Intra-amniotic infection, meconium staining of the amniotic fluid, and meconium aspiration syndrome: what is the link?
The fetus ingests and inhales the amniotic fluid as part of its normal behavioural state. Earlier studies of fetal sheep concluded that the egress of lung fluid was towards the amniotic cavity (58, 59), suggesting that the fetus could not aspirate amniotic fluid and therefore meconium.
However, recent ultrasound and colour Doppler studies have demonstrated clearly that there is an influx as well as efflux of fluid in the nasopharynx, the nose, and in the trachea (60-62). Fetal gasping has long been accepted as the precursor of meconium aspiration syndrome (MAS) and it has been described in the human fetus 24-72 hours before death in the absence of labour (63), in fetal lambs that died from antenatal infection, hypoxia, and other causes (64), and in primate fetuses before death (65). Therefore, we know that amniotic fluid can be inhaled in utero, especially when the fetus is in a pre-agonal state (65-68) and meconium has conclusively been demonstrated in the fetal lung of stillborn fetuses (69).The amniotic fluid is normally sterile and has antimicrobial activity, which helps it to protect the fetus against ascending microorganisms from the lower genital tract. However, meconium staining of the amniotic fluid (MSAF) facilitates the growth of bacterial species (70) by inhibiting the phagocytic ability of macrophages to ingest bacteria (71-73) and impairing oxidative burst and bacterial killing by polymorphonuclear leucocytes (74). This general rule does not apply to group B Streptococcus (GBS), which has the capability to grow and multiply rapidly within normal and clear amniotic fluid (70). If ascending microorganisms invade the amniotic fluid they may gain access into the fetal systemic circulation via the immature intestinal and/or pulmonary epithelium and elicit a fetal host inflammatory response. Fetal ingestion of amniotic fluid contaminated with microorganisms, bacterial products, and inflammatory mediators may elicit enteritis and enhanced colonic motility leading to discharge of meconium.
Patients with MSAF in spontaneous term labour have a higher frequency of positive amniotic fluid culture, a higher IL-6 concentration, more common Gram-negative bacterial isolates, and more frequent endotoxin assays, compared to those with clear amniotic fluid (75). The infected meconium discharged from the bowels contains microorganisms, bacterial products, inflammatory cytokines, and complements, and if inhaled into the lungs may induce local inflammatory damage within the lungs. However, a more generalized FSIRS may enhance this local effect and extend it to the pulmonary circulation, which ultimately may lead to persistent pulmonary hypertension (76-80) linking MSAF, intra-amniotic inflammation, funisitis, and MAS (81). The fact that these events leading to meconium aspiration are already established in utero and occur before birth explains the limited success of suction and clearing meconium out of the airway at birth to prevent MAS.Based on the available evidence, Romero et al. proposed that in utero aspiration of MSAF containing bacteria, endotoxin, and high concentrations of inflammatory mediators creates the conditions which predispose to MAS (75). MSAF is necessary but not sufficient to cause MAS. Approximately one of every seven pregnancies will have MSAF and only 5% of exposed infants develop MAS. A recent study found that newborns who developed MAS were exposed to significantly higher levels of intra-amniotic inflammation, and when the latter was associated with funisitis had a higher rate of MAS than their unexposed peers (RR 4.3; 95% CI 1.5-12.3). Of 89 newborns for whom amniotic fluid and placental histology were available, MAS was significantly more common in those with both intra-amniotic inflammation and funisitis than in those without intra-amniotic inflammation and funisitis while the rate of MAS did not differ between patients with intra-amniotic inflammation alone (without funisitis) and those without intra-amniotic inflammation and funisitis, suggesting that it is the fetal host response characterized by funisitis, which determines the outcome (81).
Clinical management
The obstetrician’s task is to manage the labour complicated by MSAF with the aim of preventing MAS if this has not occurred already. In practice, this involves continuous fetal heart rate (FHR) monitoring and avoiding intrapartum asphyxia of sufficient severity to induce MAS such as very prolonged bradycardia. Some obstetricians advocate routine fetal blood sampling to exclude fetal acidaemia if there was MSAF. This is unwarranted in the presence of a normal FHR pattern. Moreover, as discussed previously, a significant proportion of cases of MAS have normal or near normal acid-base status and have no signs of significant asphyxia and fetal blood sampling will be falsely reassuring under those circumstances. The majority of fetuses with MAS will exhibit a monotonous FHR pattern without fetal cycling activity or long- term variability and these patterns have recently been reviewed (82). Depending on the timing of the original insult, the baseline FHR may be raised or within the normal range and unless the fetus is acidaemic there may be no FHR decelerations associated with maternal contractions. Such babies should be delivered expeditiously to avoid exacerbation of the pre-existing injury. In some parts of the world amnioinfusion is deployed to dilute MSAF and reduce the frequency of variable deceleration but it has no impact on the risk of MAS if the fetus had continuous FHR monitoring. It also is associated with fetal and maternal infectious morbidity and therefore not recommended in the United Kingdom.
Intrapartum fetal monitoring in the presence of infection and MSAF
For the infected fetus, labour is markedly hazardous. The fetus is at risk of overwhelming intrauterine sepsis, or severe injury at lower levels of asphyxial insult, or both. Unfortunately, there are no consistent FHR patterns that predict fetal infection. However, FHR tachycardia is a sensitive marker of intrauterine infection and FSIRS especially when this is associated with MSAF in early labour where the risk of infection is 51-fold (83).
The same study showed a weak or no association with maternal tachycardia or maternal fever (83). There is no place for fetal blood sampling in the assessment of the infected fetus or one suspected to be infected. There are no significant differences in the mean arterial pH values of fetuses exposed to intrauterine infection and controls, however, the fetuses exposed to Abnormal vaginal flora and selected bacterial infectionsBacterial vaginosis
Bacterial vaginosis (BV) is an ecological disorder of the vagina characterized by varying degrees of depletion or total absence of the normally protective Lactobacillus species and an overgrowth of anaerobes (Figure 17.2). Over 60% of BV-positive women are asymptomatic (85) but the condition is associated with significant complications of pregnancy including late miscarriage, preterm delivery, preterm prelabour rupture of membranes, low birth weight, amniotic fluid infection, chorioamnionitis, and postpartum
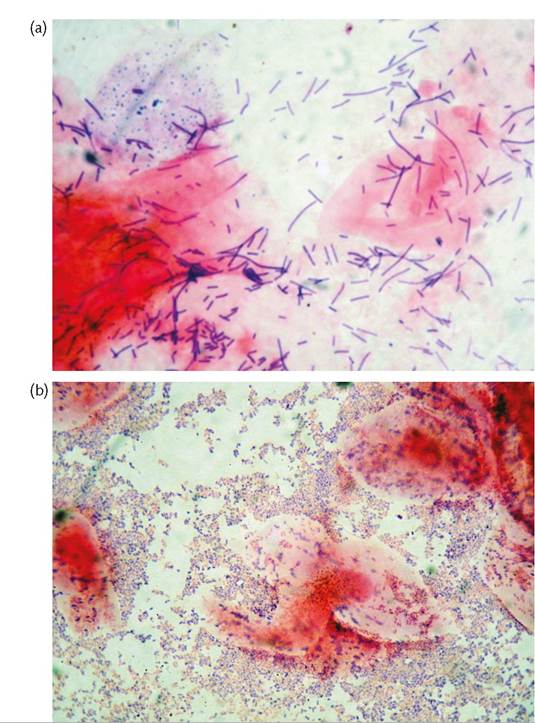
Figure 17.2 Gram stain of normal vaginal smear showing the dominant Lactobacillus species (a), and bacterial vaginosis showing a depletion of the protective Lactobacillus species and an increase in other bacterial species (b).
Reproduced from Ugwumadu A. Managing bacterial infections in pregnancy and the puerperium. The Prescribes, 2010,21(21):53-57 with permission from John Wiley and Sons.
endometritis. The role of screening for and treating BV in the general population of pregnant women at low risk of adverse pregnancy outcome is controversial. However, there is strong and persuasive evidence of benefit for screening and treating high-risk women with a prior history of late miscarriage or preterm delivery for BV (86, 87). When treatment is indicated in pregnancy, the authors prefer oral clindamycin because of its wider spectrum of activity against the range of organisms associated with BV, anti-inflammatory properties, and fewer recurrences after treatment, compared to metronidazole, which is an antianaerobe only.
There is consensus that symptomatic women should be treated, however, there is debate whether clindamycin is superior to metronidazole, what gestational age to initiate treatment, the optimal route of antibiotic administration, and the dosage and duration of therapy.Group B Streptococcus
Approximately 20-30% of pregnant women are GBS carriers, with higher rates of colonization in black than in white or Asian women (88). It emerged in the 1970s as the leading cause of neonatal sepsis and trials showed that intravenous (IV) penicillin or ampicillin during labour prevented neonatal disease (89), in contrast to antenatal eradication of genital GBS colonization before labour (90, 91). There are no efficacy data on oral or intramuscular antibiotic prophylaxis during labour.
Prevention of early-onset neonatal GBS disease
Two competing strategies for the prevention of early-onset neonatal GBS disease (EOGBSD) are widely recognized, the cheaper but less effective one is the treatment of women with known risk factors for EOGBSD, namely intrapartum fever (20% of GBS-positive women), preterm labour, prolonged rupture of membranes (≥18 hours), GBS bacteriuria, previously affected infant, and isolation of GBS at any other time; the other is a culture-based screening of all women before labour (35-37 weeks in practice) to identify and offer intrapartum antibiotic prophylaxis to those colonized by GBS. Implementation based on this resulted in a nationwide reduction of 70% in the incidence of EOGBSD (from 1.5-2 cases/1000 live births to 0.5 cases/1000 live births) in the United States (92). However, a subsequent large, retrospective cohort study showed that late antenatal culture-based screening was over 50% more effective in reducing the EOGBSD than the risk-based approach (93), leading to its adoption (94). The improvement may be related to the detection and treatment of the 20% of colonized women who do not display any risk factors. For optimal detection rates (up to 27%), a rectovaginal or vaginal/perianal swab inoculated into a selective medium was recommended in addition to intrapartum treatment of women who have had a previously affected infant, GBS bacteriuria, or whose GBS status was unknown.
Intrapartum antibiotic prophylaxis and risk of resistant organisms
The recommended regimens for intrapartum antibiotic prophylaxis include penicillin G, 5 million units IV initially followed by 2.5 million units every 4 hours until delivery, or ampicillin 2 g IV initially, then 1 g IV every 4 hours until delivery. Patients who are allergic to penicillin but not at risk of anaphylaxis should receive cefazolin 2 g IV initially, then 1 g IV every 4 hours until delivery, or either clindamycin 900 mg IV every 8 hours or erythromycin 500 mg IV every 6 hours until delivery, if they were at risk of anaphylaxis. At present, GBS remains universally sensitive to penicillin and the narrow spectrum of penicillin G drives the mistaken belief that there is less selective pressure for the emergence of resistant organisms. However, recent studies have shown that intrapartum administration of both benzylpenicillin and ampicillin was associated with a 35% increase in vaginal colonization with ampicillin-resistant Enterobacter species, 36 hours postpartum (95). One large study found a significant increase in the rate of early-onset Escherichia coli sepsis, although this was restricted to low-birthweight neonates (96, 97), and the total Gram-negative bacterial sepsis declined despite the increase in E. coli infections.
Some clinicians wrongly presume that clindamycin and erythromycin are automatically effective as prophylaxis for GBS in women who are sensitive to penicillin but the frequency of strains of GBS which are resistant to erythromycin (currently 47%) or clindamycin (15%) is rising. Vancomycin 1 g IV every 12 hours until delivery is recommended if the susceptibility was unknown. Clinicians should request sensitivity studies when taking samples for possible GBS colonization from women who volunteered a history of penicillin allergy. The risk-based approach, associated with a 55% reduction in the incidence of EOGBSD, is adopted in the United Kingdom. It is noteworthy that the baseline incidence of EOGBSD in the United Kingdom is estimated at 0.5-1.15/1000 live births (98) in contrast to the 1.5-2.5/1000 rate in the United States prior to the introduction of mass screening in late pregnancy. The introduction of screening for the prevention of EOGBSD in the United Kingdom may not be appropriate or cost-effective. The current United Kingdom NICE guidelines do not recommend intrapartum antibiotic prophylaxis for women with prolonged rupture of membranes (≥24 hours) or their babies, if there is no evidence of infection such as pyrexia in labour (http://www.nice.org.uk/CG55). This is a significant deviation from current understanding of the risk factor-based approach to the prevention of EOGBSD, particularly as 20% of colonized women do not display any risk factors.
Gonorrhoea
Gonorrhoea is a sexually transmitted infection caused by Neisseria gonorrhoeae, a Gram-negative diplococcus bacteria.
Epidemiology
Gonorrhoea is spread by contact with the penis, vagina, mouth, or anus. The incidence of newly diagnosed gonorrhoea in the United Kingdom increased by 6% from 16,629 cases in 2008 to 17,385 cases in 2009 (99-101). Some of the risk factors associated with infection include young age, previous sexually transmitted infections, inconsistent condom use, drug abuse, and new or multiple sexual partners. N. gonorrhoeae may infect the genitourinary tract, rectum, pharynx, or eye. Spread of infection to the upper genital tract can cause pelvic inflammatory disease. The perinatal implications include transmission to the neonate causing conjunctivitis and blindness if untreated. Disseminated infections may cause septic arthritis, endocarditis, and meningitis. Pregnant women are at greater risk for disseminated infection than non-pregnant women (101).
Clinical diagnosis
In most cases, gonorrhoea is asymptomatic but some women may complain of dysuria or mucopurulent vaginal discharge. Screening women at high risk for sexually transmitted infections is essential for infection control. Pregnant women should be screened at the first prenatal visit if they are at risk or if there is a high rate of gonorrhoea in the population (101). Patients who continue to be at high risk should be screened again in the third trimester. Although Gram stain of the endocervical fluid has a high positive predictive value, diagnosis is usually made by culture, nucleic acid hybridization, or nucleic acid amplification tests (NAATs) of samples obtained from the endocervix, vagina, male urethra, or urine. The patient should be evaluated also for other sexually transmitted infections including chlamydia, syphilis, and human immunodeficiency virus (HIV), and have all their sexual contacts traced and offered treatment.
Treatment
Due to spread of resistant strains of bacteria, the recommended regimens for uncomplicated urogenital and anorectal gonorrhoea include single-dose intramuscular ceftriaxone 250 mg or oral cefixime 400 mg with treatment for chlamydia if the latter has not been excluded (102). Alternative regimens include single-dose intramuscular spectinomycin 2 g or cefotaxime 500 mg. Cefpodoxime 400 mg and cefuroxime axetil 1 g have been suggested as oral alternatives. For disseminated infection, ceftriaxone 1 g intramuscularly or IV every 24 hours is recommended; alternative regimens include cefotaxime 1 g IV every 8 hours or spectinomycin 2g intramuscularly every 12 hours. Treatment should be continued for 24-48 hours after clinical improvement and then continued with cefixime 400 mg orally twice daily or cefpodoxime 400 mg orally twice daily to complete 1 week of therapy. Pregnant women should not be treated with fluoroquinolones or tetracyclines. It is good practice to treat empirically for chlamydia infection even if this has not been tested for, as concurrent infection is frequent.
Syphilis
Syphilis is a sexually transmitted infection caused by the spirochete Treponema pallidum. Without treatment the disease progresses through different stages over time. Syphilis may cause miscarriage, stillbirth, hydrops, polyhydramnios, or fetal abnormalities.
Epidemiology
In 2001, the World Health Organization estimated that 12 million new cases of syphilis occurred in adults per year across the globe (103). There has been a recent resurgence of syphilis in developed countries after many years of low seroprevalence. For example, a rapid increase of infectious syphilis occurred in the United Kingdom between 1999 and 2008 mostly among men who have sex with men (104). This was attributed to increased IV drug misuse and HIV infection. Risk factors associated with infection include multiple sexual partners, drug abuse, poor socioeconomic status, and young age.
Vertical transmission results in more than 1 million infants born with congenital syphilis annually worldwide (105). Rates of perinatal transmission of infection vary depending on the stage of maternal disease—almost 100% if the fetus is exposed to the chancre during delivery in primary syphilis, 50% during secondary syphilis as a result of transplacental infection, 40% during early latent disease, and about 10% during late latent and tertiary syphilis (106). Vertical transmission is decreased to 1-2% in women who are adequately treated during pregnancy.
Clinical diagnosis
The infection has a long natural history progressing through recognized stages:
1. Primary syphilis—this is characterized by the chancre (a raised, indurated, exudative, and painless ulcer) at the site of entry of the spirochete. There may be non-tender regional lymphadenopathy (bubo). The chancre usually resolves spontaneously within 3-6 weeks even without treatment. The incubation period averages 3 months but may lie between 3 and 90 days depending on the size of the inoculum at infection.
2. Secondary syphilis—this is the stage during which the spirochetes become systemic and begins from about 6 weeks and may last up to 6 months after initial infection. It is seen in about 25% of untreated individuals. Clinical signs include extensive maculopapular rash particularly involving the palms and soles, lymphadenopathy, and genital condyloma lata.
3. Latent syphilis is the diagnosis of asymptomatic infection documented with positive serology but absent manifestation on physical examination. If this occurs within 1 year of inoculation it is called early latent; if the diagnosis occurs after 1 year or cannot be determined, it is defined as late latent syphilis.
4. Tertiary (late) syphilis occurs after the initial stages of syphilis and the onset may vary from 1 year to 30 years after the initial inoculation. It is slowly progressive and may involve the central nervous system, the cardiovascular system, or the skin and subcutaneous tissues. The typical lesion of tertiary syphilis, the gumma, is an area of chronic inflammatory destruction presenting as an indolent lesion with a necrotic centre. Gumma may be single or multiple and are variable in size from microscopic to large tumour-like areas. They have a predilection for the skin, liver, bones, and spleen.
Congenital syphilis occurs via transplacental transmission of T. pallidum to the fetus and can occur at any time during pregnancy. Congenital transmission is extremely high during the first 4 years after inoculation. It may result in intrauterine growth restriction, intrauterine fetal demise, neonatal death, preterm birth, and congenital infection and anomalies.
Diagnosis of primary or secondary syphilis can be made with dark-field microscopy and direct visualization of spirochetes or serological testing. Serological tests remain the method of choice for diagnosis. The Venereal Disease Research Laboratory (VDRL) test and rapid plasma reagin (RPR) tests are simple and inexpensive with high sensitivity during early infection (106). Specific treponemal serological tests include fluorescent treponemal antibody absorption (FTA-ABS), the microhaemagglutination test for antibodies to T. pallidum (MHA-TP), and the T. pallidum particle agglutination assay (TPPA). False-positive results may occur with both non-treponemal and treponemal methods, therefore single-test syphilis diagnosis is inadequate. A false-positive result is associated with febrile illness, immunizations, autoimmune conditions particularly systemic lupus erythematosus, IV drug use, chronic liver disease, and HIV infections. Yet other tests for detecting syphilis include direct fluorescence antibody testing (DFA-TP) and multiplex polymerase chain reaction (PCR). Cerebrospinal fluid analysis via lumbar puncture is essential in anyone with latent syphilis, oph- thalmic/neurological signs or symptoms, treatment failure, coexistent HIV infection, and active tertiary syphilis.
Screening for syphilis is recommended at the first prenatal visit, and repeated during the third trimester and at delivery for patients at high risk. If positive for VDRL, further specific tests from a reference laboratory should be arranged along with referral to a specialist in genitourinary medicine. During pregnancy, ultrasonography can be used to determine the extent of fetal disease during the second half of pregnancy. If there are ultrasonographic signs of fetal disease such as hepatosplenomegaly or hydrops fetalis, a multidisciplinary team including genitourinary medicine and perinatology/fetal medicine specialists should be consulted. An abnormal ultrasound scan is an indication for antepartum FHR monitoring prior to instituting antibiotic treatment. Sonographic signs of fetal syphilis combined with an abnormal FHR pattern may indicate a severely affected and possibly moribund fetus (103).
Treatment
Penicillin continues to be the gold standard treatment for syphilis in and outside of pregnancy. Treatment is effective for maternal disease, prevention of vertical transmission to the fetus, and eradication of early fetal disease. Primary syphilis may be treated with a single dose of penicillin G (benzathine 2.4 million units intramuscularly). In all other cases, the disease should be considered latent and of unknown duration and treated with a course of three intramuscular injections of penicillin G (benzathine 2.4 million units) spaced a week apart. An alternative treatment regimen is daily intramuscular inj ections of procaine penicillin (0.6-0.9 million units) for 10-14 days. Neurosyphilis requires aqueous crystalline penicillin G between 12 and 24 million units daily in divided IV doses for 10-14 days.
Treatment of maternal syphilis is complicated in pregnant woman with a penicillin allergy (5-10% of cases). Confirmation of the penicillin allergy with skin testing is recommended, unless there is a documented anaphylactic reaction. In this situation, penicillin desensitization followed by penicillin treatment is the next treatment option of choice. Oral penicillin desensitization is given in small, gradually increasing doses with inpatient monitoring over approximately 4 hours, followed by the administration of the therapeutic dose intramuscularly 30 minutes after completion. Most adverse reactions can be managed supportively without discontinuation of the desensitization protocol. The Jarisch-Herxheimer reaction is a common systemic reaction to the treatment of syphilis occurring in approximately 40-45% of pregnant women, during the first course of penicillin (107). It is thought to result from the release of an endotoxin-like substance when a large number of spirochetes are killed by the antibiotics. The Jarisch-Herxheimer reaction is characterized by headache, pyrexia, malaise, rash, tachycardia, and hypotension usually 1-12 hours after the administration of an initial antibiotic dose and should be managed supportively. It may precipitate FHR abnormalities and/or preterm labour, therefore fetal monitoring is recommended (108). However, the reaction is usually not seen with subsequent antibiotic doses. The therapeutic response to treatment should be followed up with serological testing at 1-, 3-, 6-, 12-, and 24-month intervals.
Treatment of the baby at birth is recommended if maternal treatment was with alternative antibiotics such as macrolides. If delivery occurred within 30 days of treatment completion, the neonate needs empirical treatment (108). The neonatologists should be informed before delivery of the baby so that appropriate examination, management, and follow-up may be arranged for the neonate. If the neonate's serum is negative on screening and there are no signs of congenital syphilis, no further testing is necessary and the mother can be reassured. About 75% of infected babies may not show any symptoms at birth with signs of congenital syphilis manifesting many weeks, months, or years after birth. These can present as skin lesions, snuffles, hepatosplenomegaly, lymphadenopathy, and failure to thrive (108). Women diagnosed with syphilis should be offered testing for other sexually transmitted infections including HIV infection and their sexual contacts traced and offered treatment.
Listeriosis
Listeriosis is a rare infection caused by the bacterium Listeria monocytogenes, a Gram-positive, rod-shaped organism, which may contaminate raw food such as soft cheese, cured meat, and prepacked raw items such as smoked fish, sandwiches, or salads. Infection occurs when contaminated food is ingested.
Epidemiology
The incidence of listeriosis in pregnancy is 12 per 100,O0O compared with a rate of 0.7 per 100,O0O in the general population (109). Infection is mostly seen in neonates, however, listeriosis is 20 times more likely in pregnancy and 300 times more likely with acquired immunodeficiency syndrome (AIDS) (110). Elderly and immunocompromised individuals are at high risk of infection. Neonatal infection is caused mainly by vertical transmission of maternal infection via the placenta or occasionally as an ascending infection to the fetus.
Clinical diagnosis
In immunocompetent individuals, infection is often asymptomatic or presents as acute fever and gastroenteritis with full recovery within 2 days. Maternal symptoms include fever, malaise, headache, sore throat, conjunctivitis, abdominal or back pain, diarrhoea/ vomiting, stiff neck, and confusion. Among pregnant women, about 20-30% of cases may result in stillbirth or neonatal death, and miscarriage is common (110). (111). Seventy per cent of pregnancies with listeriosis result in preterm delivery below 35 weeks' gestation and about 66% of infants surviving a pregnancy complicated by listeriosis will have neonatal listeriosis (112). Mortality in the infected neonate is 30-50%.
Pregnant women with listeriosis may show signs of chorio- amnionitis such as uterine fundal tenderness, contractions, fever, vaginal discharge, or ruptured membranes. Early-onset neonatal disease (and microcephaly or hydrocephaly (117). The diagnosis of primary CMV infection is by the demonstration of seroconversion of CMV-specific immunoglobulin (Ig)-G antibodies from negative to positive (117). A rise of IgG titre is not useful as this can also occur with recurrent infection.
Diagnosis of primary maternal CMV infection in pregnancy should therefore be based on the de novo appearance ofvirus- specific IgG in the serum of the pregnant woman who was previously seronegative or on detection of specific IgM antibody associated with low IgG avidity. IgM specific to CMV is not a reliable marker for diagnosis of primary infection because the CMV IgM, though suggestive of recent infection, can remain positive for many months. IgM can also indicate reactivation of past infection (118). The diagnosis of secondary infection should be based on a significant rise of IgG antibody titre with or without the presence of IgM and high IgG avidity.
Ultrasound scan findings of microcephaly, hepatosplenomegaly, ventriculomegaly, calcifications of the brain, liver, or placenta, intrauterine growth restriction/oligohydramnios, ascites, pericardial or pleural effusion, hypoechogenic bowel, and/or hydrops may raise suspicion of fetal infection. Amniotic fluid culture for CMV or PCR for DNA identification should be offered to pregnant women with documented primary CMV infection or sonographic findings suggestive of CMV infection. A high CMV viral load in the amniotic fluid is associated with a higher risk of an affected fetus (119).
Treatment
At present there is no therapy for the in utero treatment of primary infection. There is also no CMV vaccine available at the present time. Routine screening for CMV infection in pregnancy is not recommended. Antenatal management options include counselling followed by either expectant management or termination of pregnancy. Termination of pregnancy should be offered if a significant CMV viral load is confirmed on prenatal testing. Specific treatment strategies such as therapies with adenosine arabinoside, cytosine arabinoside, ganciclovir, and foscarnet have been used for severe clinical infection (119). In view of their toxicity profiles, advice should be sought from perinatal infection specialists prior to using these agents. Research studies are exploring the use of CMV-specific IV immunoglobulins in affected pregnancies.
Rubella
The rubella virus is an RNA virus of the Togaviridae family. The infection is also known as German measles.
Epidemiology
Prior to the introduction of the rubella vaccine the infection was seen mainly in children of school age but the incidence in most countries has fallen in recent times with the introduction of the vaccine (120). The number of women of reproductive age who remain susceptible varies widely between countries as rubella vaccine is not universally available. Rubella infection during pregnancy may lead to intrauterine fetal demise, miscarriage, fetal growth restriction, hydrops, or congenital rubella syndrome characterized by sensorineural deafness, cataracts, glaucoma, chorioretinitis, microphthalmia, patent ductus arteriosus, peripheral pulmonary artery stenosis, atrial or ventricular septal defect, microcephaly, meningoencephalitis, and intellectual disability (121). Other associations include hepatosplenomegaly, thrombocytopenia, bone defects, and purpuric skin lesions resulting in the classic ‘blueberry muffin' presentation.
Clinical diagnosis
In most of the developed world, pregnant women are routinely screened for immunity to rubella and advised to avoid contact with rubella if they are non-immune. Evaluation for rubella infection should be done in susceptible pregnant women if clinical features consistent with rubella infection occurred or following exposure to an active case. Rubella causes a febrile illness with transient rash, fever, arthralgia, and postauricular and suboccipital lymphadenopathy. The rash often migrates from the face to the rest of the body. The incubation period is 12-24 days. Complications of rubella infection include encephalitis, myocarditis, pericarditis, hepatitis, and thrombotic thrombocytopenic purpura/haemolytic uraemic syndrome. The risk of fetal anomaly is over 90% with infection before 11 weeks of pregnancy, dropping down to the background risk after 20 weeks (105). Serology is the usual method for the diagnosis of rubella infection. It involves the detection of specific IgM antibodies or a significant rise in specific IgG titres. If recent infection is suspected, rubella IgM and rubella-specific IgG avidity may be used to confirm primary infection. Fetal infection may be confirmed by testing for viral DNA in a chorionic villus sample in the first trimester or by PCR of the amniotic fluid or fetal blood.
Treatment
If fetal infection is confirmed at an early stage, termination of pregnancy should be offered as an option. Management is limited to supportive care since there is no specific treatment available.
Rubella vaccine is available as a single live attenuated vaccine or in combination with the measles and mumps vaccine (MMR). It should be offered to all non-immune and seronegative women of reproductive age outside of pregnancy. Vaccination should be offered to non-immune women post delivery and they should be advised to avoid pregnancy for 3 months after vaccination. There is no contraindication to breastfeeding with the vaccine. Approximately 5% of women may not respond to the vaccine and remain susceptible to rubella (105).
Measles (rubeola)
Measles is an acute, highly infectious illness caused by the rubeola virus and is transmitted via droplet infection. The virus belongs to the Paramyxoviridae family, which are enveloped negative singlestranded RNA viruses.
Epidemiology
Although measles is highly contagious, the infection is uncommon in industrialized nations because of a safe and effective vaccine (122). The disease remains one of the leading causes of death among young children globally. In 2015, there were 134,200 measles deaths globally—about 367 deaths every day or 15 deaths every hour (122). Most epidemics occur in the spring and summer of alternate years. The spread of infection occurs by direct contact with droplets from respiratory secretions of infected persons.
Clinical diagnosis
The incubation period following exposure is 10- 14 days. Exposure to the virus results in entry via the respiratory mucosa and/or conjunctiva. There may be transient respiratory symptoms, fever, or a rash during this period. There is a prodromal phase of 2-4 days followed by fever, conjunctivitis, coryza, and Koplik’s spots (white, irregular lesions on the buccal mucosa opposite the upper premolars) on day 2 of the fever. By day 3 to 4, an erythematous maculopapular rash appears starting initially at the forehead, and behind the earlobes moving to the trunk and feet by the third day. The early lesions become confluent, although peripherally, the lesions remain discrete. It begins to fade by the third day in the order of its appearance.
Most measles-related deaths are caused by complications associated with the disease including disseminated disease and pneumonia. Post-infectious encephalitis can occur in 1 in 800-1600 cases. It has a mortality rate of up to 15% with neurological sequelae in half of the survivors (123). Subacute sclerosing panencephalitis is another rare (1 in 100,000 cases) late-appearing complication occurring most often in children (123). Measles during pregnancy is associated with increased maternal mortality secondary to pneumonia. Hence women with suspected pneumonia should be referred to a tertiary centre (105). Measles infection in pregnancy increases the risk of preterm birth and fetal growth restriction (105). Serum testing for measles- specific IgG and IgM antibodies is utilized for the confirmation of acute infection.
Treatment
Measles usually runs a self-limiting course, resulting in full recovery with supportive therapy such as hydration and antipyretics. Secondary bacterial infections (otitis or pneumonia) should be treated appropriately as soon as a diagnosis is made. Live attenuated measles vaccine is highly effective in controlling epidemic disease as well as the rare neurological sequelae (123). Two doses of the vaccine are recommended to ensure immunity and prevent outbreaks. In non-immune women of childbearing age, two doses of MMR vaccine can be given separated by a 3-month interval. In susceptible exposed women, passive immunization with pooled immunoglobulins may be offered within 72 hours of exposure as postexposure prophylaxis.
Parvovirus
Parvovirus B19 is a DNA virus of the Parvoviridae family. It causes erythema infectiosum or ‘fifth disease’. Outbreaks usually occur in nurseries or schools with seasonal peaks.
Epidemiology
Parvovirus B19 infection is common among school children and 60% of women are immune to it by the age of 20 years (124). The cellular receptor for B19 parvovirus is the erythrocyte P antigen, thus its main target is erythroid progenitor cells. The infection is spread via respiratory secretions. Mothers, nursery teachers, and health workers who come in contact with school-aged children are at highest risk of contracting the infection. The virus is also transmissible via blood and blood products. There is a 50% risk of transmission from an infected mother to her fetus in utero (125).
Clinical diagnosis
Parvovirus B19 infection is characterized by a flu-like illness (fever, malaise, arthropathy, and lymphadenopathy) followed by a malar rash with the characteristic ‘slapped cheeks’ appearance and a lace-like rash in the extremities. The rash may reappear for several weeks following stimulus, including changes in temperature, sunlight exposure, or emotional stress. While in some cases, the infection may be asymptomatic, in others, the symptoms may persist for several months. Fetal infection may be asymptomatic or result in serious consequences such as miscarriage or fetal loss (10-15%) or hydrops fetalis (3-10%) as a result of haemolytic anaemia and congestive cardiac failure (126). If infection occurs after 20 weeks’ gestation, the fetal loss rate is 2% (124). Spontaneous recovery of hydropic fetuses with delivery of normal infants has been reported (127).
Serological testing with enzyme-linked immunosorbent assay (ELISA) to detect IgG and IgM antibodies to B19 parvovirus may be used for diagnosis. Susceptible individuals will have negative status to both antibodies. A positive IgG and negative IgM suggests immunity or infection of more than 120 days prior. Recently infected patients will have positive IgM and negative IgG, and, finally, those who have had an infection more than 7 days but less than 120 days prior will show seropositivity to both G and M immunoglobulins. DNA detection by PCR is the other diagnostic test available. If primary infection during pregnancy is confirmed, serial fetal ultrasound scans should be offered starting from 2 to 4 weeks after infection or seroconversion to detect any hydrops fetalis. Monitoring by scanning should continue every 1-2 weeks until 34 weeks of pregnancy.
Treatment
Maternal treatment is just supportive care since the infection is self-limited. Cordocentesis and intrauterine transfusion are recommended if hydrops occurs, and fetal medicine specialists should be involved in the care. If hydrops has not occurred by 8 weeks after maternal infection, it is unlikely to occur (127). Parvovirus B19 infection is not associated with congenital anomalies in the fetus and there is no indication for therapeutic termination of pregnancy. Currently, routine screening for infection is not justifiable and no prophylaxis or vaccine is available.
Herpes simplex virus
Over 70% ofprimary genital herpes infections pass asymptomatically. Recurrent episodes tend to be milder in severity and shorter in duration than the primary infection. Transmission of herpes simplex virus (HSV) from mother to child around the time of delivery can cause potentially fatal disease in the newborn; however, routine antenatal screening for the detection of HSV 1 and 2 in the cervix, or antibodies from patients with a history of recurrent HSV, is not recommended. Therefore, if genital herpes infection is suspected, it is essential to determine whether the infection is primary or a recurrence and establish the gestational age of the pregnancy. Women who suffer their first genital HSV infection during pregnancy are at the highest risk of transmitting the virus to their newborn. Efforts to prevent vertical transmission of HSV disease may be summarized as follows:
1. Prevention of acquisition of maternal genital HSV infection.
2. Prevention of transmission of HSV during pregnancy and delivery.
3. Prevention of disease in an exposed newborn postnatally.
At the present time, there is no vaccine licensed to prevent genital herpes, although a number of clinical trials are ongoing. The potential role of intrapartum antiviral therapy and postnatal strategies
to prevent neonatal HSV disease is yet to be determined. Oral aciclovir and valaciclovir given prophylactically in late pregnancy have been shown to reduce recurrences of genital herpes, shedding of HSV at delivery, and is the mainstay of prevention of HSV acquisition (128). There is insufficient evidence to determine the effect of antiviral prophylaxis in pregnancy on neonatal HSV disease. Neonatal HSV disease should always be treated with systemic antiviral therapy. Opinion is still divided on the use of caesarean section for the management of recurrent HSV. If the infection is primary, the woman should be referred urgently to the local sexual health clinic. A primary episode of HSV at 34 weeks' gestation or more but before the onset of labour is managed with prophylactic aciclovir until delivery. However, a primary episode in labour is managed by caesarean section provided the membranes have not been ruptured for more than 4 hours. If the interval between initiating prophylactic antiviral therapy and delivery is more than 4 weeks, vaginal delivery is appropriate. With infections prior to 34 weeks, aciclovir should be started from 34 weeks until delivery with the aim of vaginal delivery.
Varicella zoster virus
Varicella zoster virus (VZV) is the cause of chickenpox, a highly contagious infection. Like other viruses in the herpes family the infection is characterized by an acute illness, which is followed by the persistence of the virus within body tissues where they lie dormant for prolonged periods of time and may become reactivated subsequently. The zoster virus persists in the dorsal root ganglia of the spinal cord from where reactivation may give rise to shingles long after the primary infection.
Epidemiology
Over 90% of the antenatal population in the United Kingdom have had chickenpox infection, usually as a mild self-limiting illness in childhood, which confers lifelong immunity. As a result, the incidence of chickenpox in pregnancy in the United Kingdom is low, estimated to be 3 per 1000 (129). In contrast, the infection is usually acquired at older ages in the tropics resulting in higher susceptibility among adults from those populations. Therefore, immigrant women from tropical countries are at a greater risk of chickenpox infection than their counterparts who grew up in the United Kingdom (129, 130).
Clinical diagnosis
The infection is transmitted via respiratory droplets. The symptoms include malaise, fever, pruritic maculopapular rash, vesicles, crusts, and lesions at different stages of healing. If the infection is suspected or diagnosed, the woman should avoid contact with other pregnant women, immunosuppressed patients, and neonates for more than 5 days, or until the lesions crust over. Pregnant women are at greater risk of pulmonary complications particularly if they smoked, had chronic lung disease, took immunosuppressant drugs, had over 100 vesicles, or are in the second half of pregnancy. Other maternal complications include hepatitis, encephalitis, acute cerebella ataxia, thrombocytopenia, purpura, and haemorrhagic gangrene. These women and those with mucosal lesions or new lesions after 6 days should be referred urgently to the hospital. Shingles is usually mild and there is no risk to the fetus or neonate. Viraemia is rare with shingles unless in the immunocompromised host. Since the introduction of antiviral therapy, mortality from VZV pneumonia in pregnant women has become rare (130).
Risk assessment and prevention
Susceptible pregnant women should avoid contact with people with chickenpox and report any potential exposure. If a pregnant woman presents with a history of significant contact with chickenpox (defined as living in the same household, being in the same room for ≥15 minutes, face-to-face conversation for >5 minutes with someone who has chickenpox or shingles in an exposed part of the body, or any contact with a case of chickenpox during the period of ‘infectiousness') immunity should be assumed if she gives a definite history of chickenpox (130). However, an urgent VZV IgG assay should be ordered if the history is negative or vague. Immunity (VZV IgG) can also be determined on the booking serum sample. Varicella zoster immunoglobulin (VZIG) should be administered as soon as possible (up to 10 days) if a woman with significant exposure is found to be non-immune. VZIG has no therapeutic benefit once chickenpox has developed and it does not prevent intrauterine infection. The woman should be referred to the fetal medicine unit between 16 and 20 weeks or 6 weeks after the infection for ultrasound scan assessment (130). After birth, the infant should undergo ophthalmic assessment and VZV IgM, and IgG at 7 months (130).
Fetal risks
Chickenpox infection is not associated with an increased risk of first- or second-trimester miscarriage. Fetal varicella syndrome is characterized by segmental skin loss, scarring, limb deformities, microcephaly, intellectual disability, hypotonia, bladder and/or bowel sphinteric dysfunction, cataracts, and chorioretinitis, and the risk of its occurrence is about 1% if maternal infection occurred before 28 weeks. Fetal varicella syndrome is due to the reactivation of VZV in utero. Since transplacental transfer of maternal antibodies is limited before 28 weeks' gestation, maternal immunity does not usually protect fetuses less than 28 weeks' gestation (130).
Perinatal chickenpox
Maternal chickenpox infection near the time of delivery or in the immediate postpartum period results in early neonatal chickenpox because of insufficient production and transfer of protective antibodies to the infant. Approximately 50% of infants delivered within 1-4 weeks of maternal infection are infected even in the presence of high antibody titres suggesting that in the short term, these antibodies may be less protective. Severe neonatal chickenpox is likely if delivery occurred within seven days of the onset of maternal rash. VZIG should be administered at birth in this situation and also if maternal chickenpox occurred within 2 days of delivery (130). The infant should be monitored for signs of infection for 14-16 days and treated with IV aciclovir if neonatal chickenpox occurred. Consideration should be given if possible to delaying the delivery for 5- 7 days after the onset of maternal illness to allow transfer of maternal antibodies. If a neonate of a non-immune mother comes into contact with chickenpox, VZIG should be administered (130).
Hepatitis B
The hepatitis B virus (HBV) is a partially double-stranded DNA hepatotropic virus. It is estimated that 240 million people worldwide are chronically infected with hepatitis B (131).
Epidemiology
Hepatitis B is a potentially life-threatening liver infection and more than 686,000 people die every year from complications of hepatitis B infection, including cirrhosis and liver cancer (132). The virus is transmitted through contact with infected blood or other body fluids including sexual transmission. Hepatitis B is an important occupational hazard for health workers. In highly endemic areas, hepatitis B is most commonly spread from mother to child at birth (perinatal transmission) or through horizontal transmission (exposure to infected blood), especially from an infected child to an uninfected child during the first 5 years of life.
Clinical diagnosis
The HBV can survive outside the body for at least 7 days. The virus remains infectious during this time if it enters the body of a susceptible individual. The incubation period is approximately 75 days but can vary from 30 to 180 days. The virus may be detected within 30-60 days of infection and may persist and develop into chronic hepatitis B.
Hepatitis B viral infection has a wide sp ectrum of clinical manifestations ranging from acute hepatitis, through asymptomatic carriage, to liver cirrhosis and hepatocellular carcinoma. While most affected individuals are asymptomatic during the acute infection, some experience acute illness manifesting as fatigue, nausea, vomiting, jaundice, and abdominal pain, which may persist for several weeks. A small subset of patients with acute hepatitis may develop acute liver failure, which can be fatal. The likelihood of chronic infection is inversely related to the age of acquisition of the virus. The majority of infected adults recover and develop long-lasting immunity, defined as loss of hepatitis B surface antigen (HBsAg) and development of antibodies against the surface antigen (anti-HBsAb). In contrast, vertical transmission at birth or infection in early childhood carries a high risk of chronic liver infection, which may progress to liver cirrhosis or hepatocellular carcinoma. Children less than 6 years of age who become infected with the HBV are the most likely to develop chronic infection. The diagnosis of the infection is based on the clinical picture and serological detection of:
• HBsAg—current infection
• HB e antigen (HBeAg)—active viral replication
• anti-HBsAb (antibodies)—indicating immunity either from infection or vaccination.
Treatment
There is no specific treatment for acute hepatitis B. Therefore, care is aimed at maintaining comfort and adequate nutritional balance, including replacement of fluids lost from vomiting and diarrhoea. Chronic hepatitis B infection with high viral load can be treated with antiviral agents such lamivudine. It is now well established that HBV infection and its complications can be prevented by active and passive vaccination. A vaccine against hepatitis B has been available since 1982. The vaccine is 95% effective in preventing infection and the development of chronic disease and liver cancer (131). All pregnant women should be screened for HBV at booking. High- risk women (commercial sex workers and IV drug abusers) should be counselled and vaccinated before pregnancy. Acute HBV infection in pregnancy is per se not associated with an increase in maternal morbidity or mortality and does not increase the risk of fetal congenital abnormalities. An increased risk of preterm labour has been reported. The risk of perinatal transmission is high especially in the third trimester or postpartum period.
The risk of perinatal infection in chronic carriers depends on maternal HBeAg status. Without immunoprophylaxis and depending on maternal viral load, up to 90% of infants born to HBeAg-positive mothers acquire the infection compared to approximately 10% of babies born to HBeAg-negative mothers (133). If chronic HBV infection is diagnosed in pregnancy, complete serological work-up including liver ultrasound, liver function tests, viral load estimation, and if indicated serum levels of alpha-fetoprotein should be determined to assess liver damage. Hepatologists should be involved in the care of the pregnant woman to determine the need for and type of antiviral therapy required during or after delivery. The risk of fetal hepatitis B infection through amniocentesis is low; however, if amniocentesis is required, insertion of the needle through the placenta should be avoided. During labour, invasive procedures such as fetal blood sampling, fetal scalp electrode, or instrumental delivery should be avoided. Neonatal infection may be fatal or result in chronic carrier status with significant lifelong risks of cirrhosis and liver cancer. Babies whose mothers have acute or chronic HBV should receive HBV IgG (immunoglobulins) and vaccination within 24 hours of delivery with the aim of completing the schedule. This is thought to be up to 95% effective at preventing neonatal HBV infection (131).
Hepatitis C
Hepatitis C virus (HCV) infection is a major global health problem. The infection is caused by a single-stranded virus, which is transmitted through infected blood and sexual (rare) route.
Epidemiology
The average time from exposure to the HCV to seroconversion is about 8-9 weeks. Women with risk factors for HCV such as IV drug abusers and HIV-positive women should be counselled and offered screening.
Clinical diagnosis
Acute infection may present with loss of appetite, nausea, vomiting, abdominal pain, and jaundice. However, up to two-thirds of infections are asymptomatic.
The diagnosis is confirmed by detecting anti-HCV antibodies or HCV RNA in blood. HCV may remain quiescent for many years before progression to chronic infection (85%), cirrhosis (20%), or hepatocellular carcinoma (134, 135) (intrapartum invasive procedures such as fetal scalp electrode or fetal blood sampling should be avoided in women with undetectable viral load. Membranes should be kept intact for as long as possible during labour. To prevent chorioamnionitis and perinatal transmission, labour should be expedited for all women with rupture of membranes at term.
If a woman presents in labour and is not on treatment, she should be given a stat dose of nevirapine as this rapidly crosses the placenta. While the obstetric management continues, if time permits prior to caesarean section, more potent ART, which crosses the placenta and results in rapid reduction of the viral load should be administered (136). If delivery is indicated before 34 weeks, the risk of prematurity-related complications, availability of neonatal facilities, and the risk of perinatal HIV transmission should be considered in timing of the delivery.
ART to the newborn is an example of pre-exposure prophylaxis and should be decided before the delivery. The main antiretroviral therapies licensed for neonates are oral preparations and therefore it is necessary to treat the mother in order to optimize the prognosis for the preterm neonate. ART should be commenced in the neonate as soon after birth as possible. Infants born to HIV-positive mothers should have an HIV test on day 1, at 6 weeks, and at 12 weeks of age. If breastfeeding has not occurred and all these tests are negative, the infant is classified as HIV negative and a confirmatory blood test should only be offered at 18 months of age. In the postpartum period, women should be advised not to breastfeed, although in resource-poor settings breastfeeding may need to continue in the absence of valid alternatives. HIV-p ositive mothers should be offered appropriate vaccines and given advice regarding contraception and regular cervical screening (140). A multidisciplinary care plan should be put in place during and after pregnancy for women with HIV as many of them may suffer from consequences of chronic HIV infection, opportunistic infections, stigma, poverty, homelessness, domestic violence, drug abuse, and mental illness.