Management
Hormone therapy
Starting HT
There is now consensus that the minimum effective dose to alleviate symptoms should be used for the shortest duration of time.
The recommended starting doses of oestrogen are:
• 0.3 mg oral conjugated equine oestrogen
• 1 mg oral micronized oestradiol or oestradiol valerate
• 25-50 mcg transdermal oestradiol
• two (0.5 mg) metred doses of oestradiol gel
• 25-50 mcg implanted oestradiol.
Women who have a uterus must be prescribed combined HT (oestrogen and progesterone) because of the risk of endometrial hyperplasia and cancer associated with the effects of unopposed oestrogen on the endometrium. Those women who have had a total hysterectomy may use oestrogen-only preparations.
If the last menstrual period was more than 1 year ago, continuous combined preparations may be used; otherwise sequential (continuous oestrogen with progesterone for 12-14 days per month) preparations should be commenced. After 1 year of therapy, women on sequential preparations may change to continuous combined preparations if they wish to avoid a regular bleed.
Unscheduled vaginal bleeding is common in women with a uterus in the first 3 months of starting HT; however, it should be reported at review appointments.
Risks of HT
Breast
Breast cancer is the most common cancer in women and today there are an estimated 550,000 women in the United Kingdom living with breast cancer.
Female sex and age are the most important risk factors, but family history, particularly in association with BRCA1 and BRCA2 gene mutations, are associated with a high risk for developing breast cancer. Personal factors must also be considered: alcohol intake and obesity are considered to be risk factors, while physical activity and breast feeding may be protective. HT has also been implicated as a potential risk factor in randomized and observational studies.
Currently the question of linkage between breast cancer and HT use in women over the age of 50 years is complex. NICE suggests that we explain to women that HRT with oestrogen alone is associated with little or no change in the risk of breast cancer, but HRT with oestrogen and progesterone can be associated with an increase in risk (2). This risk of breast cancer attributable to HT is small, is duration dependent, and decreases after stopping. When counselling women it is also important to emphasize that the baseline risk of breast cancer will vary from women to woman, and other risk factors must be considered (Table 46.1).
Venous thromboembolism
Venous thromboembolism (VTE) is a condition comprising deep vein thrombosis and pulmonary embolism precipitated by conditions such as immobility, compression of the blood vessel, or increased blood viscosity that cause blood flow to slow.
HT is associated with a twofold increased risk of VTE, which appears to be greatest in the first year of use, and in those with increased body mass index (BMI).
Oral HT must undergo first-pass metabolism in the liver, and as such, affects the clotting cascade by increasing resistance to protein C and protein S (anticoagulants), and increasing fibrinogen, and as a result increasing the clotting risk. Transdermal preparations are absorbed directly into the bloodstream through the skin, bypassing this metabolism, and at standard doses are associated with a VTE risk no greater than baseline.
Transdermal preparations should be considered in those women with a BMI greater than 30 kg/m2, but those women at high risk of VTE (e.g. inherited thrombophilias) should be referred to a specialist before considering HT.
Prescribed non-hormonal alternatives for flushing
Monoamines have been shown to play an important role in the control of thermoregulation, and animal studies have shown that noradrenaline acts to narrow the thermoregulatory zone. Noradrenergic stimulation of the medial preoptic area of the hypothalamus in primates causes peripheral vasodilation, heat loss, and a drop in core temperature, similar to changes which occur in women during hot flushes.
Clonidine is an alpha-2-adrenergic agonist licensed for use as a non-hormonal alternative for the treatment of flushing. It has been shown, in a meta-analysis of poor to fair quality trials, to reduce hot flush frequency and severity at 4 weeks and at 8 weeks (24); however, adverse effects include dry mouth, insomnia, and drowsiness.
Serotonin is involved in many bodily functions including mood, anxiety, sleep, sexual behaviour, and thermoregulation. Oestrogen withdrawal is associated with decreased blood serotonin levels, and short-term oestrogen therapy has been shown to increase these levels.
A meta-analysis assessed two RCTs comparing paroxetine to placebo and concluded that paroxetine was more effective than placebo in reducing the frequency and severity of hot flushes (24). This same meta-analysis assessed a further two RCTs comparing venlafaxine and placebo. There was an improvement in quality of life in one study, despite no reduction in frequency of flushes, and a decrease in hot flush frequency compared with placebo, in the other. Adverse effects included dry mouth, constipation, decreased appetite, nausea, and sleeplessness. Nausea typically improves in 2-3 days, and can be improved by titrating the dose slowly.
Table 46.1 Absolute risks of breast cancer for different types of HRT compared with no HRT (or placebo), different durations of HRT use, and times since stopping HRT for menopausal women
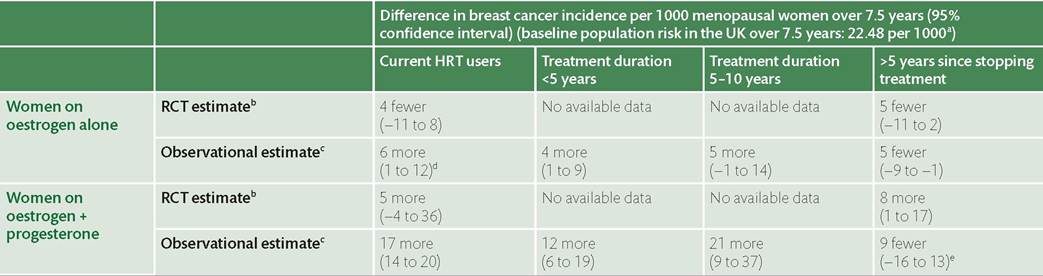
a Office of National Statistics (2010) breast cancer incidence statistics.
b For women aged 50-59 years at entry to the RCT
c Observational estimates are based on cohort studies with several thousand women.
d Evidence on observational estimate demonstrated very serious heterogeneity without plausible explanation by subgroup analysis.
e Evidence on observational estimate demonstrated very serious imprecision in the estimate of effect.
Reproduced from National Institute for Health and Care Excellence (NICE). Menopause: Diagnosis and Management of Menopause. NICE guideline [NG23]. London: NICE: 2015. Available at: https://www.nice.org.uk/guidance/ng23.
NICE does not advocate the use of SSRIs/SNRIs or clonidine as first-line therapy for vasomotor symptoms alone (2).
Use of these drugs in women with breast cancer using tamoxifen is common; therefore, consideration must be given to potential interactions. Tamoxifen must be metabolized by the cytochrome P450 enzyme system, predominantly cytochrome P450 isoenzyme 2D6 (CYP2D6), to become active, and CYP2D6 is inhibited to varying degrees by SSRIs. Paroxetine is an exceptionally potent inhibitor, whereas sertraline inhibits to a lesser degree and citalopram and escitalopram are only weak inhibitors. Evidence is conflicting on the success rates of tamoxifen in preventing recurrence of breast cancer when using a concurrent SSRI. For those women who need to begin treatment with an SSRI for depression, citalopram or escitalopram may be the safest choice; however, improvements in flushing are better with venlafaxine and desvenlafaxine, and these appear to be safe choices.
Over-the-counter remedies
A Cochrane systematic review of phytoestrogens included five trials in a meta-analysis, which demonstrated no significant decrease in the frequency of hot flushes (25).
Black cohosh is a native American herb that is thought to behave as a selective oestrogen receptor modulator with mild central oestrogenic effects. A meta-analysis of several short-term and relatively small RCTs comparing black cohosh use with placebo ‘revealed a trend towards reducing vasomotor symptoms', but only in cases of mild to moderate symptoms (26). This was particularly notable when hot flushes were associated with sleep and mood disturbances. This was confirmed in another 12-week study of 304 women in addition to improvements in mood, sleep disorders, sexual disorders, and sweating.
In contrast, however, the recent Herbal Alternatives for Menopause Trial (HALT) (27) which compared black cohosh to both placebo and oestrogen replacement over 12 months suggested that black cohosh was ineffective in relieving vasomotor symptoms. It is, however, important to exercise caution as there is limited information on its potential to influence breast cancer development or progression.NICE recommends that, while there is some evidence for the use of black cohosh and isoflavones, it is important to explain to women that there are multiple preparations, these preparations may vary, and their safety is uncertain (2). In addition, interactions with other medicines have been reported.
Vitamin E and evening primrose oil are no better than placebo at reducing the frequency or severity of hot flushes (28, 29).
Alternative therapies
Acupuncture is a popular form of complementary medicine used by women in menopause. It can be defined as the insertion of needles into the skin and underlying tissues at particular sites, known as acupoints, for therapeutic or preventative purposes. A systematic review of six randomized control trials revealed only one with favourable results of acupuncture and this trial was considered too small to generate reliable findings (30).