Introduction
While it is widely agreed that one of the major achievements in women's health in the last millennium has been the availability of safe and effective contraception, there are some 225 million women worldwide with unmet contraceptive needs and this results in about 80 million unintended pregnancies per annum of which about 50% are terminated, often by unsafe abortion.
This unmet need is highest among the most vulnerable in society including adolescents, people living with HIV, the poor, and other marginalized groups.The Millennium Development Goals (MDGs) were formulated following the Millennium Summit in 2000 and MDG 5 aimed at ‘Improving maternal health'. This goal specifically dealt with reducing maternal mortality and morbidity by 2015. It was after considerable lobbying by interested parties that in 2007 MDG 5b was included which explicitly presented targets for reproductive health including the contraceptive prevalence rate (1). The MDGs have now been superseded by the 17 Sustainable Development Goals (SDGs) which present the 2030 agenda for a plan of action for ‘people, planet and prosperity'. SDG 3 aims to ‘ensure healthy lives and promote wellbeing for all at all ages' and it is within this SDG that contraceptive access is mentioned and promoted. Given that effective contraception will prevent unintended pregnancies and significantly impact maternal mortality and morbidity it is concerning that it does not achieve a higher profile (2).
In the Western World, most of the original contraceptive services were male orientated and utilized condoms or coitus interruptus. As new and safe methods for female contraception have become available, these services and technologies have expanded both in industrialized and developing countries. Access to fertility regulation is varied around the world with some notable successes and some unfortunate failures.
The commitment of governments in developing countries to fund women's health initiatives is often limited by resources. Darroch and Singh reviewed the trends in contraceptive need and use in developing countries and noted that women who wish to avoid unintended pregnancies and need effective contraception often do not have their requirements adequately addressed within the services available to them (3). There is a considerable literature about the impact of early motherhood on women and their children and it is evident that this puts young women at risk for educational underachievement and prejudices their economic situation (4). This obviously impacts their children and may exacerbate the cycle of deprivation and need. It is therefore essential that good contraceptive services and appropriate counselling are provided to women in all situations. The impact of unintended pregnancy is considerable and affects the lives of both the mother and her children (5, 6).According to the WHO guideline ‘Ensuring human rights in the provision of contraceptive information and services', nine key health and human rights standards should be considered (7). These are outlined in Box 53.1. The application of human rights principles to contraceptive service provision is of critical importance and can also be used to identify, reduce, and eliminate barriers to accessing contraception (8).
Contraceptive effectiveness is determined by efficacy (theoretical ability to prevent pregnancy), compliance, continuation, fecundity (ability to conceive), and the timing of coitus. All methods which are offered need to be accessed utilizing these parameters (9) (Table 53.1). There is currently a move to classify methods in terms of their duration of effectiveness but this is not yet in place.
The Medical Eligibility Criteria (MEC) for contraceptive use is part of the WHO process for improving the quality of care in contraceptive provision. The fifth edition was published in 2015 and presents current WHO guidance on the safety of various contraceptive methods for use in the context of specific health conditions and characteristics (10).
In these guidelines, the safety of each contraceptive method is outlined and several considerations are utilized in the context of both the medical condition and medically relevant characteristics. This very valuable document takes into account whether the contraceptive method worsens the medical condition or creates additional health risks and secondarily whether the medical condition has an effect on the effectiveness of the contraceptive method. The safety of the method should always be weighed against the benefit of preventing unintended pregnancy. The recommendations cover many contraceptive methods and for each condition or characteristic the methods are characterized in one of four numbered categories (11) (Table 53.2). Every client should be assessed individually as more than one condition may need to be considered to determine contraceptive eligibility. This document provides valuable information to both clinicians and policymakers and should be regularly accessed.Box 53.1 Human rights in the provision of contraceptive information and services
1 Non-discrimination
2 Availability
3 Accessibility
4 Acceptability
5 Quality of care
6 Participation
7 Informed decision-making and choice
8 Privacy/confidentiality
9 Accountability
Source data from World Health Organization. Ensuring Human Rights in the Provision of Contraceptive Information and Services: Guidance and Recommendations. Geneva: World Health Organization; 2014. http://apps.who.int/iris/bitstream/10665/ 102539/1/9789241506748_eng.pdf (accessed 10 September 2015).
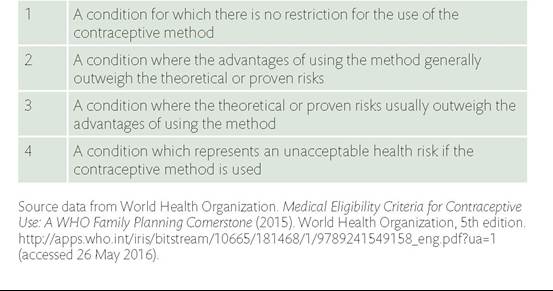
Table 53.1 Percentage of women experiencing an unintended pregnancy during the first year of typical use and the first year of perfect use of contraception and the percentage continuing use at the end of the first year
| Method | Women experiencing an unintended pregnancy within the first year of use | Women continuing use at 1 year (%) | |
| Typical use (%) | Perfect use (%) | ||
| No method | 85 | 85 | |
| Spermicides | 28 | 18 | 42 |
| Withdrawal | 22 | 4 | 46 |
| Fertility awareness methods a. Standard days methodab. 2-day methodb c. Ovulation methodb d. Symptothermal methodb | 24 | 5 4 3 0.4 | 47 |
| Condom (male) | 18 | 2 | 43 |
| Combined pill and progestogen- only pill | 9 | 0.3 | 67 |
| Combined hormonal patch (Evra) | 9 | 0.3 | 67 |
| Combined hormonal ring (Nuvaring) | 9 | 0.3 | 67 |
| Depo medroxyprogesterone acetate, DMPA (Depo-Provera) | 6 | 0.2 | 56 |
| Cu-IUCD (Copper T) | 0.8 | 0.6 | 78 |
| LNG-IUS(Mirena) | 0.2 | 0.2 | 80 |
| Subdermal implant (Implanon) | 0.05 | 0.05 | 84 |
| Female sterilization | 0.5 | 0.5 | 100 |
| Male sterilization | 0.15 | 0.1 | 100 |
a Method involves avoiding intercourse on cycle days 8-19.
b The ovulation and 2-day methods are based on evaluation of cervical mucus. The standard days method avoids intercourse on cycle days 8 through 19. The symptothermal method is a double-check method based on evaluation of cervical mucus to determine the first fertile day and evaluation of cervical mucus and temperature to determine the last fertile day.
Source data from Trussell J. Contraceptive efficacy In: Hatcher RA, Trussell J, Nelson AL, Cates W, Kowal D, Policar M, eds. Contraceptive Technology, 20th revised edn, pp. 779844. New York: Ardent Media; 2011.
There are numerous challenges in providing accessible and appropriate fertility regulation to women around the world. While it has been stated that a women ‘cannot die from a pregnancy she does not have, the prevention of unintended pregnancies also impacts perinatal and child mortality. Contraception is central to maternal health and we recognize the needs of developing countries in accessing advances in reproductive health. Health budgets are limited and the newer technologies such as the levonorgestrel-r eleasing intrauterine system (LNG-IUS) are often unaffordable. The HIV pandemic which has particularly affected Africa has impacted every aspect of healthcare. In providing good contraceptive advice worldwide it must be recognized what the challenges are, what the limitations of provision are due to budgetary constraints, and what is acceptable in different countries and cultures.