31 Urogynecology and Reconstructive Pelvic Surgery
Jennifer L. Hallock
Chi Chiung Grace Chen
Urogynecology is the subspecialty of obstetrics and gynecology that addresses aspects of pelvic floor dysfunction in women including urinary incontinence (UI), anal incontinence (AI), and pelvic organ prolapse (POP).
Symptomatic pelvic floor disorders are common, ranging from 25% to 50% in American women and increasing with age.• Little is known about the natural history of pelvic floor disorders. For instance, not all women with prolapse are symptomatic, and symptoms do not necessarily correlate with physical exam findings.
• Pelvic floor disorders such as POP are the indication for more than 300,000 surgeries annually in the United States at a cost of $1 billion. Up to 11 % of women have surgery for POP or stress urinary incontinence (SUI) by the age of 80 years. Twenty-nine percent of patients will require repeat surgery.
NORMAL ANATOMY AND FUNCTION
• Anatomy of the bladder: The bladder is both an elastic muscular reservoir and a pump for urination. The urethra serves as the conduit, but micturition requires coordination of urethral and bladder functions. Urethral muscular components which affect urinary continence include an outer layer of striated muscle arranged in a circular pattern (external urethral sphincter [EUS]). Internal to the striated component of the urethral sphincter is a circular layer of smooth muscle, which in turn surrounds a well-developed layer of inner longitudinal muscle (internal urethral sphincter [IUS]). Deep to these layers is a prominent vascular plexus that is believed to contribute to continence by forming a watertight seal via coaptation of the mucosal surfaces. Distally, the fibers of the compressor urethrae pass over the urethra to insert into the urogenital diaphragm near the pubic ramus. Urethral function
P.406 is also impacted by the relatively static supportive layer beneath the vesical neck, which provides a backstop against which the urethra is compressed during increased intra-abdominal pressure.
TABLE 31-1 Neuroanatomy of the Bladder and Urethra
| Muscle | Innervation | Neurotransmitter Rreceptors |
| External urethral sphincter (EUS) | Perineal branch of pudendal nerve | Nicotinic acetylcholine |
| Internal urethral sphincter (IUS) | Sympathetic fibers from hypogastric plexus | Muscarinic acetylcholine, alpha- and betaadrenergic, and others |
| Detrusor relaxation | Sympathetic fibers | Beta-adrenergic |
Detrusor contraction
Parasympathetic fibers from Muscarinic acetylcholine
sacral plexus
Adapted from de Groat WC. Integrative control of the lower urinary tract: preclinical perspective. Br J Pharmacol 2006;147(S2):S25-S40.
• Neurophysiology of the lower urinary tract (Table 31-1)
• Micturition cycle: The bladder has two basic functions: storing urine (sympathetic) and, when socially appropriate, evacuating urine (parasympathetic). Bladder filling occurs with relaxation of the detrusor muscle and contraction of the IUS. With bladder filling, afferent activity via baroreceptors triggers the storage reflex to maintain sympathetic tone in the IUS. When the bladder is full, afferent activity in the pelvic nerve stimulates the micturition reflex.
• Anatomy of the pelvic floor: See Chapter 26.
• Anatomy of the anal sphincters: The internal anal sphincter (IAS) is smooth muscle innervated by the parasympathetic nervous system and is tonically contracted, whereas the external anal sphincter (EAS) is striated muscle innervated by sympathetic nervous system and can only sustain voluntary contraction for a few minutes. The puborectalis muscle and the EAS function together.
• Anal continence is the end result of orchestrated functioning of the cerebral cortex, along with sensory and motor fibers innervating the colon, rectum, anus, and pelvic floor.
The distension of the rectum by stool entering from the sigmoid colon causes the urge to defecate, and the IAS to relax while the EAS contracts (known as the rectoanal inhibitory reflex). At an appropriate time, the anorectal angle is straightened, the rectum is contracted, the EAS is inhibited, and the rectal contents are released. Rectal filling beyond 300 mL results in the sensation of urgency.ETIOLOGY OF PELVIC FLOOR DISORDERS
• Most women with pelvic floor disorders have multiple risk factors.
• Race: Epidemiologic studies have not consistently demonstrated any racial or ethnic difference in the prevalence of pelvic floor disorders. Some studies address variables such as knowledge and perception about pelvic floor disorders and access to care.
P.407
• Age: The prevalence of POP, UI, and AI has been observed to increase with age. Although bladder capacity, ability to postpone voiding, bladder compliance, and urinary flow rate decrease with age in both sexes, overactive bladder symptoms and incontinence are not a normal result of aging.
• Hypoestrogenism: Estrogen deficiency can result in urogenital atrophy with resultant thinning of the submucosa and a decrease in the functional urethral length. The literature is unclear as to the association of estrogen deficiency and lower urinary tract symptoms (LUTS).
• Parity and childbirth: The incidence of pelvic floor disorders such as UI, POP, and AI are higher among parous than nulliparous women. Damage to the pelvic tissues during a vaginal delivery is thought to be a key factor in the development of these disorders, which may be more significant with operative delivery. In addition, lacerations of the internal and external anal sphincters at the time of vaginal delivery can result in impaired anal sphincter strength and AI.
• Underlying medical conditions such as diabetes, obesity, dementia, stroke, depression, Parkinson, or multiple sclerosis may be risk factors for pelvic floor disorders.
• Previous pelvic surgery may increase the risk of pelvic floor disorders.
• Pharmacologic agents, such as diuretics, caffeine, anticholinergics, and alphaadrenergic blockers, may affect urinary tract function.
• Chronically increased intra-abdominal pressure (chronic obstructive pulmonary disease [COPD], chronic constipation, obesity) may be a risk factor for LUTS and POP.
PATIENT EVALUATION IN UROGYNECOLOGY
History and Physical Examination
• Any patient evaluation in urogynecology should include a thorough medical, surgical, gynecologic, and obstetric history. The clinical evaluation should elicit the patient's complaints, defining the location and severity of support defects and evaluating other potential etiologies of pelvic floor symptoms. Pelvic floor defects are rarely localized to one anatomic compartment and are often multifactorial. The clinician should gain an understanding of the duration, frequency, severity, precipitating factors, social impact, effect on hygiene, effect on quality of life, and measures used to avoid bothersome symptoms. Patients may be reluctant to volunteer symptoms of pelvic floor disorders.
• Symptoms of pelvic floor disorders including LUTS, POP, or AI can be grouped into four main categories:
• Bulge: Patients may complain of pelvic pressure, heaviness, protruding tissues, or bulging.
• Voiding dysfunction or incontinence: Patients may complain of day- or nighttime involuntary loss of urine, with or without Valsalva or urgency. Patients may have symptoms associated with urethral obstruction secondary to prolapse, especially with anterior compartment prolapse. They may have urinary hesitancy, incomplete emptying, or the need for vaginal splinting or Valsalva before successfully passing urine. Patients may have associated recurrent or persistent urinary tract infections (UTIs) secondary to urinary retention. They may also report irritative voiding symptoms such as urgency, frequency, and urge incontinence. They may demonstrate occult stress incontinence when prolapse is reduced (e.g., after surgery or with pessary placement).
P.408
• Defecatory dysfunction: Patients may have symptoms of defecatory dysfunction, especially with apical and posterior compartment prolapse. These include symptoms of incomplete defecation, required splinting or straining, constipation, and pain with defecation. Women with anal sphincter defects may present with AI of flatus, liquid, or formed stool.
• Altered sexual functioning and body image: Patients may complain of dyspareunia, avoidance of intercourse, decreased libido, and decreased self-image.
• There are many validated and reliable questionnaires that can aid in eliciting a symptom history from patients, such as the Pelvic Floor Distress Inventory, the Pelvic Floor Impact Questionnaire, and the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire.
• Urinary diary: The patient records the volume and frequency of fluid intake and voiding as well as symptoms of frequency and urgency and episodes of incontinence over 24 hours, ideally for 3 days. This will allow the practitioner to better characterize the patient's symptoms as well as enable the patient to use it as a therapeutic tool to modify her behavior.
• A comprehensive physical examination should be performed at the first visit, including:
• A screening neurologic examination to evaluate overall mental status and sensory and motor function of the lower extremities.
• A pelvic exam, including a systematic evaluation of all components of the pelvic floor, including innervation, vulvar architecture, muscular and connective tissue support, and perineal scars. Particular attention should be given to urethral anatomy and hypermobility (see Q-tip test in the succeeding text). î Speculum exam, using a Sims speculum or the posterior blade of a Graves speculum, is helpful to
assess support, the presence of scarring, and any associated findings.
î The bimanual exam investigates the location, size, and tenderness of the bladder, uterus, cervix, and adnexa. The strength of the levator ani muscles is assessed by placing one or two fingers in the vagina and asking the patient to squeeze.
The firm muscular sling of the posterior puborectalis should be readily palpable.• Sacral nerve roots and the sacral reflex (also called the bulbocavernosus reflex) should be evaluated. When the clitoris or the area lateral to the anus is lightly scratched, an ipsilateral contraction of the anal sphincter should occur. In older patients, this reflex may be absent. In obese patients, this reflex may be difficult to evaluate.
• The Q-tip test evaluates urethral support. A cotton swab is placed in the urethra to the level of the urethrovesical junction, and the change in axis from rest to strain is measured to assess urethral hypermobility. Angular measurements of >30 degrees are generally considered hypermobile. Urethral hypermobility is thought to occur due to loss of integrity of the fibromuscular tissue that supports the bladder neck and urethra.
• A rectal examination can further assess pelvic pathology as well as evaluate the presence of fecal impaction. The exam should include an inspection of the perineal area for evidence of skin irritation or stool on the skin as well as digital examination of the anal sphincter for resting and squeeze pressure. One should also note the presence of a gaping anus or scarring.
• To evaluate POP, four specific anatomic components should be assessed: (a) anterior vaginal wall, (b) uterus and vaginal apex, (c) posterior vaginal wall, and (d) presence or absence of an enterocele. These compartments should be assessed with a standardized
P.409 system. The International Continence Society (ICS), American Urogynecologic Society, Society of Gynecologic Surgeons, and the National Institutes of Health recommend the standardized Pelvic Organ Prolapse Quantification (POPQ) system for grading support defects (Fig. 31-1). Many staging systems exist, but the POPQ system is widely accepted and published, easily learned, and reproducible. Additionally, pelvic muscle function can be assessed using scales such as Brink.
• The POPQ uses the hymen as a fixed point of reference and describes six specific topographic points on the vaginal walls (Aa, Ba, C, D, Bp, and Ap) and three distances (genital hiatus, perineal body, total vaginal length).
• The prolapse of each segment is measured in centimeters during Valsalva relative to the hymenal ring with points inside the vagina reported as negative numbers and outside as positive. The numeric values are then translated to a stage as described in Table 31-2.
• The perineal body is normally at the level of the ischial tuberosities. Descent of >2 cm below this level with flattening of the intergluteal sulcus indicates perineal descent.
• To fully evaluate POP, the patient may need to perform a Valsalva maneuver in lithotomy or strain while seated or standing while being examined by the provider. Pelvic floor muscle strength can be assessed, as outlined earlier.
• Examination of the anterior vaginal wall should include evaluation of the support of the urethra. With a speculum (or half of the speculum) used to depress the posterior vaginal wall, the patient is asked to
strain, and any descent of the anterior vaginal wall is noted.
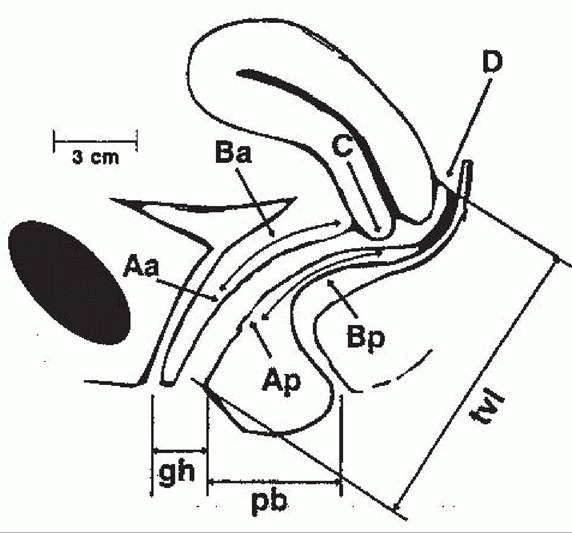
Figure 31-1. The Pelvic Organ Prolapse Quantification (POPQ) system components and anatomic reference points. For explanation of terms, see Table 31-2. (From Bent AE, Ostergard DR, Cundiff GW, et al, eds. OstergardS Urogynecology and Pelvic Floor Dysfunction, 5th ed. Philadelphia, PA Lippincott Williams & Wilkins, 2003:97, with permission.)
P.410
TABLE 31-2 Description and Staging of the Pelvic Organ Prolapse Quantification System
| Point/Distance | Description |
| Aa | Midline anterior vaginal wall, 3 cm proximal to the urethral meatus |
| Ba | Anterior vaginal wall, most distal point between Aa and anterior fornix (cuff) |
| C | Edge of the cervix (or vaginal cuff in posthysterectomy patients) |
| D | Posterior fornix. Not used in patients with hysterectomy |
| Ap | Midline posterior vaginal wall, 3 cm proximal to the hymenal ring |
| Bp | Posterior vaginal wall, most distal point between Ap and posterior fornix (cuff) |
Genital hiatus
Middle of the urethral meatus to posterior midline hymenal ring
Perineal body Posterior margin of genital hiatus to the middle anus
T otal vaginal Greatest depth of vagina with C or D reduced to its normal position
length
Staging of the POPQ system
Stage 0 Perfect support; Aa, Ap at -3. C or D within 2 cm of TVL from introitus.
Stage 1 Most distal portion of prolapse is -1 (or more negative) proximal to
introitus.
Stage 2 Most distal portion within 1 cm of the hymenal ring (between -1 and +1).
Stage 3 Most distal portion > +1 cm but 1/3 of void volume or >150 mL.
Cystourethroscopy can be used to assess the anatomy of bladder and urethra interior.
• Urodynamic studies can be used to assess the physiologic function of the bladder during filling and voiding. Simple cystometric testing can be performed in the office using a straight catheter and syringe to fill the bladder with a known volume of sterile water. At various bladder volumes, the patient is asked to cough and Valsalva in an attempt to demonstrate SUI or induce a detrusor contraction. Multichannel cystometrics, using one catheter in the bladder and the other either in the vagina or rectum, can be used for patients with complex symptoms or voiding complaints.
• Anorectal manometry provides quantitative information regarding function of the rectum, anus, and anal sphincter. It can also be used therapeutically in conjunction with biofeedback.
• Endoanal ultrasonography: The value of endoanal ultrasound lies in its ability to locate defects in the internal or external sphincter to facilitate planning for surgical correction.
• Magnetic resonance imaging can provide detailed soft tissue evaluation without radiation. This imaging modality may be useful if one suspects an enterocele that is not clearly palpable or if the patient's symptoms do not appear consistent with her anatomy on physical examination. It is also the gold standard for evaluating urethral diverticulum.
• Defecography: During a defecating proctogram, the patient's pelvis is imaged using fluoroscopy as she defecates while sitting after an enema is used to infuse contrast material. This test may be especially useful in patients with defecatory complaints.
• Anoscopy, proctoscopy, sigmoidoscopy, or colonoscopy may be indicated in patients in whom anatomic abnormalities are suspected, such as cancer or inflammatory bowel disease.
LOWER URINARY TRACT SYMPTOMS
Disorders of the lower urinary tract are categorized by storage or voiding symptoms. LUTS include overactive bladder and UI, described separately in the following text. For most LUTS, the first line of management is conservative. Definitions of some common LUTS include:
• Frequency—the complaint of voiding too often. In some populations, a cutoff for normal is seven voids during waking hours.
P.412
• Urgency—the complaint of a sudden compelling desire to pass urine that is difficult to defer. Urgency can occur with or without urge incontinence.
• Nocturia—the complaint of waking at night one or more times to void.
• Nocturnal enuresis—the complaint of loss of urine occurring during sleep.
Overactive Bladder
• Overactive bladder (OAB) is a clinical diagnosis to describe bothersome symptoms of urinary urgency with daytime frequency or nocturia, with or without urge incontinence. OAB often results from inappropriate detrusor contraction. When spontaneous or provoked involuntary detrusor contractions are demonstrated on urodynamic testing, OAB is referred to as detrusor overactivity (DO). DO may be neurogenic (associated with an underlying neurologic process) or idiopathic.
• The estimated overall prevalence of OAB in adult American women is 15% to 27%, which increases with age and in institutionalized women.
• T reatment of OAB includes the first-line methods of lifestyle modifications, behavioral therapy with pelvic floor physical therapy, and pharmacotherapy. If these methods provide unsatisfactory results, second-line methods can be tried. These therapies include sacral nerve stimulation, botulinum toxin A, and urinary diversion.
Lifestyle Modifications and Behavioral Management of Overactive Bladder
• Lifestyle modifications include weight loss, caffeine intake reduction, smoking cessation, and manipulation of daily fluid intake.
• Bladder retraining drills involve scheduled voiding with progressive increases in the interval between voids.
• Biofeedback is a form of patient reeducation in which a closed feedback loop is created so that one or more of the patient's normally unconscious physiologic processes is made accessible to her by auditory, visual, or tactile signals.
• Pelvic floor muscle exercise (PFME), requiring repeated voluntary pelvic floor muscle training (Kegel exercises), may be used in conjunction with bladder retraining.
• Functional electrical stimulation and weighted vaginal cones may be used during PFME although the evidence is unclear if there is additional benefit.
Medical Management of Overactive Bladder
• Oral and transdermal medications are available and can be combined with behavioral therapies to improve efficacy.
• Anticholinergics inhibit involuntary detrusor contractions and are the first-line pharmacotherapy for OAB due to their safety and efficacy. Dry mouth is the most common side effect. There are minimal differences found in efficacy or side effects between the various anticholinergics available. These medications are not recommended in patients with closed angle glaucoma or impaired gastric emptying.
î Of the five subtypes of muscarinic receptors, M2 is the most common in the bladder followed by M3.
î Oxybutynin (Ditropan) and tolterodine tartrate (Detrol) do not differ in outcomes. Oxybutynin is relatively selective for M3 and M1 receptors, and common side effects include dry mouth, constipation, blurred vision, and gastritis. Tolterodine tartrate targets M3 and M2 receptors and is better tolerated than the short-acting form of oxybutynin. In general, long-acting varieties are better tolerated but are more expensive.
P.413 î Anticholinergic medications with potentially fewer side effects are available. Trospium (Sanctura) is hydrophilic and theoretically does not cross the blood-brain barrier, limiting central nervous system side effects. Darifenacin (Enablex) binds to M3 receptors, whereas solifenacin (VESIcare) binds M3 and M1 relatively selectively and are thought to cause less frequent dry mouth, a principal reason for noncompliance with treatment.
• Tricyclic antidepressants such as imipramine improve bladder hypertonicity and compliance, suppressing involuntary detrusor contractions through multiple sites of action including Onuf nucleus.
î Mirabegron (Myrbetriq) is a beta3 agonist also used for the treatment of OAB symptoms. It relaxes the detrusor muscle during storage phase and increases bladder capacity by augmenting the sympathetic nervous system stimulation of the bladder.
Surgical Management of Overactive Bladder
• Surgical management of DO is reserved for intractable cases that have already failed multiple attempts at nonsurgical management. Procedures include sacral nerve root neuromodulation, augmentation cystoplasty, and urinary diversion via an ileal conduit. There is level I evidence supporting intradetrusor botulinum toxin injections in women with neurogenic and idiopathic DO; however, there is a high rate of associated urinary retention and UTI, as well as the need for repeat injections to maintain efficacy over time.
URINARY INCONTINENCE
The ICS defines UI as any involuntary leakage of urine. In the United States, the prevalence of UI in adult women is approximately 50%.
Types of Urinary Incontinence
• SUI, or urodynamic stress incontinence, is the most common type of UI among ambulatory incontinent women, accounting for 50% to 70% of cases. SUI occurs when abdominal pressure exceeds bladder pressure, for example, with coughing, sneezing, or laughing.
• Urge UI is involuntary leakage accompanied by or immediately preceded by the urge to void. Many patients complain of inability to reach the toilet in time. Involuntary detrusor contractions are typically the cause.
• Mixed incontinence describes symptoms of both stress and urge UI.
• Functional incontinence is associated with cognitive, psychological, or physical impairments that make it difficult to reach the toilet or interfere with appropriate toileting. A useful mnemonic is DIAPPERS: Delirium, Infection, Atrophy, Pharmacology, Psychology, Endocrinopathy, Restricted mobility, and Stool impaction.
• Bypass incontinence may be caused by urogenital fistulae or by congenital or acquired anatomic abnormalities.
• In the United States, gynecologic surgery is the most common cause of urogenital fistulae (0.1% of all hysterectomies). Other causes include radiation, trauma, and severe pelvic pathology. In developing countries, obstetric injuries are the most common cause. Patients often report painless and continuous vaginal leakage of urine, usually within the context of recent pelvic surgery (1 to 2 weeks). Instillation of methylene blue dye into the bladder will stain a vaginal pack if a
P.414 vesicovaginal fistula is present which can be confirmed on cystourethroscopy. Intravenous pyelography (IVP) or computed tomography scan can be performed to evaluate for possible ureterovaginal fistula. The preferred surgical route for correction of a vesicovaginal fistula is vaginal; however, in certain instances, an abdominal route may be optimal. The vaginal Latzko procedure is commonly used for postsurgical vesicovaginal fistulae. Treatment of ureterovaginal fistulae depends on location. Often, simply stenting the involved ureter can correct the fistula. If the ureterovaginal fistula persists and is close to the ureterovesical junction, ureteroneocystostomy can be performed. A psoas bladder hitch or Boari flap can be used to alleviate tension on this anastomosis. The interposition of vascular flaps may aid in the surgical success of fistula correction.
• Suburethral diverticulum is an outpouching of the urethra, and patients often complain of dysuria, recurrent UTIs, dyspareunia, and postvoid dribbling.
Treatment of Stress Urinary Incontinence
• Pharmacologic: The limited available medications for SUI are aimed toward increasing urethral sphincter tone. The efficacy for these interventions is unclear.
• Pelvic muscle exercise: Limited long-term prospective studies of this low-risk intervention suggest effectiveness, which is dependent on patient adherence.
• Continence pessaries: A prospective study comparing continence pessary to behavior therapy for SUI found that they have comparable results at 12 months (~50% satisfaction rate).
• Surgery: The etiology of SUI may be multifactorial and may not be completely corrected by surgery. Reported cure rates after surgery are usually high although can vary widely depending on parameters used to define cure of SUI. The most common techniques currently used for the treatment of SUI are retropubic colposuspension, suburethral sling, and urethral bulking agents.
Surgical Procedures for Stress Urinary Incontinence
• Retropubic urethropexy procedures are indicated for women with SUI and a hypermobile proximal urethra and bladder neck.
• The Burch retropubic colposuspension is a well-established surgery for SUI. Through a Pfannenstiel or Cherney incision, or laparoscopically, permanent sutures are placed in the fibromuscular tissue lateral to the bladder neck and proximal urethra, and the urethrovesical junction is supported by attaching these sutures to the iliopectineal line (i.e., Cooper ligament). Reported 5-year success rates have been over 80%.
• The Marshall-Marchetti-Krantz (MMK) procedure supports the bladder neck and urethra similar to the Burch, except the permanent sutures are placed through the periosteum of the pubic symphysis instead of Cooper ligament. This technique is seldom used now due to the risk of osteitis pubis.
• Suburethral slings are indicated for SUI with urethral hypermobility, although data also suggests some efficacy in patients with limited urethral mobility. The sling can be placed at the midurethra or bladder neck. It supports the urethra or bladder neck, providing static stabilization of the urethra at rest and dynamic compression of the urethra with increases in abdominal pressure. Suburethral slings can be created using various biologic and synthetic materials. The slings can be placed via retropubic versus transobturator approach. Cochrane analysis suggested improved cure rates compared to Burch at the cost, however, of a more invasive surgery.
P.415
• Tension-free vaginal tape (TVT): A polypropylene mesh is placed without tension at the midurethra through the retropubic space or space of Retzius. Success rates of TVT are similar to that of Burch colposuspension. Bladder perforation is the most common complication (5%), with bowel or vascular injuries being the most serious complications (both and when prolapse becomes bothersome. Risks of expectant management include vaginal epithelial erosion and persistence of LUTS and defecatory dysfunction.
• The nonsurgical approach may be useful in patients with a mild degree of prolapse, who desire future childbearing, have frail health, or are unwilling to undergo surgery.
• Pelvic floor muscle training (PFMT) or exercises (PFME), also known as Kegel exercises, can alleviate the symptoms of prolapse. These treatments have also been shown in small trials to reduce the anatomic severity of mild prolapse.
• Pessaries: The two basic types are supportive (most commonly a ring, with or without support) and space occupying (most commonly a Gellhorn). Pessaries can decrease symptom frequency and severity and delay or avoid surgery. Treatment with estrogen, either locally or systemically, may help the vaginal epithelium tolerate the foreign body. Because pessaries can cause vaginal wall erosion or ulceration and fistula formation, if neglected, patients should be examined routinely. Complications are minimized by avoiding excessive pressure on the vaginal epithelium and by emphasizing proper pessary care, including regular surveillance and cleansing. Serious complications are rare and more likely to occur in those who are unable to clean their pessaries regularly or who cannot come for routine cleaning visits. Risk factors for unsuccessful pessary fitting include a large genital hiatus and a short vaginal length.
• The goal of surgery is relief of prolapse symptoms. Overcorrection should be avoided because it can lead to new symptoms including LUTS or SUI. Although the uterus itself does not contribute to POP, most of the literature on prolapse surgery include hysterectomy concomitantly with POP repair to maximize the opportunity to correct apical support. The three categories of POP repair are obliterative, reconstructive, and compensatory.
Surgical Procedures for Pelvic Organ Prolapse
Reconstructive Procedures
• Abdominal sacral colpopexy replaces normal vaginal support with interposition of a suspensory bridge of mesh or graft between the apical anterior and posterior vagina with the anterior sacral promontory. Success rates are 78% to 100% for the
P.418 correction of apical prolapse. It has a lower rate of recurrence, dyspareunia, and is more durable than vaginal procedures such as sacrospinous ligament suspension. Its complications include rare intraoperative hemorrhage and a 3% to 4% prevalence of vaginal mesh erosion.
• Sacrospinous ligament suspension (SSLS) anchors the vaginal apex to the sacrospinous ligament, usually on the right side. This approach is faster, less expensive, and is associated with earlier return to daily activities than the abdominal procedures such as abdominal sacral colpopexy but has been shown to be not as effective. There is a 63% to 97% success rate. There are high rates of postoperative anterior vaginal prolapse, thought to be due to the pronounced posterior deviation of the vaginal axis (37%). Complications include hemorrhage, nerve injury, stress incontinence, dyspareunia, and buttock pain.
• Iliococcygeus fascia suspension, performed in patients who have suboptimal uterosacral ligaments, attaches the vaginal apex to the iliococcygeal fascia just below the ischial spine. Case-control studies report similar rates of success, complications, recurrence, and postoperative anterior vaginal prolapse as after SSLS.
• Uterosacral ligament suspension with fascial reconstruction suspends the apex of the vagina to the uterosacral ligaments, restoring the natural axis of the vagina. There is an 80% to 100% success rate. The most clinically relevant complication is ureteral kinking.
• Anterior colporrhaphy involves plicating the layers of the vaginal muscularis and pubocervical fibromuscular connective tissue to repair anterior prolapse (cystocele). The 5-year success rate is 30% to 40%. Complications include sexual dysfunction and dyspareunia.
• Posterior colporrhaphy is the plication of the pararectal and rectovaginal fibromuscular connective tissue over the rectum. Dyspareunia is common and occurs more frequently with posterior than anterior colporrhaphy.
• Defect-directed repairs isolate defects in the rectovaginal fibromuscular connective tissue and reapproximate normal anatomy.
• Perineorrhaphy is the reconstruction of the perineal body and attachment to the rectovaginal septum.
The goal is to build up the perineum, but it has been associated with subsequent dyspareunia.
• Enterocele, or herniation of bowel into or through the vagina, may occur after a previous hysterectomy.
Some recommend a preventative procedure concomitantly with any vaginal hysterectomy such as McCall culdoplasty that surgically obliterates the cul-de-sac at the time of vaginal hysterectomy and may prevent future enterocele. Once identified, an enterocele can be repaired by dissecting the bowel from the vaginal wall and endopelvic connective tissue and obliterating the cul-de-sac.
Obliterative Procedures
• Obliterative procedures include colpocleisis and colpectomy. They may be useful for older patients who do not desire future vaginal intercourse. The benefits include decreased complications, decreased surgical time, and high success rate (86% to 100%). A partial colpocleisis (LeFort) involves leaving the uterus in place with lateral drainage channels for cervical secretions. In a total colpectomy, the vaginal epithelium is removed and the vaginal vault tissue is reduced.
• Patients should be counseled regarding the risk of regret (5% to 10%), as the procedure precludes subsequent vaginal intercourse. If clinically indicated, preoperative evaluation can include a Pap smear, pelvic sonogram, or endometrial biopsy.
P.419
Compensatory Procedures
• When native tissue is weak or insufficient, compensatory procedures with graft/mesh placement/augmentation may be indicated. Biologic grafts can be native tissue, allografts (cadaveric tissue), and xenografts (porcine, bovine). The most commonly used synthetic mesh is type I polypropylene mesh.
• Anterior and posterior vaginal wall fibromuscular connective tissue replacement. Various graft materials and synthetic meshes have been used to augment vaginal prolapse repairs. The purpose of the graft is often twofold: via replacing the weakened or absent vaginal supports and acting as an absorbable “collagen scaffold” for fibroblast infiltration and scar formation. If the repair is too tight, the loss of flexibility can lead to fecal urgency and dyspareunia.
Use of Mesh in Vaginal Prolapse Surgery
• There are many mesh/graft “kits” for anterior and posterior repairs and for apical suspension. Although some of these procedures have resulted in decreased anterior vaginal prolapse recurrence when compared with vaginal restorative procedures without mesh/graft augmentation, the FDA issued a public health notification in July 2011 regarding adverse events related to transvaginal POP repair with mesh, including mesh erosion (10% within 12 months), pain, infection, urinary complaints, bleeding, and organ perforation. Therefore, these procedures should only be performed judiciously on selected patients who are thoroughly counseled regarding the data on efficacy and complications by surgeons especially trained to perform these types of procedures.
DISORDERS OF ANORECTAL FUNCTION
Anal Incontinence
• AI includes loss of voluntary control of flatus or stool (solid or liquid). Fecal incontinence (FI) is the loss of control over solid or liquid stool. AI can be a psychologically devastating and socially incapacitating condition.
Treatment of Anal Incontinence
• Nonsurgical treatment should be attempted with all patients before surgical reconstruction. Improvement is seen in 63% to 90% of patients. The first step is to eradicate treatable underlying causes, such as transient neurologic conditions, inflammatory bowel disease, fecal impaction, metabolic disorders, or offending diets.
• Environmental adjustments are necessary to decrease social isolation and anxiety and to improve quality of life.
• Skin care is important to prevent associated morbidities.
• Pelvic muscle-strengthening exercises and behavioral therapy: All patients should undergo a pelvic muscle training program before contemplating surgery.
• Pharmacologic agents that slow motility and reduce frequency (e.g., loperamide hydrochloride [Imodium], diphenoxylate hydrochloride [Lomotil]) may help some patients exercise more control over their stool.
• Dietary change: Increasing ingestion of natural fiber or the use of bulking agents, such as psyllium preparations (Metamucil), can change the consistency of stool, making it firmer and more easily controlled. Reduced caffeine intake will decrease colonic motility. A bowel diary can assist in eliminating offending foods.
P.420
• Surgical: Patients with FI should try nonsurgical treatment before pursuing surgical management. The procedures performed include end-to-end or overlapping sphincteroplasty, muscle transposition (neosphincter), artificial sphincter implantation, and colonic diversion. Sacral neuromodulation is FDA- approved for FI.
Constipation
• The Rome III criteria diagnoses constipation if the patient has at least 3 months of 2 or more of the following six symptoms: less than three defecations per week or 25% of defecations that involve straining, hard stools, sensation of incomplete evacuation or anorectal obstruction, or manual maneuvers to facilitate defecation.
• Constipation is not only a risk factor for pelvic floor disorders due to the chronic increase in intra-abdominal pressure, it is also a common symptom of pelvic floor disorders such as prolapse (rectocele). Some women will present with symptoms of AI due to constipation, as liquid stool escapes around impacted bowel contents.
• Management of constipation should be guided by the patient's history and physical exam. Initial options for treatment include behavior modification, changes in diet including increase in fiber intake, laxatives, or enemas. Defecatory dysfunction may respond to biofeedback or relaxation exercises, or botulinum toxin injections. If initial management is not successful, further evaluation may be necessary including imaging studies or referral to specialists.
SUGGESTED READINGS
American College of Obstetrics and Gynecology Committee on Practice Bulletins—Gynecology. ACOG practice bulletin no. 63: urinary incontinence in woman. Obstet Gynecol 2005;105(6):1533-1545.
American College of Obstetrics and Gynecology Committee on Practice Bulletins—Gynecology. ACOG practice bulletin no. 85: pelvic organ prolapse. Obstet Gynecol 2007;110(3): 717-729.
Abrams P, Andersson KE, Birder L, et al. Fourth International Consultation on Incontinence Recommendations of the International Scientific Committee: evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol Urodyn 2010;29(1):213-240.
Bradley CS, Zimmerman MB, Qi Y, et al. Natural history of pelvic organ prolapse in postmenopausal women. Obstet Gynecol 2007;109:848.
Hagen S, Stark D. Conservative prevention and management of pelvic organ prolapse in women. Cochrane Database Syst Rev2011 ;(12):CD003882.
Handa VL, Garrett E, Hendrix S, et al. Progression and remission of pelvic organ prolapse: a longitudinal study of menopausal women. Am J Obstet Gynecol 2004; 190:27.
Jelovsek JE, Maher C, Barber MD. Pelvic organ prolapse. Lancet 2007;369:1027.
Madoff RD, Parker SC, Varma MG, et al. Faecal incontinence in adults. Lancet 2004;364(9434):621-632.
Nygaard I, Barber MD, Burgio KL, et al. Prevalence of symptomatic pelvic floor disorders in US women. JAMA 2008;300:1311.
Swift S, Woodman P, O'Boyle A, et al. Pelvic Organ Support Study (POSST): the distribution, clinical definition, and epidemiologic condition of pelvic organ support defects. Am J Obstet Gynecol 2005;192:795.