prostaglandin E2 [Prostin E2] and misoprostol). Less commonly, hypertonic solutions (saline or urea) may be administered intra-amniotically to induce second-trimester abortions. Antiprogestins, such as mifepristone, may also be used.
Abortion Complications
Fortunately, legal abortion is a safe procedure. However, as with any other procedure, complications can occur. Complications with medical abortion generally stem from retained POCs, bleeding, and infection.
P.438
Risks of Surgical Abortion
• Perforation is a risk of surgical abortion. Management of perforation is beyond the scope of this chapter, but there are principles one can follow.
• If perforation is suspected, the suction is stopped, suction is not applied, and the patient should be examined clinically and with ultrasound.
• If she is stable, observation with close monitoring may be appropriate.
• If the patient shows signs of bleeding or instability, surgical management (laparoscopy vs. laparotomy) should be performed.
• Excess uterine bleeding or hemorrhage due to atony can be managed with uterotonics, such as misoprostol, Methergine, or oxytocin. Bimanual massage is also helpful.
• Hematometra should be suspected if a patient has intense pain and an enlarged uterus immediately after surgical abortion.
• Surgical reaspiration is the key to management, and uterotonics such as Methergine can be considered.
• Postabortal endomyometritis may present with fever and abdominal pain postabortion.
• Oral or intravenous doxycycline and a cephalosporin, with or without metronidazole, should be administered.
• The decision to use outpatient versus inpatient management can be made applying criteria similar to those designated for PID.
• Retained POCs after abortion can cause fever, pain, bleeding, and/or symptoms of pelvic infection. The treatment is evacuation of the uterus.
• Oral prophylactic doxycycline administration, before or after surgical abortion, can reduce the risk of postabortion endomyometritis by 40%.
Risks of Medical Abortion
• Medical abortion has a low complication rate.
• Continuing pregnancy occurs in 1 % to 3% of cases.
• Retained products may also occur.
• These can be managed by surgical evacuation or possibly by an additional dose of misoprostol.
• The risk of bleeding severe enough to require transfusion is far less than 1 %.
• A series of case reports that appeared several years ago described a very rare risk of fatal sepsis resulting from medical abortion related to Clostridium sordellii.
• In response to this, some providers have come to recommend buccal administration of misoprostol over vaginal, although whether this or prophylactic antibiotics further decrease infection risk is controversial.
SUGGESTED READINGS
Blumenthal P, Edelman A. Hormonal contraception. Obstet Gynecol 2008;112(3):670-684.
Chervenak FA, McCullough LB. The ethics of direct and indirect referral for termination of pregnancy. Am J Obstet Gynecol 2008:199(3):232-233.
Clark MK, Sowers MR, Nichols S, et al. Bone mineral density changes over two years in firsttime users of depot medroxyprogesterone acetate. Fertil Steril 2004;82:1580-1586.
Grimes DA, Lopez LM, Manion C, et al. Cochrane systematic review of IUD trials: lessons learned. Contraception 2007;75(6)(suppl):S55-S59.
P.439
Jabara S, Barnhart K. Is Rh immune globulin needed in early first-trimester abortion? A review. Am J Obstet Gynecol 2003;188:623-627.
Morrison CS, Bright P, Wong EL, et al. Hormonal contraceptive use, cervical ectopy, and the acquisition of cervical infections. Sex Transm Dis 2004;31:561-567.
Mosher WD, Martinez GM, Chandra A, et al. Use of contraception and use of family planning services in the United States: 1982-2002. Advanced Data 2004;350:1-36.