Liver disease
Liver diseases of pregnancy can be divided into disorders specific to pregnancy or diseases incidental to pregnancy. Pregnancy-specific disorders include hyperemesis gravidarum, intrahepatic cholestasis of pregnancy (ICP), acute fatty liver, and pre-eclampsia with hepatic involvement.
Many hepatic diseases affect women of reproductive age. Viral hepatitis is very common worldwide. Some non- infectious disorders present in women of reproductive age (e.g. autoimmune hepatitis). While these commonly will have been diagnosed prior to a woman becoming pregnant, some may present de novo in pregnancy. It is therefore important to take a thorough history and perform a clinical examination to establish the underlying diagnosis in pregnant women with new symptoms or signs consistent with liver disease. The typical symptoms associated with specific liver disorders are summarized in Table 23.1. Not all symptoms are specific to a specific disorder, for example, although pruritus is associated with cholestasis, it may also occur in pregnant women who do not have liver disease. It is also important to know which clinical features are not of concern in pregnancy, and of note, palmar erythema and spider naevi occur in a large number of pregnant women without associated liver disease.To manage women with gestational liver disease effectively, clinicians should know the normal ranges for liver function tests (LFTs) in pregnancy (Table 23.2) (1). The upper end of the normal range for liver transaminases is reduced by approximately 20%, likely secondary to the increase in circulating volume in the second half of pregnancy. There is a similar reduction in the normal range for bilirubin and gamma-glutamyltranspeptidase, but this is not seen for alkaline phosphatase because there is secretion of a placenta-specific isoform in the third trimester.
Disorders specific to pregnancy
Hyperemesis gravidarum
While nausea and vomiting are relatively common in the first trimester, affecting almost 50% of pregnant women, it is much less common to have severe and protracted vomiting (approximately 1%).
If women cannot maintain normal fluid and food intake or weight, they should be assessed for dehydration and for coexisting pathology (Table 23.3). Blood tests should be taken to ensure they do not have electrolyte disturbance, abnormal LFTs, or biochemical abnormalities of thyroid function tests. Many women with protracted vomiting have hyponatraemia, and this should be corrected slowly with normal saline. It is important to also monitor serum potassium concentrations and to correct hypokalaemia. Abnormal LFTs usually indicate starvation, and they typically return to normal once a woman recommences oral intake. Women with severe hyperemesis gravidarum can have biochemical thyrotoxicosis. This is very rarely seen in conjunction with clinical features of hyperthyroidism, and is usually a marker of severe disease that resolves when the underlying hyperemesis has been successfully treated.Women with hyperemesis gravidarum can be treated with hydration and antiemetics. There are good safety data for most commonly used antiemetic drugs such as doxylamine with pyridoxine, cyclizine, metoclopramide, promethazine, and prochlorperazine. Women should be reassured that use of these drugs is not associated with an increased risk of congenital malformation. The majority of women respond to a combination of these drugs, ideally with doses spaced throughout the day. If women do not respond to these drugs, either ondansetron or glucocorticoids may be used as second-line treatment. Thromboprophylaxis should be given to women who are admitted to hospital or to those that have risk factors for thrombosis, and thiamine replacement is recommended due to the increased risk of deficiency with acute vomiting. This is important as thiamine deficiency is associated with Wernicke’s encephalopathy.
Some investigators have reported increased rates of small-for- gestational age babies and preterm birth in women with hyperemesis gravidarum with low weight gain throughout pregnancy, although this was not seen in all studies.
However, it is important to ensure adequate food and fluid intake in pregnancy and antiemetic drugs with good safety data to support their use should not be withheld. This is of particular importance given that women with hyperemesis gravidarum are reported as dying in pregnancy approximately once every 1-3 years in the United Kingdom in the Confidential Enquiries into Maternal Deaths.Table 23.1 Typical symptoms associated with abnormal liver function tests in pregnancy and likely associated diagnosis
| Symptom | I Likely diagnosis | I Other possible diagnoses |
| ICP | Pre-eclampsia, AFLP biliary obstruction, pre-existing hepatobiliary disease (PBC, PSC), DILI | |
| Epigastric pain Nausea and vomiting—second and third trimester Headache Visual disturbance | Pre-eclampsia, HELLP syndrome, AFLP | Gallbladder disease, cholangitis, viral hepatitis |
| Nausea and vomiting—first trimester | Hyperemesis gravidarum | Viral hepatitis |
| Jaundice | Viral hepatitis | HELLP syndrome, gallbladder disease, cholangitis, DILI, rarely ICP or pre-eclampsia |
| Pale stools and dark urine | Biliary obstruction secondary to gallstone disease | ICP cholangitis, viral hepatitis, other rare causes of biliary obstruction |
AFLP1 acute fatty liver of pregnancy; DILI, drug-induced liver injury; HELLP1 haemolysis, elevated liver enzymes, and low platelets; ICP, Intrahepatic cholestasis of pregnancy; PBC, primary biliary cholangitis; PSC, primary sclerosing cholangitis.
Source data from Walker I, Chappell LC, Williamson C.
Abnormal liver function tests in pregnancy, BMJ 2013;347:f6055,Table 23.2 Typical reference ranges for liver enzymes, by trimester
| Liver enzyme | I Non-pregnant | I Pregnant | I First trimester | Second trimester | I Third trimester |
| Alanine transaminase (ALT) (IU/L) | 0-40 | - | 6-32 | 6-32 | 6-32 |
| Aspartate transaminase (AST) (IU/L) | 7-40 | - | 10-28 | 11-29 | 11-30 |
| Bilirubin (μmol∕L) | 0-17 | - | 4-16 | 3-13 | 3-14 |
| Gamma-glutamyltranspeptidase (γGT) (IU/L) | 11-50 | - | 5-37 | 5-43 | 3-41 |
| Alkaline phosphatase (ALP) (IU/L) | 30-130 | - | 32-100 | 43-135 | 133-418 |
| Albumin (g/L) | 35-46 | 28-37 | - | - | - |
| Bile acids (μmoRL) | 0-14 | 0-14 | - | - | - |
Source data from Walker I, Chappell LC, Williamson C. Abnormal liver function tests in pregnancy. BMJ 2013;347:f6055.
Table 23.3 Coexisting pathology that should be considered in a woman with hyperemesis gravidarum
| System | Diagnosis | I Investigation/initial assessment | I Frequency |
| Obstetric | Molar pregnancy | Ultrasound scan of the uterus | + |
| Gastrointestinal | Gastritis/peptic ulceration | Helicobacter pylori antibodies | + |
| Gastroesophageal reflux and ulcerative esophagitis | Endoscopy or empirical proton pump inhibitor therapy | ++ | |
| Pancreatitis | Amylase, blood glucose, calcium | + | |
| Bowel obstruction | Plain supine abdominal X-ray | + | |
| Endocrine | Addison's disease | U&E, early morning cortisol, short Synacthen test with ACTH | + |
| Hyperthyroidism | Surveillance for symptoms and signs of hyperthyroidism, TFTs, thyroid autoantibodies | ++ | |
| Diabetic ketoacidosis | Blood glucose, urinary dipstick for ketones, glucose tolerance test | ++ | |
| CNS | Intracranial tumour | CNS examination, brain imaging | + |
| Vestibular disease | CNS examination | + | |
| Respiratory | Asthma | Chest examination, peak expiratory flow rate, | ++ |
| Other | Urinary tract infection | Mid-stream urine specimen | +++ |
| Uraemia | U&E | + |
ACTH, adrenocorticotropic hormone; CNS, central nervous system; TFTs, thyroid function tests; U&E, urea and electrolytes,
Pre-eclampsia (including HELLP syndrome)
In a study of the underlying diagnosis in women presenting with abnormal LFTs in pregnancy in Wales (2), 71% of the women studied had pre-eclampsia.
While HELLP (haemolysis, elevated liver enzymes, and low platelets) syndrome affected one-third of cases, it was much commoner for women to present with pre-eclampsia and isolated abnormal LFTs, in the absence of low platelets or haemolysis. Thie presentation and management of pre-eclampsia and HELLP syndrome are discussed elsewhere (see Chapter 21). However, it is important to note that some other disorders are more commonly complicated by preeclampsia. These include pre-existing hypertension, raised maternal body mass index, diabetes mellitus, renal disease, and a number of other vascular, endocrine, and metabolic disorders.Intrahepatic cholestasis of pregnancy
ICP, also called obstetric cholestasis, is the commonest liver-specific disorder of pregnancy. ICP affects 1 in 140 pregnant women in the United Kingdom, but there is considerable geographic variation in the prevalence of the condition with higher rates in South America, particularly Chile, and in women of South Asian and Hispanic origin. Most women with ICP are well when they are not pregnant, and present in pregnancy with generalized pruritus, raised serum bile acid concentrations, and the majority also have abnormal LFTs. The serum bile acid level is the most important biochemical abnormality for diagnosis of ICP because high concentrations in the mother’s blood are associated with increased rates of adverse pregnancy outcome (3, 4). The first large, national study that demonstrated an association between serum bile acid concentrations and outcomes in ICP reported no increase in adverse outcomes (spontaneous preterm labour, fetal asphyxia events, and meconium-stained amniotic fluid) when the maternal bile acid concentration was less than 40 μmol∕L, but these complications were increased with higher concentrations (3). A UK cohort study and subsequent large individual patient data meta-analysis confirmed these results and also demonstrated a significant increase in stillbirth which increased further as the maternal bile acid concentration increased to above 100 μmol∕L confirmed these results and also demonstrated a significant increase in stillbirth which increased further as the maternal bile acid concentration became higher (4).
The association between maternal alanine aminotransferase (ALT) concentrations and adverse pregnancy outcome is not as clear cut, and hence it is advisable to monitor maternal serum bile acid concentrations regularly after a diagnosis of ICP has been made, as they typically continue to rise with advancing gestation. Although pruritus in ICP is not preceded by a rash, some women develop skin lesions secondary to scratching (Figure 23.1).If a woman presents with ICP, it is important to perform blood tests to evaluate the severity of the elevation in bile acids to consider the risk of adverse pregnancy outcome, and to measure LFTs to evaluate the extent of maternal hepatic damage. While most women have transient cholestasis that resolves after delivery, a small proportion of women with ICP have another underlying disorder (Table 23.4) and it is important to monitor the liver function to ensure they do not deteriorate. The pattern of LFTs is typically characterized by raised liver transaminases (e.g. ALT) in addition to elevated serum bile acids, and both usually continue to rise with advancing gestation. The gamma-glutamyltranspeptidase concentration is raised in approximately one-third of women, and bilirubin is rarely elevated

Figure 23.1 Dermatological lesions on the back of a woman with ICP. Excoriations and scarring are secondary to scratching. Figure reproduced with permission of ICP Support.
in ICP. Occasionally, women with ICP have abnormal coagulation tests. This is likely to be secondary to ICP-associated steatorrhoea and vitamin K malabsorption, and treatment with vitamin K should improve this. Tests should be requested to exclude hepatitis C, autoimmune hepatitis, and an abdominal ultrasound scan performed to ensure there is no extrahepatic cause of biliary obstruction. This will demonstrate gallstones in a sizeable proportion of cases because the underlying genetic susceptibility to ICP is caused by some genes that are also associated with an increased risk of gallstones. However, gallstones are very rarely the cause of the cholestasis.
The most commonly used treatment for ICP is ursodeoxycholic acid (UDCA). Several studies have reported improved maternal symptoms and biochemistry with UDCA treatment (5-8). At present it is not established whether UDCA treatment improves adverse pregnancy outcome, although a meta-analysis that considered
Table 23.4 Coexisting pathology that should be considered in a woman with intrahepatic cholestasis of pregnancy
| System | Diagnosis |
| Gestational diseases | Acute fatty liver of pregnancy Pre-eclampsia with abnormal liver function |
| Disorders not related to pregnancy | Hepatitis C Autoimmune hepatitis Primary biliary cholangitisa Primary sclerosing cholangitis Drug-induced liver injury Gallstones ± cholangitis |
a Also called primary biliary cirrhosis.
all trials of UDCA compared to another drug or placebo reported improved rates of preterm labour, fetal distress, respiratory distress, and prolonged neonatal unit admission in pregnancies treated with UDCA (7). A trial that compared UDCA to placebo treatment in 605 women with ICP, diagnosed in women with serum bile acids of 10 μmol∕L or more, in the United Kingdom showed some reduction in pruritus, but no improvement in a composite outcome of all preterm birth, stillbirth or admission to the neonatal unit (8). For women with severe pruritus, aqueous cream with 1-2% menthol may provide symptomatic relief and vitamin K treatment is recommended for women with steatorrhoea.
There is no established form of monitoring that can predict which ICP pregnancies are likely to be complicated by spontaneous preterm labour, fetal distress, or stillbirth. Many hospitals offer regular review in the antenatal day unit, with cardiotocograph checks. While this is reassuring at the time it is performed, it will not give information about the risk of stillbirth after the monitor has been removed. The recent individual patient data meta-analysis (8) showed that the significant increase in stillbirth that occurred in pregnancies where maternal serum bile acids were greater than 100 μmol∕L, showed a marked increase in risk between 35-36 weeks' gestation. Therefore early delivery should be considered in this subgroup of women with ICP. It is advisable to check serum bile acids at least weekly from 35 weeks in severe cases as they may rise considerably with advancing gestation. While the increased risk of prolonged admission to the neonatal special care unit has been shown to be associated with higher maternal bile acid concentrations, and there is evidence that bile acid inhibit phospholipase A2, and are likely to cause abnormalities in surfactant (9, 10), it is likely that preterm delivery also contributes to this risk.
For most women, the pruritus and abnormal biochemistry resolve after delivery. It is important to check the serum bile acid concentrations and LFTs to ensure they are returning to normal after delivery. For some women it takes up to 3 months for the tests to return to normal. It is advisable to refer those with ongoing abnormalities to a hepatologist for assessment. Women should be advised that they have a high risk of ICP in subsequent pregnancies, particularly if they have a multiple pregnancy. They should also avoid the combined oral contraceptive pill, although progesterone-only contraception does not cause problems for the majority. They are at increased risk of biliary disease in later life (11).
Acute fatty liver of pregnancy
Acute fatty liver of pregnancy (AFLP) affects 1 in 20,000 pregnancies in the United Kingdom (12). It presents in the third trimester with non-specific symptoms, including nausea, vomiting, polyuria, polydipsia, and feeling generally unwell. Affected women have abnormal LFTs, often with markedly raised liver transaminases, bilirubin, and coexisting elevation of creatinine, leucocytes, abnormal coagulation, and metabolic acidosis. However, the extent of the biochemical abnormalities may vary. It is often useful to consider the ‘Swansea criteria' for diagnosis of AFLP (Table 23.5). At least six of these clinical features are present in the majority ofwomen with AFLP (12, 13). The condition can deteriorate rapidly, and can result in fulminant hepatic failure. Approximately one woman in the United Kingdom dies from AFLP each year. Most affected women should be cared for in a high dependency or intensive care setting. It is advisable to involve a specialist liver unit early and the input of a multidisciplinary team will be needed, including specialist physicians, obstetricians, midwives,
Table 23.5 Diagnostic criteria for acute fatty liver of pregnancy (AFLP; Swansea criteria); AFLP is the likely diagnosis if six or more features are present
| Clinical features | Vomiting Abdominal pain PolydipsiaZpolyunia Encephalopathy |
| Blood test abnormalities | Elevated bilirubin Hypoglycaemia Elevated urate Leucocytosis Elevated transaminases Elevated ammonia Renal impairment Coagulopathy |
| Imaging | Ascites or bright liver on ultrasound |
| Invasive testing | Microvesicular steatosis on liver biopsy |
Source data from Ch'ng CL, Morgan M, Hainsworth I, Kingham JG. Prospective study of liver dysfunction in pregnancy in Southwest Wales. Gut 2002;51:876-80.
obstetric anaesthetists, and intensive care specialists. Women with AFLP should be delivered as soon as they have been stabilized as once the placenta has been delivered, the metabolites that cause maternal hepatic impairment will cease to be transported to the mother. Prior to delivery it is important to ensure that coagulopathy and hypoglycaemia have been treated, in addition to correcting any other life-threatening biochemical derangements. AFLP resolves after delivery, although women can deteriorate for a small number of days before they start to improve. Approximately 20% of cases present in the immediate postpartum period, likely related to enhanced release of placental or fetal metabolites that cause hepatic damage at the time of delivery. Providing they do not develop fulminant hepatic failure requiring transplant, most women make a full recovery within a small number of weeks following delivery. A small proportion of cases have children with disorders of beta-fatty acid oxidation (14, 15) and it is therefore advisable to ensure the children of women with AFLP are screened, as they are likely to remain healthy if fed a high-carbohydrate diet. In the United Kingdom, these disorders are detected by neonatal Guthrie spot screening. It is important to ensure that liver function returns fully to normal after pregnancy. The risk of recurrence of AFLP has not been accurately established, with the exception of women who are obligate heterozygotes for fatty acid oxidation disorders, but it is likely to be 10-20%.
Disorders incidental to pregnancy
Women of reproductive age can have a variety of hepatic disorders, and the commoner ones will be discussed in the following sections. The most important issues for the majority of women with preexisting disease are to ensure they have prepregnancy counselling from a doctor with experience and knowledge of liver disease in pregnancy. This will enable them to embark on pregnancy cognisant of the risks associated with their disease and the drugs used to treat it. Decisions can also be made about where a woman should be managed, whether this should be as part of a multidisciplinary team, at a tertiary referral centre or if she should have shared care.
Viral hepatitis
Hepatitis B infection is the commonest cause of jaundice in pregnancy worldwide. However, acute and chronic maternal disease is
managed the same way in pregnancy as in non-pregnant individuals. It is important to give the neonates of affected women immunoglobulin and the hepatitis B vaccine to prevent mother-t o-child transmission. Mode of delivery does not influence the rate of vertical transmission. However, this may be increased in women with a high viral load in pregnancy, and in these cases it is advisable to treat with nucleoside analogues (16).
The clinical presentation and treatment of most other forms of viral hepatitis are not affected by pregnancy. An exception is hepatitis E, a virus transmitted by the faecal- oral route, that normally has a mild course in non-pregnant individuals, but can commonly cause fulminant hepatic failure in pregnant women (17, 18). Hepatitis C infection is a blood-borne infection that may present for the first time in pregnancy, typically with symptoms of cholestasis. There is no specific treatment for the infection in pregnancy, but affected women should be referred for treatment postnatally. There is relatively low vertical transmission in the absence of coexisting HIV infection and mode of delivery does not influence this. Breastfeeding should be encouraged as this does not increase the rate of neonatal infection.
Autoimmune hepatitis
Autoimmune hepatitis occurs in women of reproductive age. They have a 25% chance of flare, particularly in the postpartum period, and this is reduced in those that continue immunosuppressive treatment. It is therefore important for hepatologists caring for these women to ensure that they are given appropriate prepregnancy counselling. They should be informed that azathioprine has good safety data to support its use in pregnancy and lactation, and that prednisolone treatment can be used if required (19). Mycophenolate mofetil should not be used in pregnant women as it is associated with high rates of congenital malformations, and if a woman using this drug intends to conceive, her medication should be changed to another drug (e.g. azathioprine, ciclosporin, or tacrolimus). Some women with autoimmune hepatitis have cirrhosis (see later).
Budd-Chiari syndrome
Pregnancy is a prothrombotic state, and a number of new cases of Budd-Chiari syndrome have been diagnosed in pregnancy. However, this is a relatively rare disorder and the majority of cases will have presented before pregnancy. In the rare circumstance when a woman presents de novo in pregnancy, the typical symptoms are ascites, jaundice, and right upper quadrant pain. In women with a pre-existing diagnosis of Budd-Chiari syndrome, many have an underlying thrombophilia and it will be important to ensure adequate anticoagulation, usually with low-molecular-weight heparin. A series of 24 pregnancies in 16 patients treated for Budd-Chiari syndrome reported good maternal outcomes but a preterm birth rate exceeding 50% (20).
Primary biliary cholangitis and primary sclerosing cholangitis
Primary biliary cholangitis (PBC), also called primary biliary cirrhosis, is a chronic autoimmune cholestatic disorder that typically affects postmenopausal women. Common symptoms are pruritus and fatigue in conjunction with hepatic impairment, and it may coexist with other autoimmune disorders. Some cases occur at younger ages and the condition can occur in pregnant women. The prognosis of PBC in pregnancy has improved in more recent studies in which women are treated with UDCA (21). However, despite improved maternal and fetal outcomes most women have a deterioration in liver function postpartum, although this usually resolves after 12 months.
Primary sclerosing cholangitis (PSC) is a chronic inflammatory disorder characterized by fibrosis and stricturing of the intrahepatic and extrahepatic bile ducts, resulting in cholestasis and hepatic damage. Up to 90% of patients have coexisting ulcerative colitis. PSC more commonly affects men, but women are also affected and it usually presents before the age of 40, so it may occur in pregnancy. The most common maternal symptoms are pruritus and abdominal pain (22). UDCA is used less frequently to treat PSC than PBC, and there is no evidence that it improves maternal prognosis during pregnancy. However, given the accumulating data that maternal serum bile acid concentrations of at least 40 μmol∕L increase the risk of spontaneous preterm labour, prolonged admission to the neonatal unit, and stillbirth in pregnancies complicated by cholestasis in the absence of PBC or PSC (4), it seems sensible to consider UDCA treatment during pregnancy for women with raised serum bile acids. However, it should be noted that high-dose UDCA treatment is associated with poorer outcomes in PSC outside pregnancy.
Cirrhosis
Many women with chronic cirrhosis have impaired fertility, but some women with treated autoimmune hepatitis, PBC, PSC or long-standing viral hepatitis can become pregnant with cirrhosis. Women with established cirrhosis should be screened for oesophageal varices in the second trimester, and if necessary treatment can be performed with banding or sclerotherapy. Decisions about mode of delivery should be made on a case-by-case basis. The presence of portal hypertension with treated (or minor) varices is not a reason to avoid vaginal delivery.
Bleeding from oesophageal varices
Women with portal hypertension (with or without cirrhosis) are at risk of gastrointestinal haemorrhage. Oesophageal varices may develop in pregnancy in women without liver disease, and in those with portal hypertension this may result in a considerable risk of gastrointestinal bleeding. For women with non-cirrhotic portal hypertension, the risk of bleeding is 10-15%. For those with cirrhosis and untreated oesophageal varices, the risk is very high (70-90%) and is considerably reduced if the varices are treated with banding or sclerotherapy (approximately 10%). In women with life-threatening haemorrhage, vasoconstrictors such as terlipressin can be used, although there are limited safety data for these drugs.
Gallstones
Pregnancy is associated with a tendency to develop cholesterol gallstones. In the majority of women they will be asymptomatic and they may resolve postpartum. Asymptomatic gallstones should not be treated in pregnancy. A small proportion of women may develop acute cholecystitis, and this group should be treated in the same way as they would be managed outside pregnancy with cessation of oral intake, intravenous fluids, antibiotics, and assessment for suitability for surgery. A study that compared outcomes of women with acute cholecystitis treated medically or surgically demonstrated good outcomes for all women treated with surgery, while there was a 38% relapse rate in those that received medical management (23).
Pregnancy following liver transplantation
Fertility typically returns within 6 months of a liver transplant. It is advised to delay conception until 12 months after transplantation as this reduces the risk of transplant rejection. Good outcomes are reported for the majority of women, although there is an increased risk of pregnancy-induced hypertension, pre-eclampsia, and preterm delivery (24). Most immunosuppressive drugs can be used in pregnancy, and there are good safety data for azathioprine, ciclosporin, and tacrolimus. Women treated with mycophenolate should be given prepregnancy advice about the high congenital malformation rate associated with this drug, and their treatment regimen should be changed to include alternative immunosuppressive drugs prior to conception.
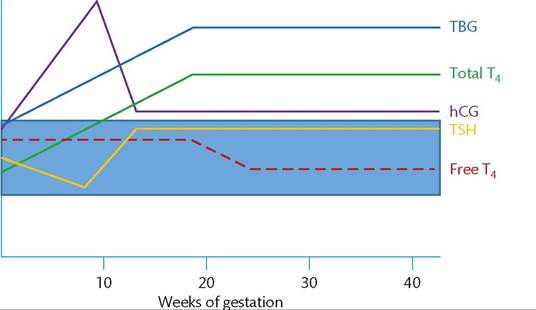
Figure 23.2 Normal ranges for thyroid function tests in pregnancy. hCG, human chorionic gonadotropin; T4, tetraiodothyronine (thyroxine); TBG, thyroid-binding globulin; TSH, thyroid-stimulating hormone.
Endocrine disease
Endocrine disorders affect many glands and are commonly seen in pregnant women. Most women with endocrine disorders in pregnancy have a condition that is not specific to pregnancy. However, there are a small number of women who develop gestational hyperthyroidism, and hyperemesis has an endocrine component as women with severe disease can develop biochemical thyrotoxicosis (see ‘Hyperemesis gravidarum'). Autoimmune endocrine disorders can improve during pregnancy, but typically worsen in the postpartum period. Also, some endocrine tumours can worsen during pregnancy, for example, prolactinomas commonly enlarge and in a subgroup of women with large tumours this can cause visual impairment. Clinicians managing pregnant women with endocrine disease should know about the impact of pregnancy on specific disorders as well as the best strategies for surveillance and safest treatments. It is important to be aware of the normal ranges of specific hormones in pregnancy to enable precise decisions to be made about whether hormones are present in excess or if women have deficiencies. This chapter will consider the commonest endocrine disorders that are seen in pregnancy.
Thyroid disease
The changes over time of specific thyroid hormones are shown in Figure 23.2. Human chorionic gonadotropin (hCG) shares some structural similarities to thyroid-stimulating hormone (TSH) and can stimulate the TSH receptor, and this causes a transient increase in tetraiodothyronine (thyroxine) and suppression of TSH in the first trimester. TSH levels will subsequently normalize once hCG levels plateau (Figure 23.2).
Also, conditions associated with higher hCG levels (e.g. molar pregnancy, multiple pregnancy, or hyperemesis gravidarum) can result in biochemical derangements suggestive of thyrotoxicosis. Thyroid-binding globulin levels increase in pregnancy, likely secondary to elevated oestrogen levels, and therefore total thyroxine measurement is not helpful, and free thyroxine measurement should be used. The normal ranges of thyroid function tests in each trimester of pregnancy are summarized in Table 23.6.
Autoimmune hypothyroidism
Autoimmune hypothyroidism is common, affecting 1% of pregnancies. If well controlled, women should have good pregnancy outcomes. However, overt hypothyroidism is associated with increased risks of adverse pregnancy outcome, including miscarriage, pre-eclampsia, placental abruption, and low birth weight, in addition to having an adverse impact upon the intelligence of the baby (25-27). Therefore it is important to ensure that affected women are adequately treated. However, overtreatment is associated with impaired fetal growth and can cause iatrogenic maternal hyperthyroidism, so overtreatment should be avoided as well (28). While it is clear that overt hypothyroidism causes impaired offspring intelligence, the impact of subclinical hypothyroidism on subsequent intelligence of the fetus is not clearly established. Although some older studies suggested that this could be an issue, there is no clear evidence for this in large, robustly performed studies. Indeed, a well-powered United Kingdom study that evaluated the impact of thyroxine replacement from the end of the first trimester for sub- clinical hypothyroidism did not show any difference in subsequent intelligence of the offspring at 3 years of age, and nor was there any impact upon birth weight or the rate of preterm birth (29). Therefore it is clearly important to ensure that women with hypothyroidism receive treatment with thyroxine to maintain their thyroid function tests in the normal range for pregnancy, but there is no evidence for treatment of women with normal thyroid function tests (28). There is also no evidence base for taking a TSH concentration of 2.5 mU/L as the threshold above which thyroxine replacement should be commenced in pregnant women with no history of thyroid disease, and recent studies have raised concerns that this practice will be result
Table 23.6 Normal ranges for thyroid function tests in pregnancy
| Normal range | I FT4 (pmol/L) | TSH (mU/L) |
| Non-pregnant | 11-23 | 0-4 |
| First trimester | 11-22 | 0-1.6 |
| Second trimester | 9-19 | 0.1-1.2 |
| Third trimester | 7-15 | 0.7-5.5 |
FT4, free thyroxine; TSH, thyroid-stimulating hormone.
Based on data taken from Parker et al. BJOG 1985;92:1234-38; Chan et al. BJOG 1988;95:1332-36; Soldin et al. Ther Drug Monit 2007;29:553-59.
in unnecessary treatment of up to 15% of pregnant women with no obvious thyroid disease (30).
There is some debate about whether all women need an increase in the dose of thyroxine in early pregnancy. As the thyroid-binding globulin concentration is elevated (Figure 23.2), some women will need an increase in thyroxine dose. A study that addressed the need for increased dose of thyroxine in 100 pregnancies in women with autoimmune hypothyroidism found that 50% of women needed more thyroxine, but in the majority of cases this was due to inadequate replacement prior to pregnancy, poor compliance, or recent diagnosis with insufficient time to optimize treatment, rather than a consequence of a gestation-specific need to increased dose (31). Therefore it is advisable to check the thyroid function tests as early as possible in pregnancy (and ideally prepregnancy) and to adjust the thyroxine dose in those that are deficient using normal ranges for pregnancy.
A small number of women present in early pregnancy with overt hypothyroidism and elevated TSH concentration above the normal range for pregnancy. This group of women are often concerned about the potential impact on the intelligence of their children. While there has been no study that specifically focuses on this group of infants, it is likely that the impact will be minimal if thyroxine replacement is optimized in the second and third trimester. Small studies of mild hypothyroxinaemia in the first trimester have shown that there is no impact on subsequent intelligence if the maternal thyroxine concentration returns to normal by the third trimester (32).
There is evidence that pregnant women positive for thyroid autoantibodies are more likely to have a miscarriage and preterm delivery (33). However, the underlying mechanism is not established. It is possible that this may relate to the coexistence of other autoimmune disorders that are associated with these adverse outcomes (e.g. antiphospholipid syndrome). To address the question of whether thyroxine treatment can reduce the risk of adverse pregnancy outcome in euthyroid women with positive thyroid peroxidase antibodies, the TABLET trial randomised 952 euthyroid women to 50 μg thyroxine or placebo from before conception and to be continued throughout pregnancy. This trial did not demonstrate any impact upon live birth rate (34). It is noteworthy that the study of thyroxine replacement for women with subclinical hypothyroidism (29) did not show any change in the rate of miscarriage or preterm labour in the group that received thyroxine replacement.
Hyperthyroidism
Hyperthyroidism affects 1 in 800 pregnancies. The majority of cases have Graves' disease. Rarer causes of hyperthyroidism in pregnancy are toxic nodule, thyroid adenoma, carcinoma, or subacute thyroiditis. Many clinical features of hyperthyroidism also occur in normal pregnancy, for example, palpitations, heat intolerance, and palmar erythema. However, eye signs and pretibial myxoedema are specific to autoimmune thyroid disease and weight loss does not occur in normal pregnancy. The biochemical features of hyperthyroidism are seen in women with hyperemesis gravidarum, but these do not occur in conjunction with clinical signs of thyroid hormone excess.
As most cases of hyperthyroidism occur in women of reproductive age, affected women are likely to need advice about pregnancy and conception. Carbimazole and propylthiouracil are used to treat hyperthyroidism, and both drugs are associated with an increased risk of congenital abnormalities, with the most recent studies suggesting the rate is twice the background rate (35, 36). There are more data to support the association of carbimazole/ methimazole with congenital abnormalities, but the 2013 study by Andersen et al. (36) demonstrated that this is a concern for propylthiouracil as well. This is important as guidance from the American Thyroid Association prior to this study recommended that propylthiouracil should be the treatment of choice in pregnant women on the basis of less evidence for an association with congenital malformations, despite the fact that use of propylthiouracil is rarely associated with fulminant hepatic failure in 1:10,000 adults and 1:2000 children (37). A pragmatic approach given the current data is to continue carbimazole in women who are already taking it prior to conception. Either carbimazole or propylthiouracil can be used for newly diagnosed cases in the first trimester of pregnancy, with appropriate advice about the risk of congenital malformations. It should also be explained that untreated thyrotoxicosis is associated with increased risks of fetal loss, growth restriction, preterm labour, and untreated women are at risk of thyroid storm, so treatment should be given. If the diagnosis is made after the first trimester, carbimazole is the most sensible choice. Many women with autoimmune hyperthyroidism find that their disease improves in pregnancy and in some the dose of antithyroid drugs may be reduced or even stopped. However, the requirement for treatment usually returns postpartum.
Women with autoimmune thyroid disease should have TSH receptor antibodies checked as they can cross the placenta and stimulate the fetal thyroid. In women who are taking antithyroid drugs this is unlikely to cause problems until after delivery as carbimazole and propylthiouracil also cross the placenta, but there is a risk of neonatal thyrotoxicosis 2-4 days postpartum. This is because the drugs will clear from the neonatal circulation rapidly, but the maternal antibodies will remain for approximately 3 months. As a consequence, it is important to involve the neonatologists in early fetal assessment. If a woman is not taking antithyroid drugs (e.g. because she has previously had surgery or radioiodine treatment), her pregnancy should be closely monitored for fetal hyperthyroidism or goitre because TSH receptor antibodies can cross the placenta and there will be no antithyroid drugs to prevent fetal disease. Monitoring should include assessment of fetal growth, fetal heart rate, and to ensure there is no goitre.
Carbimazole and propylthiouracil can be given to lactating women. There are no concerns about transfer to the baby with low, maintenance doses of either drug, but if high doses are used, the baby's thyroid function should be monitored.
Adrenal disease
Addison's disease
Adrenal insufficiency can be due to autoimmune destruction of the adrenal gland (Addison's disease), or can be the consequence of prolonged treatment with glucocorticoids causing adrenal suppression, or secondary to ACTH deficiency. Addison's disease is associated with the presence of adrenal antibodies and can have an insidious onset. It should be considered in women with other autoimmune diseases, in particular in those with unexplained lethargy, nausea, vomiting, hypotension or hyponatraemia. Pigmentation of palmar creases, the buccal mucosa, or scars may be seen. If suspected, a short tetracosactrin test should be performed. Glucocorticoid replacement can be given while waiting for the result. Replacement doses of hydrocortisone are usually given, with higher doses in the morning, and this should be decided in collaboration with an endocrinologist. Women with known hypoadrenalism should receive additional glucocorticoids at times of stress, vomiting, and to cover labour. They should also be advised to carry a steroid card and wear a medic-alert bracelet.
Cushing syndrome
Cushing syndrome is caused by glucocorticoid excess. It is caused by tumours of the pituitary or adrenal and by ingestion of excess doses of exogenous glucocorticoids. As adrenal tumours are reported to occur more commonly in pregnancy, likely a consequence of pituitary tumours influencing gonadotrophin secretion, Cushing syndrome will be considered under the heading of adrenal disease. However, the principles relating to complications are the same for both disorders. Cushing syndrome can be difficult to diagnose in pregnancy as many symptoms and signs are also seen in pregnant women, such as weight gain, striae, hypertension, glucose intolerance, and hirsutism. However, the striae in pregnancy are not usually as marked or coloured purple as they are in women with Cushing syndrome. The condition is associated with a number of adverse maternal and fetal outcomes (38-41). Severe hypertension may occur and impaired glucose tolerance or gestational diabetes mellitus affect 25% of cases. There is an increased rate of preterm labour and stillbirth (39). Maternal and fetal outcomes are improved in women who are treated surgically (39). Metyrapone and ketoconazole have also been used in pregnancy with good maternal and fetal outcomes (39, 40).
Phaeochromocytoma
Phaeochromocytoma is rare, affecting 1 in 54,000 pregnancies, but is a cause of severe morbidity and mortality that is important to recognize. The presenting symptoms include sweating, headache, and palpitations and the principal sign is hypertension. The condition may be missed due to these clinical features being attributed to pregnancy. However, the hypertension is often paroxysmal and in women with the classical symptoms and a suggestive history, plasma or urinary catecholamines, and metanephrines should be checked. If phaeochromocytoma remains undiagnosed, the maternal and fetal mortality can be as high as 50%, and this is markedly reduced with active management (41, 42). It is important to involve a multidisciplinary team in the management of women with phaeochromo- cytoma, particularly to ensure coordinated plans for delivery. The most important treatment is to commence an alpha-adrenoreceptor blocker, and the most commonly used drug is phenoxybenzamine. Once alpha-blockade has been achieved, some women require betablockade, but this must not be commenced before alpha-blockade has been achieved. Timing of surgery varies in different studies, with reports of adrenalectomy during the first 24 weeks of pregnancy, usually by a laparoscopic approach. Surgery can also be successfully achieved at the time of delivery or postpartum, providing adequate alpha-blockade has been achieved (43, 44). While there is no contraindication to vaginal delivery in well-controlled women, many cases are delivered by caesarean section. It is important that a team including intensive care physicians, obstetric anaesthetists, endocrinologists, obstetricians, and midwives are involved with peripartum care.
Primary aldosteronism
Primary aldosteronism, also called Conn syndrome, is caused by an aldosterone-producing tumour of the adrenal. The typical presenting features are hypertension and hypokalaemic alkalosis due to autonomous production of aldosterone and secondary renin suppression (45). This condition is rare in pregnancy. The commonest management strategy during pregnancy is to use potassium supplements and antihypertensive drugs with deferral of surgery until after delivery. Potassium-sparing antihypertensive agents (e.g. amiloride) may be used (41).
PituitaryZhypothalamic disease
Prolactinoma and other pituitary tumours
Prolactinomas are the commonest hormone-s ecreting tumours. They occur in women of reproductive age, and affected women frequently have menstrual irregularity, reduced fertility, and gal- actorrhoea. Large tumours may present with headache and visual symptoms secondary to compression of the optic chiasm. Prolactinomas respond well to dopamine agonist treatment, and women typically conceive rapidly once they commence treatment. Prolactinomas are subdivided according to size. The commoner subtype is microprolactinomas (measuring postpartum as well as at regular intervals during pregnancy. Some women with severe hepatic impairment (e.g. those with AFLP) can develop transient diabetes insipidus, likely a consequence of impaired hepatic degradation of placental vasopressin.
Parathyroid disorders
Primary hyperparathyroidism
Primary hyperparathyroidism occurs in approximately 8 per 100,000 women of reproductive age. In uncomplicated pregnancy, the maternal corrected calcium concentration in serum is usually slightly reduced, and this may explain why women with primary hyperparathyroidism in pregnancy often do not have the typical symptoms of nephrolithiasis or abdominal pain. However, up to 25% present with pre-eclampsia or pregnancy-induced hypertension (56). Maternal hyperparathyroidism is associated with a high perinatal complication rate, including stillbirth and neonatal tetany. A single-centre study of 77 pregnancies in 32 women with hyperparathyroidism reported a 48% fetal loss rate in 62 pregnancies where there was no surgical treatment. In contrast, in the 15 cases where parathyroidectomy was performed in the second trimester, there were good fetal outcomes (57). In this study, the fetal loss rate increased in pregnancies where the maternal serum calcium rate was higher. Given the association with fetal loss, parathyroidectomy is advisable in many cases. Alternatively, the serum calcium can be controlled in some cases with hydration and oral phosphate administration.