Methods of intrapartum fetal monitoring
About one out of every ten newborns who later develop cerebral palsy has evidence of isolated intrapartum hypoxia as a cause. Despite its low specificity for hypoxia, cardiotocography (CTG) continues to be the central documentary evidence for all claims for fetal asphyxia (1, 2).
Although it is clear that in some of the cases interventions may have prevented or decreased the severity of cerebral palsy, it has been shown overall that fetal heart rate (FHR) patterns are poor predictors of cerebral palsy (1-4). The low specificity of CTG for fetal hypoxia therefore necessitates secondary or definitive tests to confirm fetal acid-base status in labour such as fetal blood sampling, vibroacoustic stimulation, fetal oximetry, or ST segment analysis of the fetal electrocardiogram (ECG).
Intermittent auscultation
Intrapartum intermittent auscultation of the FHR is probably the commonest and most widely used method of fetal surveillance in labour throughout the world. Its advantages include the ease of monitoring, low cost, and minimal training requirements.
When performing auscultation, a Doppler device is preferable to a Pinard stethoscope. The mother should be asked about fetal movements and a baseline FHR recorded. An attempt should then be made to feel the fetal movements per abdomen and look for any FHR accelerations associated with these movements. When the uterus contracts, the presence or absence of any obvious decelerations immediately after the contractions should be noted and an attempt made to estimate the depth and duration of deceleration, and whether it recurs with the next few contractions with the mother on her left lateral side. FHR accelerations associated with fetal movements and no decelerations should reassure the mother and the healthcare professional of good fetal health. Subsequent observations should be auscultation of FHR soon after contraction every 15 minutes for 1 minute in the first stage of labour and every 5 minutes or after every alternate contraction in the second stage.
A change to electronic monitoring should be considered (where available) when recurrent or prolonged decelerations or abnormalities of baseline especially a rising baseline rate are detected on auscultation.Randomized controlled trials (RCTs) undertaken in the 1970s and 1980s demonstrated no differences in the perinatal mortality, Apgar scores, or neonatal intensive care unit admissions when one- to-one intermittent auscultation (every 15 minutes in the first stage of labour and every 5 minutes in the second stage of labour) was compared to EFM (5-10). However it is important to recognize that the results with intermittent auscultation are poor as compared to EFM when there is no one-to-one care. Thus, in most situations of a busy maternity service when it is not possible to ensure that each healthcare personnel attend a single woman in labour, the success of auscultation may be less than what was observed in RCTs.
As part of the initial assessment (at first contact with the woman in labour, and at each further assessment), the National Institute for Health and Care Excellence (NICE) guideline recommends auscultation of FHR for a minimum of 1 minute immediately after a contraction. The maternal pulse should be palpated to differentiate between maternal heart rate and FHR. Any accelerations and decelerations, if heard, should be documented clearly (11). The biggest drawback of auscultation is that although it may provide the baseline FHR and indicate the presence of accelerations/decelerations, baseline variability is not audible to the unaided ear and quantifica- tion/description of the type of decelerations is difficult. It also does not provide objective evidence such as a paper trace for medicolegal purposes.
Electronic fetal monitoring
Since its introduction in the 1960s, the intrapartum and admission use of EFM has increased rapidly in well-resourced countries. Despite its shortcomings, continuous intrapartum CTG remains the predominant method of intrapartum fetal surveillance wherever facilities allow.
This is because of medicolegal reasons (it provides a graphical trace record of the FHR throughout labour), also because it is helpful in identifying possible fetal hypoxia during labour and because there is no other better independent monitoring modality yet established for widespread clinical use. When intrapartum CTG was introduced in clinical practice, it was the expectation that this method would reduce the incidence of cerebral palsy and intellectual disability by 50%. However, this dream was not realized. As reviewed in 2002 by Freeman (3), the disappointing outcomes associated with EFM may be because (a) the asphyxial damage may begin before labour, (b) acute asphyxia associated with events such as prolapsed cord or ruptured uterus may not sometimes allow sufficient time for intervention before damage is done, (c) a large proportion of surviving very low birth weight infants contribute to the existing cases of cerebral palsy, (d) a fetal inflammatory response to infection/pyrexia may be responsible and (e) the amount of asphyxia required to cause permanent neurological damage is very near the amount that causes fetal death so the number of patients who develop cerebral palsy caused by intrapartum asphyxia is probably quite small. It is also possible that in some of the studies, the study sample size was not large enough.Evidence
One large analysis of initial studies concluded that intrapartum fetal death was significantly less common in patients who were observed with electronic FHR monitoring than in those who had auscultation without one-to-one care (12). However, subsequent RCTs comparing EFM with intensive one-t o-one auscultation in term patients found no differences with respect to perinatal mortality, Apgar scores, or neonatal intensive care unit admissions (5-10). The effectiveness of continuous CTG in labour was also a subject of a Cochrane systematic review in 2013 which included 13 trials (randomized and quasi-randomized controlled trials with >37,000 women).
Compared with intermittent auscultation, continuous CTG showed no significant improvement in overall perinatal death rate (risk ratio (RR) 0.86; 95% confidence interval (CI) 0.59-1.23; n = 33,513; 11 trials), but was associated with a halving of neonatal seizures (RR 0.50; 95% CI 0.31-0.80; n = 32,386; nine trials). There was no significant difference in cerebral palsy rates (RR 1.75; 95% CI 0.84-3.63; n = 13,252; two trials). There was a significant increase in caesarean sections associated with continuous CTG (RR 1.63; 95% CI 1.29-2.07; n = 18,861; 11 trials). Women were also more likely to have an instrumental vaginal birth (RR 1.15; 95% CI 1.01-1.33; n = 18,615; 10 trials). Data for subgroups of low-risk, high-risk, preterm pregnancies and high-quality trials were consistent with overall results. Access to fetal blood sampling did not appear to influence the difference in neonatal seizures nor any other prespecified outcome. The authors suggested that the real challenge was how best to convey this uncertainty to women to enable them to make an informed choice without compromising the normality of labour (13). Most clinical guidelines that subsequently emerged recommended continuous CTG for women at high risk and intermittent auscultation for those considered at low risk in labour.Challenges of electronic fetal monitoring
Intrapartum monitoring of FHR presents its own challenges. The report from the Centre for Maternal and Child Enquiries in 2008 and the Chief Medical Officer’s report in 2006—‘Intrapartum related deaths: 500 missed opportunities’ in the United Kingdom have identified problems with interpreting and acting on fetal surveillance in labour (14, 15). It is not uncommon in clinical practice to unexpectedly find normal-size babies born asphyxiated while those delivered operatively for severe fetal distress to be born in good condition. Herein lie the challenges for healthcare professionals trying to interpret the intrapartum FHR patterns and base their management decisions on them.
Presently, there appears to be a consensus regarding the reassuring value of a normal reactive CTG pattern (Figure 27.1) with accelerations, normal baseline rate, and normal baseline variability without any decelerations. On the other hand, patterns containing absent variability associated with persistent late or variable decelerations (Figure 27.2) are considered ominous and those with shallow late decelerations (Figure 27.3) and prolonged decelerations where FHR is less than 80 beats per minute (bpm) for longer than 15 minutes (Figure 27.4) are considered preterminal and indicate the need for immediate delivery to avoid hypoxic damage. However, the clinician is often challenged with a CTG trace that falls between these two extremes and needs to decide the further action depending on their interpretation of the findings based on overall clinical assessment of the case. Besides, hypoxia may not be the only damaging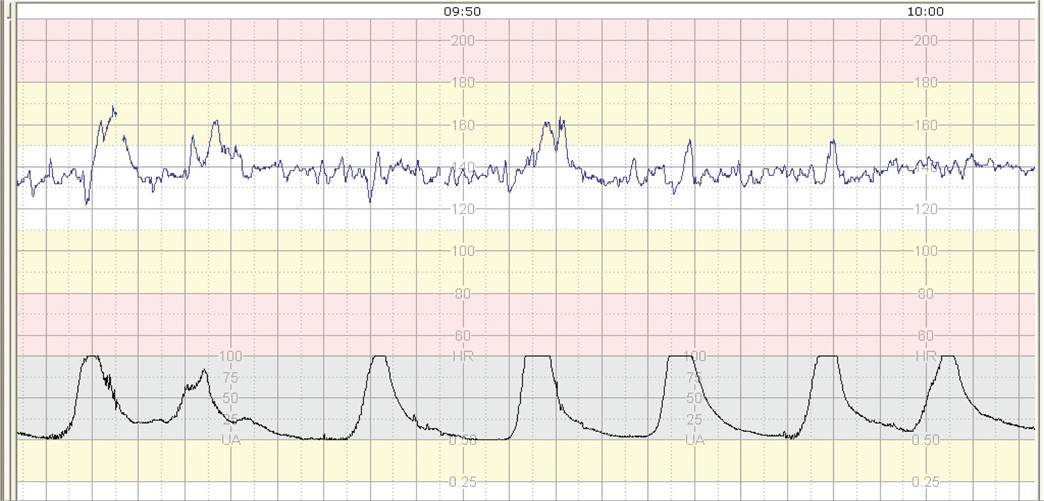
Figure 27.1 A normal reactive CTG with normal baseline rate, baseline variability accelerations, and no decelerations.


Figure 27.2 An ominous trace with reduced baseline variability, tachycardia, no accelerations, and variable decelerations.
factor during labour. Recent studies suggest a fetal inflammatory response due to infection/pyrexia as a cause of central nervous system damage (16, 17). The patterns of CTG associated with such insults may vary considerably and need to be carefully interpreted based on the overall clinical scenario.
Admission test
The labour admission test (LAT) is a test of fetal well-being that is performed when a woman with a low-risk pregnancy is admitted in labour. Its aim is to assess fetal well-being at the onset of labour and identify those fetuses that may be already hypoxic or may not
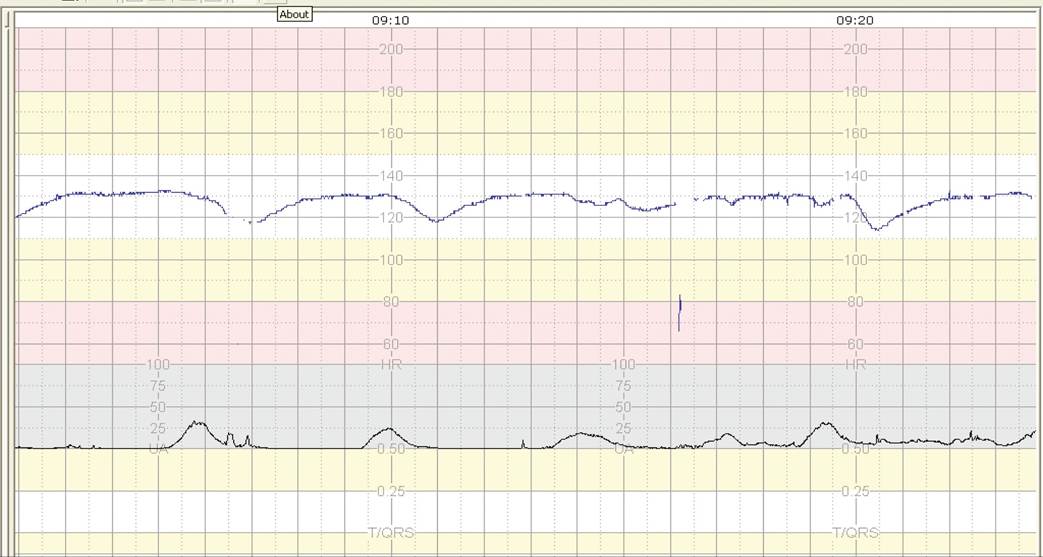
Figure 27.3 Abnormal CTG trace with tachycardia, markedly reduced baseline variability, and shallow late decelerations—a pre-terminal trace.
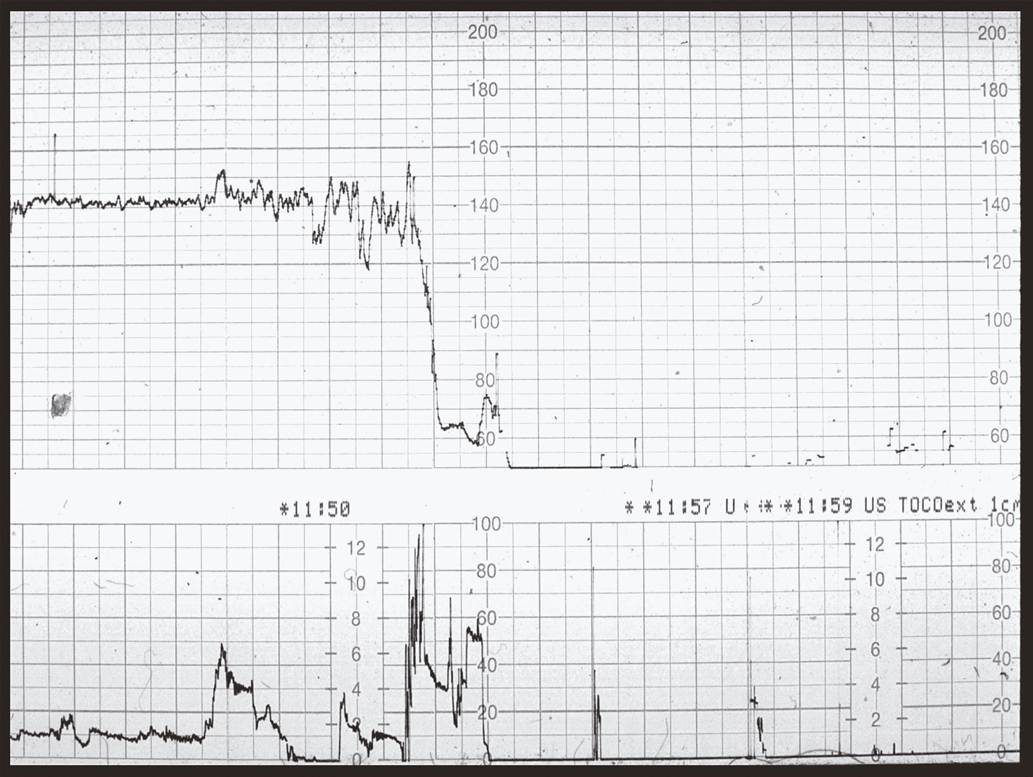
Figure 27.4 Prolonged deceleration less than 80 bpm for longer than 15 minutes.
withstand the stress of uterine contractions which can expose them to hypoxia in labour.
The LAT was originally designed as a preliminary assessment of women with low-risk pregnancies at the onset of labour so that those with non-r eassuring FHR patterns could be subjected to additional tests of fetal surveillance or delivered depending on the severity of fetal jeopardy. It often meant that women with an abnormal LAT were classified as high risk and then monitored with continuous CTG throughout labour. Thus, the LAT could be utilized as a screening tool in early labour to detect compromised fetuses on admission and select the women who may benefit from continuous CTG during labour.
The LAT can be performed by auscultation only or using CTG. The admission CTG comprises of a CTG trace of 20-30 minutes’ duration carried out on admission to the maternity ward. Most admission tests last 15- 30 minutes. However a normal trace that shows two accelerations and no decelerations with two contractions within 5 to 10 minutes should not be monitored unduly. If the test is attempted when the fetus is in quiescent/sleep phase, it will need to be continued until the fetus reawakens and a reassuring FHR pattern emerges. Although the existing RCTs and systematic reviews do not favour admission testing, the methodology used in some of these major studies is open to criticism. There is a need for robust RCTs with adequate sample sizes to evaluate the effectiveness of the LAT. NICE guidelines do not recommend performing CTG on admission for low-risk women in suspected or established labour in any birth setting as part of the initial assessment (11).
Intermittent and continuous intrapartum EFM
The NICE guideline recommends continuous CTG in labour if any of the risk factors are identified on initial assessment, and it must be explained to the woman why this is necessary (11). These risk factors may be:
• suspected chorioamnionitis or sepsis, or a temperature of 38°C or higher
• severe hypertension (≥160∕110 mmHg)
• oxytocin use
• presence of significant meconium
• fresh vaginal bleeding in labour.
Continuous CTG is also recommended if two or more of the following risk factors are present:

• Prolonged period since rupture of membranes (≥24 hours).
• Moderate hypertension (150/100 to 159/109 mmHg).
• Confirmed delay in the first or second stage of labour.
• Presence of non-significant meconium.
CTG is also recommended if one of the above-listed factors is present with any of the following:
• Maternal pulse over 120 bpm on two occasions 30 minutes apart.
• A single reading of either raised diastolic blood pressure of 110 mmHg or more, or raised systolic blood pressure of160 mmHg or more.
• Either raised diastolic blood pressure of 90 mmHg or more, or raised systolic blood pressure of 140 mmHg or more, on two consecutive readings taken 30 minutes apart.
• A reading of 2+ of protein on urinalysis and a single reading of either raised diastolic blood pressure (≥90 mmHg) or raised systolic blood pressure (≥140 mmHg).
• Temperature of 38°C or higher on a single reading, or 37.5°C or higher on two consecutive occasions 1 hour apart.
• Any vaginal blood loss other than a show.
• The presence of significant meconium.
• Pain reported by the woman that differs from the pain normally associated with contractions.
• Confirmed delay in the first or second stage of labour.
• Request by the woman for additional pain relief using regional analgesia.
• Obstetric emergency—including antepartum haemorrhage, cord prolapse, maternal seizure, or collapse.
If continuous CTG is needed, it should be explained to the woman that it will restrict her mobility, particularly if conventional monitoring is used. The woman should be encouraged to be as mobile as possible and to change position as often as she wishes. It should be borne in mind that it is not possible to categorize or interpret every CTG trace; senior obstetric input is important in these cases (11).
CTG is also recommended if intermittent auscultation indicates possible FHR abnormalities. The CTG can be discontinued if the trace is normal after 20 minutes.
Whenever CTG is used as a form of fetal monitoring at the beginning of labour, the woman should be offered an explanation that a normal trace is reassuring and indicates that the baby is coping well with labour, but if the trace is not normal there is less certainty about the condition of the baby and further continuous monitoring will be advised.
Systematic CTG interpretation
A crucial advantage of the CTG is the ability to assess all parameters of FHR including baseline variability. Presence of accelerations, normal baseline heart rate, variability greater than 5-25 bpm, and absence of any decelerations are features of a normal reassuring CTG (Figure 27.1). With a normal baseline CTG, a gradually developing hypoxia will be reflected by no accelerations, repeated decelerations, and gradually rising baseline rate (Figure 27.5). Furthermore, it is known that if a well-grown fetus with clear amniotic fluid and a reactive CTG trace starts to develop an abnormal FHR pattern, it takes some time with these FHR changes before acidosis develops. A study estimated that in situations with abnormal FHR pattern, for 50% of the babies to become acidotic, it took 115 minutes with repeated late decelerations, 145 minutes with repeated variable decelerations, and 185 minutes with a flat trace (18). Fetuses with a reactive admission CTG will show the following features prior to or becoming hypoxic—all will exhibit decelerations (100%), and almost all will have reduced baseline variability (93%) and baseline tachycardia (93%) (19) (Figure 27.5). A rising baseline associated with reduced variability therefore may be an ominous sign of fetal hypoxia where the fetus tries to increase oxygen delivery to vital organs by increasing cardiac output. On the other hand, if the baseline CTG is non-reactive, the development of further abnormal features with progress of labour are variable and subtle; this is difficult to recognize by intermittent auscultation (20) (Figure 27.6). This is because there might be pre-existing hypoxic damage and the fetus is unable to respond. Such a fetus may not withstand the stress of uterine contractions and runs the risk of death within a few hours of admission (Figure 27.7).
When interpreting a CTG trace, it is important to follow a systematic approach (Box 27.1) (21). The use of vague descriptors such as ‘sleepy trace', ‘bad CTG', or ‘fetal distress' should be avoided. The NICE evidence-based clinical guideline (11) (Tables 27.1 and 27.2) promotes a systematic approach to CTG interpretation, with individual features classified as reassuring, non-reassuring, or abnormal and the overall CTG as normal/non-r eassuring and abnormal. Continuous EFM should be systematically assessed at least once an hour in labour and more often if indicated.
Management of non-reassuring or abnormal intrapartum CTG
In general, a ‘non-reassuring CTG' can be managed conservatively. An ‘abnormal CTG' requires institution ofconservative measures and fetal scalp blood sampling (FBS) where appropriate/feasible, otherwise delivery should be expedited. Interventions for non-reassuring or abnormal trace will depend on the suspected underlying cause for the abnormalities in FHR and the clinical situation. These features may be reversed by conservative measures such as changing maternal position, treating hypotension or pyrexia, hydration, reducing or stopping oxytocin, or tocolysis for hyperstimulation.
When the baseline FHR is greater than 180 bpm with no other non-reassuring or abnormal features on the CTG, possible underlying causes (such as infection) should be sought. The woman's temperature and pulse should be checked and if either is raised, fluids and paracetamol should be offered. FBS to measure lactate or pH should be considered if the rate stays higher than 180 bpm despite conservative measures.
Baseline variability will usually be 5-25 bpm. Intermittent periods of reduced baseline variability are normal, especially during periods of quiescence (‘sleep'). Mild or minor pseudo-sinusoidal patterns (oscillations of amplitude 5-15 bpm) are also of no significance especially if it is short lasting and the trace preceding or followed by is a reactive trace.
Timely action is crucial in cases of prolonged decelerations or bradycardia (Figure 27.5) for longer than 3 minutes where urgent intervention may be required. Possible causes include abruption, cord prolapse, and scar rupture. In the event of such a catastrophic ‘accident', immediate delivery should occur. In the absence of these, the ‘3-, 6,- 9-, 12-, 15- minute' guidance can be followed. Interventions such as cessation of oxytocin and treatment of maternal hypotension
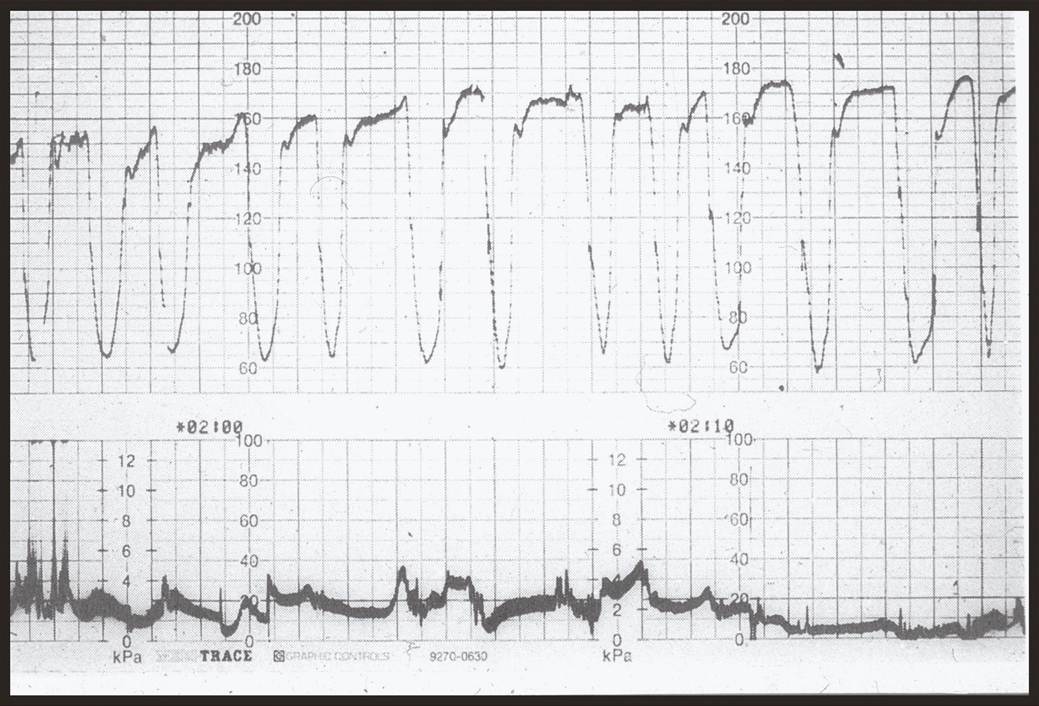
Figure 27.5 Tachycardia (rise from 140 to 170 bpm over 5 hours), absent baseline variability, and variable/late decelerations.
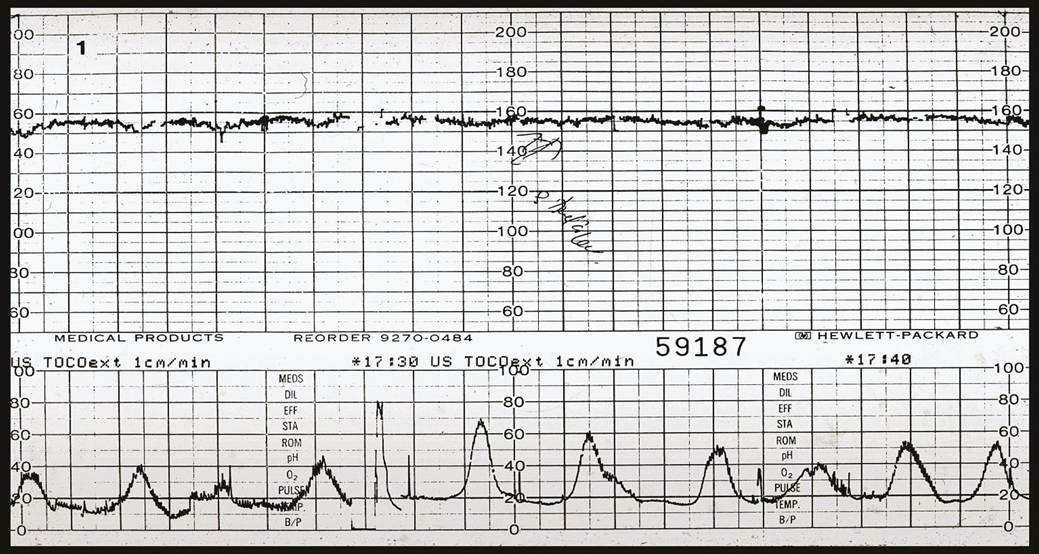
Figure 27.6 CTG trace from the time of admission showing reduced baseline variability, absent accelerations, and shallow late decelerations suggestive of ongoing/pre-existing hypoxia. The clinical history is likely to have thick meconium, reduced fetal movements, intrauterine growth restriction, infection, prolonged pregnancy or bleeding.
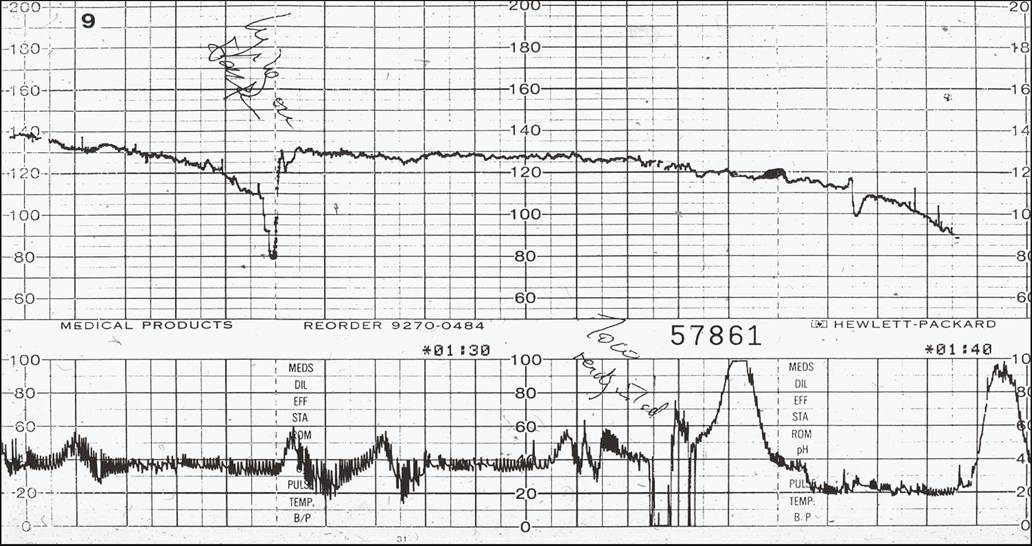
Figure 27.7 The fetal heart rate showing sudden bradycardia and collapse without showing obvious decelerations or rise in the baseline rate.
should commence. If there are no signs of recovery at 6 minutes, preparations should be made to transfer to theatre by 9 minutes. Caesarean section should commence by 12 minutes with the aim of delivery by 15 minutes. If instrumental delivery is possible this should be achieved within 15-20 minutes but a difficult instrumental delivery should be avoided. An experienced neonatal team should attend the delivery if resuscitation is anticipated. Many cases will recover by 9 minutes (especially if they had a normal CTG prior to this event) and caesarean section may not be necessary unless there are additional reasons for concern. If the FHR recovers at any time up to 9 minutes, the decision to expedite the birth should be reassessed, in discussion with the woman. Appropriate debriefing and explanation of events to the mother and partner should follow expedited delivery.
Some of the CTG patterns pose a challenge to the obstetrician regarding their interpretation and management. The following features in isolation are unlikely to be associated with significant acidosis (22): (a) moderate bradycardia (100-109 bpm), (b) moderate uncomplicated tachycardia (161-180) with accelerations present, (c) absence of accelerations, and (d) variable decelerations without complicating features.
Some of the important issues which need to be considered while recording or evaluating a CTG trace include:
• patient identity
• maternal pulse
• quality of the trace
• storage of CTG
• misinterpretation of CTG
• education and training in CTG interpretation
• teamwork and communication of findings
• action with non-reassuring or abnormal CTG
• overall clinical picture and pattern evolution of CTG
• role of infection and inflammation
• documentation of events and risk management.
At all times, it should be ensured that the focus of care remains on the woman rather than the CTG trace and no decisions about a woman’s care in labour should be made on the basis of CTG findings alone.
Fetal scalp blood sampling
CTG is an imperfect tool and many of the indicators used to identify early hypoxia are non-specific. Thus, if CTG is used as the sole method of intrapartum fetal surveillance, unnecessary operative deliveries will be performed. FBS for pH analysis and lactate measurement is used to assess fetuses with pathological FHR patterns. FBS is recommended with pathological CTGs to identify those fetuses that require delivery and ideally all maternity units where CTG is used should have ready access, 24 hours a day, to an accurate blood gas analyser. To obtain a fetal scalp capillary sample, the cervix has to be at least 3-4 cm dilated. With the mother in the left lateral position, an amnioscope is introduced into the vagina and kept against the fetal scalp to exclude amniotic fluid entering the sera of sampling and the scalp is cleaned dry. Hyperaemia is induced with ethyl chloride spray and a small sample (approximately 35 μL) is obtained in a capillary tube after making a stab incision. Once FBS has been done, pressure with a swab to the site of the puncture should stop the bleeding. Automated blood gas analysis is performed and management depends on the clinical situation as well as the absolute values of the scalp pH and base excess. In some labours, pH sampling may be required more than once. The test requires technical skill and
Box 27.1 Systematic interpretation of CTG trace
• Determine risk
• Contraction frequency and duration
• Baseline rate
• Accelerations
• Variability
• Decelerations
• Overall impression and care plan
access to a calibrated blood gas analyser, is difficult to perform at cervical dilatations less than 4 cm, and can be stressful/uncomfort- able for the mother. There is failure to obtain a result in 11-20% of cases (22). The median time from decision to undertake FBS to obtaining a result has been shown to be 18 minutes and in 9% of cases takes longer than 30 minutes (22). Contraindications to FBS or invasive fetal monitoring are maternal infections such as HIV, hepatitis B and C, active herpes simplex, fetal bleeding disorders, haemophilia (male fetus in carrier), and preterm gestation less than 34 weeks. Table 27.3 summarizes the normal and abnormal acidbase values.
NICE advises that after an abnormal FBS result, consultant obstetric advice should be sought.
After a normal FBS result, sampling should be repeated no more than 1 hour later if the FHR trace remains pathological, or sooner if there are further abnormalities. After a borderline FBS result, sampling should be repeated no more than 30 minutes later if the FHR trace remains pathological or sooner if there are further abnormalities. Further abnormalities are identified by the features of increasing depth and duration of decelerations, reduction of the inter deceleration intervals, rise in the baseline rate, and reduction in the baseline variability. The time taken to take a fetal blood sample needs to be considered when planning repeat samples. If the FHR trace remains unchanged and the FBS result is stable after the second test, a third/further sample may be deferred unless additional abnormalities develop on the trace. Where a third FBS is considered necessary or sampling fails, a consultant obstetric opinion should be sought as based on the clinical situation delivery may be more appropriate.
The clinical context of the labour should always be considered including parity, progress, stage of labour, and maternal wishes. It should be remembered that fetal infection or thick meconium associated with a pathological CTG may result in an adverse neonatal
Table 27.1 Description of Cardiotocograph trace features
| Accelerations • The presence of fetal heart rate accelerations is generally a sign that the unborn baby is healthy • If a fetal blood sample is indicated and the sample cannot be obtained, but the associated scalp stimulation results in fetal heart rate accelerations, decide whether to continue the labour or expedite the birth in light of the clinical circumstances and in discussion with the woman | |||
| Description | Feature | ||
| Baseline (beats/minute) | Baseline variability (beats/minute) | Decelerations | |
| Normal/reassuring | 100-160 | 5 or more | None or early |
| Non-reassuring | 161-180 | Less than 5 for 30-90 minutes | Variable decelerations: • dropping from baseline by 60 beats/minute or less and taking 60 seconds or less to recover • present for over 90 minutes • occurring with over 50% of contractions Or Variable decelerations: • dropping from baseline by more than 60 beats/minute or taking over 60 seconds to recover • present for up to 30 minutes • occurring with over 50% of contractions Or Late decelerations: • present for up to 30 minutes • occurring with over 50% of contractions |
| Abnormal | Above 180 or below 100 | Less than 5 for over 90 minutes | Non-reassuring variable decelerations (see row above): • still observed 30 minutes after starting conservative measures • occurring with over 50% of contractions Or Late decelerations: • present for over 30 minutes • do not improve with conservative measures • occurring with over 50% of contractions Or Bradycardia or a single prolonged deceleration lasting 3 minutes or more |
National Institute for Health and Care Excellence (NICE). Intrapartum Care for Healthy Women and Babies. Clinical guideline [CG190]. London: NICE; 2014.
Table 27.2 Management based on interpretation of Cardiotocograph traces
| Category | I Definition | I Interpretation | Management |
| CTG is normal/reassuring | All 3 features are normal/ reassuring | Normal CTG, no non-reassuring or abnormal features, healthy fetus | • Continue CTG and normal care • I f CTG was started because of concerns arising from intermittent auscultation, remove CTG after 20 minutes if there are no nonreassuring or abnormal features and no ongoing risk factors |
| CTG is non-reassuring and suggests need for conservative measures | 1 non-reassuring feature and 2 normal/reassuring features | Combination of features that may be associated with increased risk of fetal acidosis; if accelerations are present, acidosis is unlikely | • Think about possible underlying causes • I f the baseline fetal heart rate is over 160 beats/minute, check the woman's temperature and pulse. If either are raised, offer fluids and paracetamol • Start 1 or more conservative measures: - encourage the woman to mobilize or adopt a left-lateral position, and in particular to avoid being supine - offer oral or intravenous fluids - reduce contraction frequency by stopping oxytocin if being used and/or offering tocolysis • Inform coordinating midwife and obstetrician |
| CTG is abnormal and indicates need for conservative measures and further testing | 1 abnormal feature or 2 non-reassuring features | Combination of features that is more likely to be associated with fetal acidosis | • Think about possible underlying causes • I f the baseline fetal heart rate is over 180 beats/minute, check the woman's temperature and pulse. If either are raised, offer fluids and paracetamol • Start 1 or more conservative measures (see 'CTG is nonreassuring...' row for details) • Inform coordinating midwife and obstetrician • Offer to take an FBS (for lactate or pH) after implementing conservative measures, or expedite birth if an FBS cannot be obtained and no accelerations are seen as a result of scalp stimulation • Take action sooner than 30 minutes if late decelerations are accompanied by tachycardia and/or reduced baseline variability • Inform the consultant obstetrician if any FBS result is abnormal • Discuss with the consultant obstetrician if an FBS cannot be obtained or a third FBS is thought to be needed |
| CTG is abnormal and indicates need for urgent intervention | Bradycardia or a single prolonged deceleration with baseline below 100 beats/minute, persisting for 3 minutes or morea | An abnormal feature that is very likely to be associated with current fetal acidosis or imminent rapid development of fetal acidosis | • Start 1 or more conservative measures (see 'CTG is nonreassuring...' row for details) • Inform coordinating midwife • Urgently seek obstetric help • Make preparations for urgent birth • Expedite birth if persists for 9 minutes • I f heart rate recovers before 9 minutes, reassess decision to expedite birth in discussion with the woman |
CTG, cardiotocography; FBS1 fetal blood sample.
a A stable baseline value of 90-99 beats/minute with normal baseline variability (having confirmed that this is not the maternal heart rate) may be a normal variation; obtain a senior obstetric opinion if uncertain.
National Institute for Health and Care Excellence (NICE). Intrapartum Care for Healthy Women and Babies. Clinical guideline [CG190]. London: NICE; 2014.
outcome even in the absence of fetal acidosis. A normal FBS result in these circumstances does not give the same reassurance.
If a FBS is indicated and the sample cannot be obtained, but the associated scalp stimulation results in FHR accelerations, the clinician should decide whether to continue the labour or expedite the birth considering the clinical circumstances and in discussion with
Table 27.3 The classification of fetal blood sampling results
| Lactate (mmol/L) | ∣ph I | Interpretation |
| ≤4.1 | ≥7.25 | Normal |
| 4.2-4.8 | 7.21-7.24 | Borderline |
| ≥4.9 | ≤7.20 | Abnormal |
These results should be interpreted taking into account the previous pH measurement, the rate of progress in labour and the clinical features of the woman and baby. National Institute for Health and Care Excellence (NICE). Intrapartum Care for Healthy Women and Babies. Clinical guideline [CG190]. London: NICE; 2014. the woman (11). This is because induced accelerations by stimulation are almost always associated with non-acidotic scalp pH values. If a FBS is indicated but a sample cannot be obtained and there is no improvement in the CTG trace, advise the woman that the birth should be expedited.
Fetal lactate measurement has been proposed as an alternative to scalp pH as the lactate levels reflect anaerobic respiration and thus tissue hypoxia and metabolic acidosis. The invasive procedure for sampling is similar to FBS but requires a smaller volume of blood (5 μL). Available data indicate that levels greater than 4.8 mmol/L are abnormal and require delivery and levels of 4.2-4.8 mmol/L should be regarded as borderline (22).
The Cochrane review in 2013 by Alfirevic et al. found no reduction in caesarean rates or neonatal seizures with access to scalp sampling in addition to EFM (13). A randomized Swedish study found that scalp pH and lactate were no different in diagnosing fetal acidosis compared with pH and base excess but lactate sampling had lower failure rates (1.2% vs 10.4%) (23).
Meconium-stained liquor
Meconium-stained liquor is defined as dark green or black amniotic fluid that is thick or tenacious, or any meconium-stained amniotic fluid containing lumps of meconium. Although passage of meconium may be a function of fetal maturity, it can also indicate possible fetal compromise. Use of prostaglandin and fetal infection are also associated with the passage of meconium. The incidence of meconium staining of the liquor increases from 36 to 42 weeks' gestation, reaching around 20-30% at full term. Although fetuses do not normally draw amniotic fluid into the airway, they gasp when hypoxic and therefore the coexistence of hypoxia and acidosis may precipitate meconium aspiration.
Since meconium passage may indicate acute or chronic hypoxia, continuous FHR monitoring is recommended in these cases to detect possible fetal compromise. Moderate and thick meconium have been linked to abnormal FHR traces and adverse neonatal outcomes. The commonest abnormal FHR features associated with adverse neonatal outcomes are prolonged decelerations, severe variable decelerations, bradycardia, and tachycardia. In the presence of meconium, the fetal scalp pH result may be a less reliable indicator of poor fetal condition than is fetal oximetry.
As part of ongoing assessment in labour, the presence or absence of significant meconium should be clearly documented. If significant meconium is detected, healthcare professionals trained in FBSs and advanced neonatal life support should be available during labour and delivery. The woman should be transferred to obstetric-led care provided that it is safe to do so and the birth is unlikely to occur before transfer is completed.
Fetal pulse oximetry
The critical fetal oxygen saturation above which the fetus does not demonstrate significant acidosis is 30%. This has led to the development of fetal pulse oximetry techniques to allow assessment of fetal oxygenation as a marker for fetal acidosis. An oximeter probe is passed transcervically and placed against the fetal scalp or side of the face. Deoxygenated and oxygenated haemoglobin absorb light at different wavelengths and by using standard curves the oximeter is able to determine the fetal oxygen saturation. The probe is connected to a standard FHR monitor and displays a continuous signal. Although a normal saturation supports fetal well-being, there is insufficient data available to support its routine clinical use. Several factors such as sensor-t o-skin contact, uterine contractions, fetal hair, and caput succedaneum may influence the performance and use of pulse oximetry.
A Cochrane review in 2014 which included published trials comparing fetal pulse oximetry and CTG with CTG alone (or when fetal pulse oximetry values were blinded), suggested that the available data provide limited support for the use of fetal pulse oximetry when used in the presence of a non-reassuring CTG, to reduce caesarean section for non-reassuring fetal status. The addition of fetal pulse oximetry did not reduce overall caesarean section rates (24).
Fetal acoustic stimulation
The ability of a fetus to respond to stimulation with an acceleration in FHR implies a well-oxygenated intact nervous system. Stimulation of the fetal head may be attempted by digital vaginal examination or the scalp laceration during FBS. A reassuring response of acceleration can indicate fetal well-being. The vibroacoustic stimulation test uses an artificial larynx placed closed to the maternal abdominal wall to startle and wake up the fetus. If accelerations are noted in the CTG following the test, a pH of less than 7.2 is unlikely.
A meta-analysis assessed the performance of stimulation tests for the prediction of intrapartum fetal acidaemia. Intrapartum stimulation tests appeared to be useful to rule out fetal acidaemia in the setting of a non-reassuring FHR pattern (25). A Cochrane review found insufficient evidence from randomized trials on which to base recommendations for its use in the presence of a non-reassuring CTG trace (26).
Fetal ECG waveform analysis
A growing number of centres are taking up the use of fetal ECG in combination with continuous EFM as an additional test of fetal well-being. Monitoring requires rupture of the membranes and application of a fetal scalp electrode and a maternal skin reference electrode. The fetal ECG is recorded continuously from a specialized scalp electrode and analysed by computer technology. Fetal hypoxia can act on the fetal myocardium and cause alterations to the ST segment of the fetal ECG. The drawback of the method is that the technology relies considerably on human interpretation of the CTG to indicate the appropriate action when ST-segment changes occur.
Various studies have assessed the effectiveness of fetal ECG with heart rate monitoring (27-30). The results showed a significant reduction in severe metabolic acidosis and neonatal encephalopathy. It was also associated with a significant decrease in obstetric interventions such as FBS and operative vaginal delivery. There was no significant difference in caesarean delivery rate. More recently, an RCT in Finland showed neither a significant improvement in neonatal outcome nor a reduction in caesarean section, although there was a reduction in the need for FBS (31). A Cochrane review found modest support for the use of fetal ST waveform analysis when a decision has been made to undertake continuous electronic FHR monitoring during labour (30).