38 Menstrual Disorders: Endometriosis, Dysmenorrhea, and Premenstrual Dysphoric Disorder
Irene Woo
Melissa Yates
ENDOMETRIOSIS
Endometriosis is defined as the extrauterine presence of functioning endometrial glands and stroma. It is most commonly found in the ovaries but also located in the pouch of Douglas, vesicouterine space, uterosacral ligaments, and surrounding pelvic peritoneum.
It is less commonly seen in laparotomy and episiotomy scars; appendix, pleural, and pericardial cavities; and the cervix.P.504
Theories of the Pathogenesis of Endometriosis
• The etiology of endometriosis is unknown. Several theories involving anatomic, immunologic, hormonal, and genetic factors have been postulated.
• Retrograde menstruation: Sampson's original theory suggests that endometriosis is related to retrograde menstruation of endometrial tissue via the fallopian tubes into the peritoneal cavity. Support for this theory is as follows:
• Blood flow from the fimbriated ends of fallopian tubes has been visualized during laparoscopy (seen in 90% of women with patent fallopian tubes).
• Endometriosis is most often found in the dependent portions of the pelvis.
• Incidence of endometriosis is higher in women with obstruction to normal outward menstrual flow (e.g., cervical stenosis).
• Endometriosis is more common in women with shorter menstrual cycles or longer duration of flow, providing more opportunity for endometrial implantation.
• Immunologic factors: Increasing data suggest that specific immunologic factors at the site of endometrial implants play a major role in determining whether and to what extent a patient will develop the disease. These factors are thought to explain the attachment and proliferation of the endometriotic cells.
• Inflammatory factors: Elevated levels of interleukin-6 and tumor necrosis factor-α have been noted in the peritoneal fluid of endometriosis patients. Interleukin-8 may help in the attachment of endometrial implants in the peritoneum and is also an angiogenic agent.
• Hormonal factors: Unlike normal endometrial tissue, endometriotic implants can produce aromatase, leading to extraovarian estrogen production. This may explain why endometriosis can recur in women who have undergone hysterectomy and bilateral salpingo-oophorectomy. Prostaglandin E2, a proinflammatory compound, has been shown to be a powerful inducer of aromatase activity in endometriotic implants.
• Coelomic metaplasia: This theory postulates that totipotential cells of the ovary and peritoneum are transformed into endometriotic lesions by repeated hormonal or infectious stimuli. This may explain the finding of endometriosis in mature teratomas and extraperitoneal sites.
• Lymphatic spread: One study showed that 29% of women with endometriosis at autopsy had positive pelvic lymph nodes for the disease. Thus, lymphatic spread may be another mechanism to explain why endometriotic implants can be found in remote anatomic areas, such as the lung.
• Genetic factors: Women who have a first-degree relative with endometriosis have a sevenfold greater risk of developing endometriosis. The mode of inheritance is most likely multifactorial.
Patient Characteristics
• Mean age at diagnosis is 25 to 30 years. The greatest incidence has been observed in nulliparous women with early age at menarche and shorter menstrual cycles. Increased parity and greater cumulative lactation have been shown to be protective factors in development of endometriosis.
• Although some women with endometriosis are asymptomatic, the most common symptoms are infertility and pelvic pain.
• Infertility: Incidence of endometriosis is believed to be 20% to 40% among infertile couples, with some studies showing endometriosis to be 7 to 10 times more likely in this patient group. Often, asymptomatic patients undergoing laparoscopy for infertility often will be diagnosed with mild endometriosis.
P.505
• Pelvic pain: Seventy-one percent to 87% of women with chronic pelvic pain have endometriosis.
Endometrial lesions can lead to chronic inflammation with increase in inflammatory cytokines and subsequent overproduction of prostaglandins, both of which can be a source of pain. Furthermore, endometriotic lesions may harbor high levels of nerve growth factors. However, the severity of pelvic pain does not correlate with the amount of endometriosis present. The pain typically associated with endometriosis is central, deep, and often in the rectal area. Unilateral pain may be compatible with lesions in the ovary or pelvic sidewall. Dysuria or dyschezia can result from urinary or intestinal tract involvement, respectively, and oftentimes predict deeply infiltrating endometriosis. Forty percent to 50% of patients with deep dyspareunia have been found to have endometriosis.• Incidence of endometriosis in patients with dysmenorrhea is believed to be 40% to 60%. One study found endometriotic implants in approximately 70% of teenagers who underwent laparoscopy for chronic pelvic pain. Dysmenorrhea often starts before the onset of menstrual bleeding and continues until bleeding abates.
Abnormal Clinical Findings Associated with Endometriosis
• Nodularity of the uterosacral ligaments, which are often tender and enlarged
• Painful swelling of the rectovaginal septum
• Pain with motion of the uterus and adnexa
• Fixed retroverted uterus and large immobile adnexa are indicative of severe pelvic disease.
Confirmation of Diagnosis
• Definitive diagnosis can be made only through histology and examination of lesions removed at the time of surgery. Histology reveals both endometrial glands and stroma. Hemosiderin-laden macrophages have been identified in 77% of endometriosis biopsy specimens. Pelvic ultrasonography can be useful in differentiating the presence of endometriomas from other adnexal masses.
• Experienced clinicians often presumptively diagnose endometriosis based on clinical history and timing of symptoms. First-line therapy with oral contraceptive pills can be initiated without a surgical diagnosis; however, when this fails, a thorough survey of the pelvis via diagnostic laparoscopy is recommended.
Endometriotic lesions classically appear as blue-black powder-burn visual appearance; however, studies have reported a marked discrepancy in appearance of the lesions and the histology. Nonclassic lesions may appear vesicular, red, white, tan, or nonpigmented. The presence of defects in the peritoneum (usually scarring overlying endometrial implants) is known as Allen-Masters syndrome. Endometriomas, “chocolate cysts,” appear filled with dark brown blood.Medical Treatment
• Estrogen stimulates the growth of endometriotic implants similar to its effect on normal endometrial tissue. Medical therapy is aimed at suppressing ovarian estrogen stimulation by interrupting the hypothalamic- pituitary-ovarian axis. Inhibition of ovulation by gonadotropin suppression removes the stimulation of endometriosis by cycling sex steroids.
• Oral contraceptive pills (OCPs): These pills cause anovulation and decidualization, which results in atrophy of endometrial tissue. Symptomatic relief of pelvic pain and dysmenorrhea is reported in 60% to 95% of patients. However, the
P.506 estrogenic component may potentially stimulate growth and increase pain during the first few weeks of treatment. The recommended dose is a 20- to 30-mg ethinyl estradiol pill. Continuous combined OCPs can provide significant pain relief in patients suffering mainly from dysmenorrhea.
• Gonadotropin-releasing hormone (GnRH) agonists: when given over the longterm suppress pituitary function by downregulating pituitary GnRH receptors. This interruption of the hypothalamic-pituitary- ovarian axis produces a “medical oophorectomy” or “pseudomenopause.” Three available agents are leuprolide acetate (Lupron Depot), 3.75 mg by intramuscular injection every month for 6 months; nafarelin acetate nasal spray, 200 mg twice daily for 6 months; and goserelin acetate (Zoladex), 3.6 mg subcutaneous implants at 28-day intervals for 6 months. Side effects are related to the hypoestrogenic state. The U.S. Food and Drug Administration (FDA) has approved the use of a 12-month course to avoid the long-term consequences of the hypoestrogenic state on bone metabolism and lipid profile changes.
• Add-back therapy: largely used for minimization of side effects. Numerous studies have demonstrated the efficacy of adding back combined estrogen/progesterone to patients on GnRH agonist therapy. Patients receiving add-back therapy have significantly less vasomotor side effects and bone mineral density loss over a 6-month period while still benefiting from pain improvement from their endometriosis. Vaginal bleeding is a side effect of add-back therapy and is dose dependent. A postmenopausal estrogen-progesterone add-back regimen can be used, such as daily conjugated estrogen 0.625 mg together with medroxyprogesterone acetate 2.5 mg. An alternate regimen is 2.5 mg norethindrone acetate daily.
• Progestins: Progestins inhibit ovulation by luteinizing hormone (LH) suppression and, eventually, may induce amenorrhea (Table 38-1). They also suppress endometriosis through decidualization and atrophy of endometrial tissue. Progesterone therapy can be continued for suppression of endometriosis symptomatology; however, health care providers should be aware of the potential for bone demineralization with long-term progesterone use.
• Danazol (Danocrine): a derivative of the synthetic steroid 17α-ethinyl testosterone. It suppresses the midcycle LH surge, inhibits steroidogenesis in the human corpus luteum, and produces a high-androgen and low-estrogen environment that does not support the growth of endometriosis. Approximately 80% of patients experience relief or improvement in symptoms within 2 months of beginning danazol treatment. Androgenic side effects greatly reduce compliance. Recurrence of symptoms is almost 50% within 4 to 12 months after discontinuation of therapy. Adverse side effects occur in approximately 15% of women taking
danazol.
• Aromatase inhibitors: Recent studies have evaluated the third-generation aromatase inhibitors, Ietrozole and anastrozole, for treatment of endometriosis refractory to other modalities. They are used alone or combined with GnRH agonists.
These medications have been shown to decrease circulating estrogen levels by 50%. The most significant side effect is decreased bone density, which is not necessarily ameliorated with the use of calcium and vitamin D; however, evidence at this point is conflicting with regard to the overall decrease in bone density, requiring further study.• Additional side effects include vaginal spotting, hot flushes, headaches, and mood swings, which are better tolerated compared to the side effects of GnRH agonists.
• Pain control with nonsteroidal anti-inflammatory drugs (NSAIDs) inhibits prostaglandin production by ectopic endometrium. NSAIDs are a good first-line agent, especially when the diagnosis of endometriosis has not been firmly established.
P.507
TABLE 38-1 Medical Management of Endometriosis
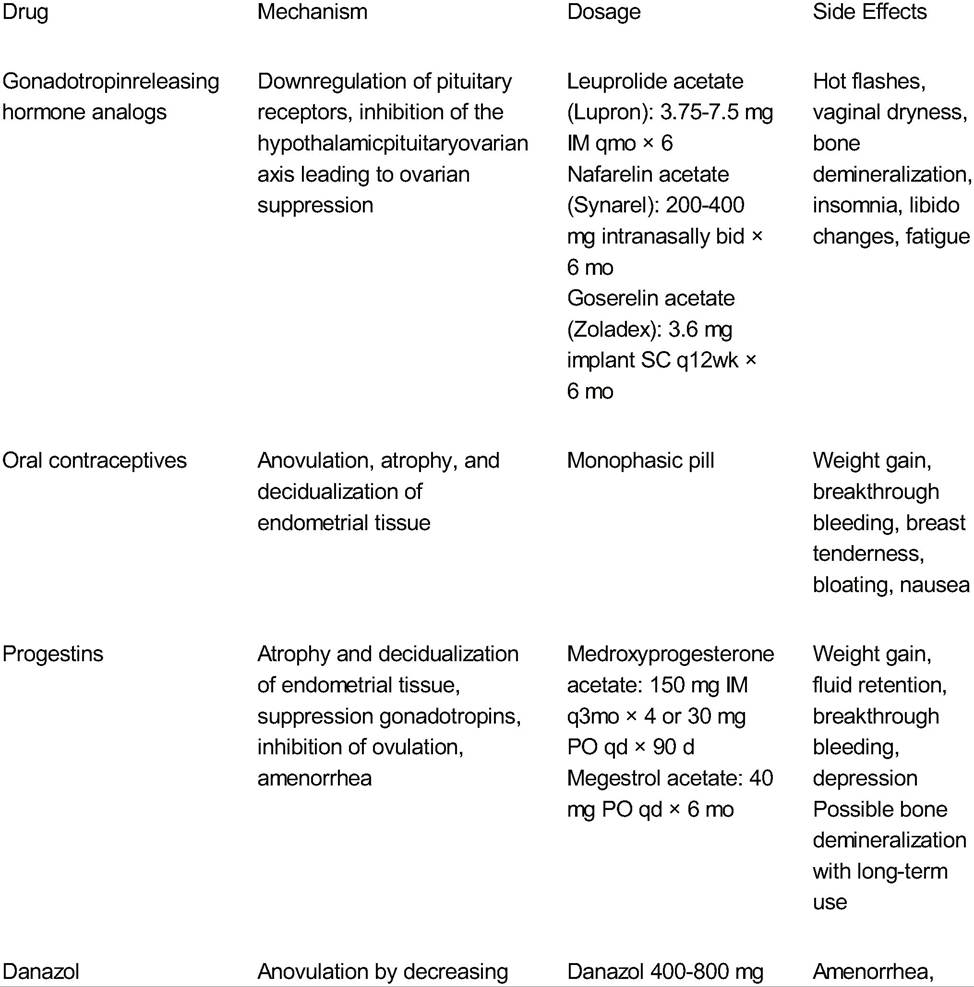
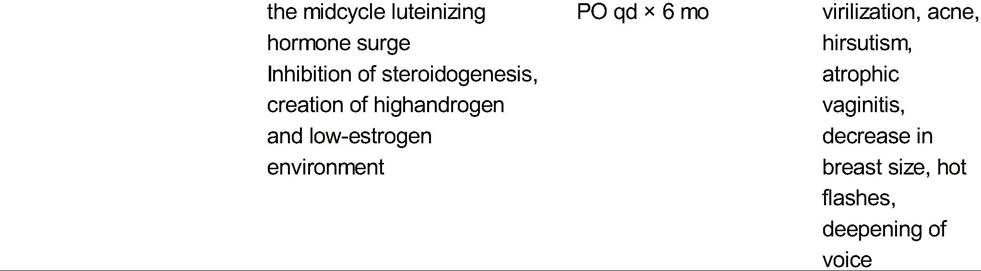
IM, intramuscularly; bid, twice a day; SC, subcutaneously; qd, every day.
Adapted from American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 114: management of endometriosis. Obstet Gynecol 2010;116:223-236.
P.508
Surgical Treatment
• Definitive surgery entails total abdominal hysterectomy with bilateral salpingooophorectomy, excision of peritoneal surface lesions or endometriomas, and lysis of adhesions. A “semidefinitive” procedure that preserves an uninvolved ovary is another option because it avoids the long-term risks of surgical menopause. However, there is a sixfold increased risk of developing recurrent symptoms and an eightfold reoperation rate to remove the remaining ovary.
• Hormone replacement therapy (HRT) after definitive surgery for the prevention of surgical menopausal symptoms is also considered safe and does not appear to increase the risk of recurrence of endometriosis.
• Conservative surgery is usually reserved for patients with endometriosis-related pain but who desire future fertility. Improvement in symptoms is often achieved with laparoscopic excision or destruction of endometrial implants via laser vaporization, electrocoagulation, and thermal coagulation. Although there is significant short-term improvement in pain, a few studies have shown at 3 years postoperation, approximately 30% of patients will require additional surgeries. Despite this, the American College of Obstetricians and Gynecologists does recommend, in patients with normal ovaries, removal of uterus and endometriotic lesions with ovarian conservation.
Endometriosis and Infertility
• The exact incidence of infertility caused by endometriosis is unknown.
• Theories on the physiologic changes caused by endometriosis that affect fertility potential include abnormal folliculogenesis, elevated oxidative stress, altered immune function, alterations in peritoneal fluid cytokines, and decreased presence of integrins during the implantation phase, thus decreasing endometrial receptivity. Together, these factors decrease oocyte quality and impair fertilization and implantation.
• Fewer oocytes are retrieved when an endometrioma is present but the pregnancy rate with in vitro fertilization (IVF) is not greatly altered and the risk of removing segments of normal ovarian cortex along with the cystectomy must be weighed against the benefit.
Endometriosis and Ovarian Malignancy
• The prevalence of endometriosis in patients with epithelial ovarian carcinoma, especially in endometrioid and clear cell types, is higher than that of the general population. Conversely, ovarian carcinoma has been documented in 0.3% to 0.8% of patients with endometriosis.
• The pathology of endometriosis exhibits many of the characteristics of neoplastic lesions: reduced cell cycle inhibitor activity, ability to resist apoptosis, angiogenic potential similar to malignant neoplasms, and ability to invade surrounding tissue.
• Endometriosis implants may represent a precancerous state. Endometriosis is related to a chronic inflammatory state involving cytokine release, which can lead to malignant mechanisms. Both atypical endometriosis and ovarian cancers associated with endometriosis have p53 overexpression; the Ki-67 index was noted to be three times higher in atypical endometriosis.
• Clear cell and endometrioid carcinoma are the most common histologies associated with ovarian endometriosis. Numerous studies reviewing the histologic slides of endometriosis demonstrate simultaneous atypical endometriosis and malignancy.
P.509
• Endometriosis-associated ovarian carcinoma is found at an earlier stage and lower grade and is associated with a better overall survival rate than sporadic ovarian cancer.
• There is a definite causal relationship between endometriosis and specific histologic types of ovarian cancer. However, the low magnitude of the conferred risk is consistent with the view that ectopic endometrium undergoes malignant transformation with a frequency similar to its eutopic counterpart.
• At present, malignant transformation of endometriotic lesions is a recognized mechanism in the development of ovarian cancer. However, definitive surgery to remove all visible evidence of endometriosis is not recommended as a prophylactic means of reducing the development of ovarian malignancy. Rather, long-term use of oral contraceptives is the preferred method of cancer risk reduction, as an 80% lower occurrence of ovarian cancer in women with endometriosis has been shown in patients using the drug for >10 years.
DYSMENORRHEA
• Primary dysmenorrhea is painful menstruation with no evidence of hormonal or anatomic pathology. Secondary dysmenorrhea has a demonstrable cause.
• Risk factors include young age (and anger that cause conflict with other people
î Lack of interest in things she used to enjoy
P.511 î Having problems concentrating
î Lack of energy
î Appetite changes, overeating, or cravings
î Having trouble sleeping or sleeping too much
î Feeling overwhelmed
î Physical symptoms such as tender or swollen breasts, headaches, joint or muscle pain, bloating, and weight gain
• Symptom onset occurs anytime in the 2 weeks prior to the onset of bleeding, continues to the start of bleeding, and resolves after a day or two of menstrual flow.
• The exact physiologic cause of premenstrual disorders is unknown. Most frequently cited theories include neuroactive progesterone metabolite, γ-aminobutyric acid receptor modulation, and critical reduction in serotonergic function during the luteal phase.
Evaluation and Diagnosis
• Dysmenorrhea, depression and anxiety disorders, menstrual migraine, cyclic mastalgia, irritable bowel syndrome, and hypothyroidism may all present with mood or physical disturbances similar to those that manifest with PMS/PMDD. See also Chapter 30.
• There are no laboratory or physical exam findings required to make the diagnosis. Rather, these tests are used to rule out other causes of similar symptoms. Hormone levels (estrogen, progesterone, LH, folliclestimulating hormone [FSH]) do not vary between women with and without PMS/PMDD; thus, there is no use in obtaining these values.
• For diagnosis of PMS, symptoms must begin at least 5 days before menses, persist for three menstrual cycles in a row, and end within 4 days after menses starts. It must also interfere with some of the patient's normal activities.
• Such logs are helpful for clinicians in order to determine whether the reported symptoms are limited to the luteal phase or are present throughout the cycle, suggesting a general medical condition. Additionally, they are helpful for patients for instituting self-help strategies and for anticipating symptoms.
Treatment
• Because PMS/PMDD is a chronic problem, adverse effects, cost, and severity of symptoms should all be considered before employing a specific treatment.
• Lifestyle changes are probably most appropriate for mild to moderate PMS/PMDD. Regular aerobic exercise; relaxation therapy; stress reduction; sufficient sleep; dietary limitation of caffeine, alcohol, and salt; and increased consumption of complex carbohydrates during the luteal phase have been shown to reduce the severity of symptoms.
• Dietary supplements (especially St. John's wort but also ginkgo and kava) are somewhat effective for mild to moderate PMS but ineffective for PMDD. However, patients should be aware of their potential adverse effects (especially the affect of St. John's wort on the effectiveness of OCPs).
• In several small randomized trials, NSAIDs taken in the luteal phase have been shown to decrease all physical symptoms with the exception of breast tenderness.
• Yaz, the combined OCP containing drospirenone and 20 mg of ethinyl estradiol, was recently approved by the FDA for treatment of PMDD and has been shown effective in treating mood and physical and behavioral symptoms of PMDD.
P.512
• Selective serotonin reuptake inhibitors are the most effective pharmacologic treatment for moderate to severe PMS and PMDD. Continuous dosing exerts a greater inhibition of symptoms than intermittent dosing. Fluoxetine, sertraline, citalopram, and paroxetine all demonstrated a statistically significant improvement in symptoms.
SUGGESTED READINGS
Allen C, Hopewell S, Prentice A. Non-steroidal anti-inflammatory drugs for pain in women with endometriosis. Cochrane Database Syst Rev 2005;(4):CD004753.
American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 110: noncontraceptive uses of hormonal contraceptives. Obstet Gynecol 2010;115(1 ):206-218.
American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 114: management of endometriosis. Obstet Gynecol 2010;116(1 ):223-236.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed.
Washington, DC: American Psychiatric Association, 1994:717-718.
Balasch J, Creus M, Fabregues F, et al. Visible and non-visible endometriosis at laparoscopy in fertile and infertile women and in patients with chronic pelvic pain: a prospective study. Hum Reprod 1996;11:387-391.
Barbieri RL, Niloff JM, Bast RC Jr, et al. Elevated serum concentrations of CA-125 in patients with advanced endometriosis. Fertil Steril 1986;45(5):630-634.
Brosens I, Puttemans P, Campo R, et al. Non-invasive methods of diagnosis of endometriosis. Curr Opin Obstet Gynecol 2003;15(6):519-522.
Diwadkar GB, Falcone T. Surgical management of pain and infertility secondary to endometriosis. Semin
Reprod Med 2011 ;29(2): 124-129.
Namnoum AB, Hickman TN, Goodman SB, et al. Incidence of symptom recurrence after hysterectomy for endometriosis. Fertil Steril 1995;64:898-902.
Sagsveen M, Farmer JE, Prentice A, et al. Gonadotrophin-releasing hormone analogues for endometriosis: bone mineral density. Cochrane Database Syst Rev 2003;(4):CD001297.
Sampson JA. Peritoneal endometriosis due to menstrual dissemination of endometrial tissue into the peritoneal cavity. Am J Obstet Gynecol 1927;71:422-469.
Shakiba K, Bena JF, McGill KM, et al. Surgical treatment of endometriosis: a 7-year follow-up on the requirement for further surgery. Obstet Gynecol 2008; 111:1285-1292.
Somigliana E, Vigano' P, Parazzini F, et al. Association between endometriosis and cancer: a comprehensive review and a critical analysis of clinical and epidemiological evidence. Gynecol Oncol 2006;101 (2):331-341.
Worley MJ, Welch WR, Berkowitz RS, et al. Endometriosis-associated ovarian cancer: a review of pathogenesis. Int J Mol Sci 2013;14:5367-5379.
Yeung P Jr, Sinervo K, Winer W, et al. Complete laparoscopic excision of endometriosis in teenagers: is postoperative hormonal suppression necessary? Fertil Steril 2011;95(6):1909-1912, 1912.e1.
U.S. Food and Drug Administration. Lupron and Lupron Depot (leuprolide acetate) injection. U.S. Food and
Drug Administration Web site. http://www.fda.gov/safety/medwatch/safetyinformation/ucm291032.htm. Accessed May 21, 2013.