Molar pregnancy
Incidence
Molar pregnancy incidence is decreasing worldwide. It is still more common in South-East Asia (2 per 1000 pregnancies) than Europe and North America (<1 per 1000 pregnancies).
A similar decrease was seen in Japan (1) which could be related to a decreasing number of childbirths and an improved economy. The use of ultrasonography early in pregnancy which may have led to early diagnosis and termination of non-viable pregnancies without histology assessment could also result in underestimation of the incidence of molar pregnancy. A decreasing incidence has also been observed in GTN in Korea and Japan (2). For choriocarcinoma, the incidence is difficult to estimate because it is uncommon to have a histological assessment of ‘tumour’ seen in GTN. The ‘tumour’ could be invasive or a metastatic mole or choriocarcinoma. Knowing this limitation, the incidence of choriocarcinoma has been reported to be approximately 1- 9 in 40,000 pregnancies, and again the incidence rates have been declining.Presentation
The most common presentation nowadays is abnormal bleeding complicating an early pregnancy and ultrasonographic examination helps to make an early diagnosis (3). Uterine size is variable in relationship to gestation. Hyperemesis gravidarum, hyperthyroidism, bleeding leading to severe anaemia, early-onset severe pre-eclampsia, uterine size larger than dates, bilateral large theca lutein cysts, and pulmonary trophoblastic embolism are rarely seen today as these symptoms and signs tend to be associated with advanced molar pregnancy.
Diagnostic investigations
Ultrasonography is the most useful diagnostic investigation for molar pregnancy. However, the typical snow-s torm appearance (Figure 66.1) is less commonly seen because of early presentation. Ultrasound features of early molar pregnancy are less typical. It could be an absence of fetal parts, a cystic appearance of the placenta, and a deformed gestational sac similar to a missed miscarriage.
In fact, one study showed that the typical sonographic appearance of a first- trimester complete mole is a complex, echogenic, intrauterine mass with many small cystic spaces (Figure 66.2) (4). Moreover, 21% and 71% of complete and partial hydatidiform moles respectively could be missed on ultrasonography, especially in early gestational age (5). Hence, histological examination of all gestational products will pick up early molar pregnancy missed by ultrasound examination.Pathology and cytogenetics
The typical histopathology of molar pregnancy includes hydropic villi and trophoblastic proliferation. The main challenge lies in differentiating between complete mole from partial mole and partial mole from hydropic degeneration of villi in miscarriages (6). Histologically, complete mole has florid cistern formation, trophoblastic proliferation, and an absence of fetal parts (Figure 66.3). In partial mole, there is less proliferation and fetal parts or fetal blood cells are present (Figure 66.4). Hydropic miscarriage looks very similar to partial mole. Early complete moles may lack florid histological features but have structures such as abnormal budding villous with trophoblast hyperplasia, stromal karyorrhectic debris, and collapsed villous blood vessels. On the other hand, patchy villous hydrops with scattered abnormally shaped irregular villi, trophoblastic pseudoinclusions, and patchy trophoblast hyperplasia are seen in partial moles (7). With the help of a cytomolecular study to identify the origin of the sex chromosomes, an androgenetic diploid complete mole (Figures 66.5 and 66.6) (41) or a biparental triploid partial mole can be differentiated from a diploid miscarriage. Using

Figure 66.1 Ultrasound image of a molar pregnancy showing a complex echogenic mass containing multiple discrete cystic spaces (snow-storm appearance) in the uterine cavity.
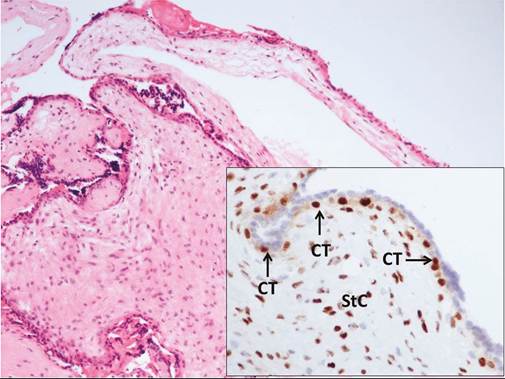
Figure 66.4 Photomicrographs demonstrating partial hydatidiform mole: cytotrophoblasts (CT) and stromal cells (StC) are positive for p57KIP2, encoded by CDKN1C, a paternally imprinted gene which is maternally expressed.
Courtesy of Cheung AN, Department of Pathology, The University of Hong Kong.

Figure 66.2 Ultrasound image of an early molar pregnancy showing echogenic tissue with numerous cystic vesicles in the uterine cavity.
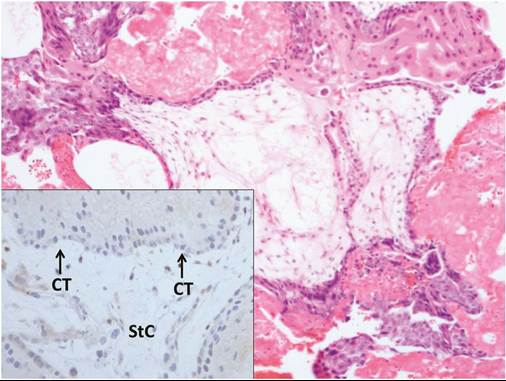
Figure 66.3 Photomicrographs demonstrating complete hydatidiform mole: cytotrophoblasts (CT) and stromal cells (StC) are negative for p57KIP2, encoded by CDKN1C, a paternally imprinted gene which is maternally expressed.
Courtesy of Cheung AN, Department of Pathology, The University of Hong Kong.
immunohistochemical staining of p57KIP2 (cyclin-dependent kinase inhibitor 1C, encoded by CDKN1C) to confirm the presence of maternal genes can exclude complete mole. However, if molar pregnancy still cannot be excluded, it is acceptable to monitor the serum hCG level for at least 6 months or until it becomes normal.
Management of molar pregnancy
The standard treatment is suction evacuation of the uterus. It should be performed by an experienced anaesthetist and gynaecologist because of the risk of bleeding, respiratory complication, and perforation of uterus. To prepare for the heavy bleeding during suction evacuation, it is essential to have venous access with a wide- bore cannula and crossmatched blood readily available. Oxytocics can be used after cervical os dilation and onset of suction curettage with no increase in risk of GTN. As the uterus tends to be soft, the use of intraoperative ultrasound or evacuation by an experienced gynaecologist may reduce the risk of uterine perforation.
However, a routine second evacuation is not recommended unless there is a clinical indication such as persistent vaginal bleeding. Termination of pregnancy using medical methods should be avoided except in second-trimester termination of a partial mole with a fetus since it increases the chance of developing GTN (8). Hysterectomy is not indicated for termination of molar pregnancy but can be performed if there is a coexisting indication or life-threatening haemorrhage.Human chorionic gonadotropin monitoring
Serial serum hCG monitoring following evacuation is essential for early diagnosis of GTN. After evacuation, weekly or biweekly hCG monitoring is performed until the level returns to normal and then it is spaced out to 4 weeks for 6 months. The criteria for a diagnosis of GTN will be discussed later (see ‘Diagnosis’). The risk of developing GTN is 0.5-1% after partial mole and 15-20% after complete mole.
Serum hCG assay
The accuracy of serum hCG measurement in monitoring of GTN is affected by the choice of assay method (9). In addition to intact hCG,
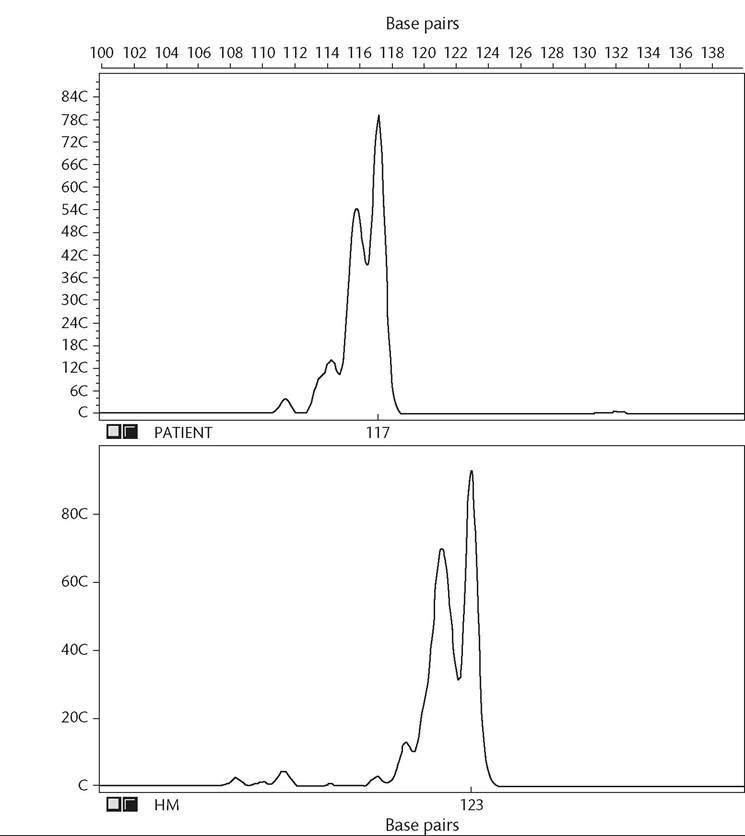
Figure 66.5 Microsatellite genotyping of a diploid complete hydatidiform mole: microsatellite polymorphisms of a patient and the diploid hydatidiform mole (HM). The patient was homozygous for the marker D17S1322, generating an allele of 117 base pairs. The HM also was homozygous for D17S1322, giving rise to an allele of 123 base pairs, which was not found in the maternal DNA and thus was androgenetic.
Reproduced from Cheung AN, Khoo US, Lai CY, Chan KY, Xue WC, Cheng DK et al. Metastatic trophoblastic disease after an initial diagnosis of partial hydatidiform mole: genotyping and chromosome in situ hybridization analysis. Cancer 2004;100:1411-17.
patients with GTN also produce nicked hCG, hyperglycosylated hCG, hCG with missing beta- subunit C- terminal segment, and hCG with free beta subunit. Thus, commercially available pregnancy test kits which often measure only total hCG are not suitable and may lead to false-negative results thus either missing the diagnosis or leading to inadequate treatment.
False-positive serum hCG
False-positive serum hCG is due to the presence of heterophilic antibodies in sera. This can explain the ‘phantom hCG' when serum hCG levels are persistently raised in the absence of GTN (10). It could be differentiated by a negative urine hCG assay or by a serial dilution assay where the levels do not follow the dilution factor.
Central registry
Ideally, all women with a molar pregnancy should be registered with a central registry to facilitate central hCG assay, monitoring, and management. Especially in countries with decreasing incidence, pooling of expertise and resources would ensure better quality of patient care. Early diagnosis and proper management of postmolar GTN has a high cure rate.
Contraception after molar pregnancy
A reliable contraceptive method is advised to allow monitoring of serum hCG after a molar pregnancy without the interference of a normal pregnancy. The combined oral contraceptive pill can be used immediately after termination of a molar pregnancy (11) or after hCG has returned to normal (12). Termination of pregnancy is not indicated if pregnancy occurs during surveillance after the hCG has declined to normal levels.
Recurrent molar pregnancy
The risk of having another molar pregnancy after a complete mole is around 1% but women with two complete moles have
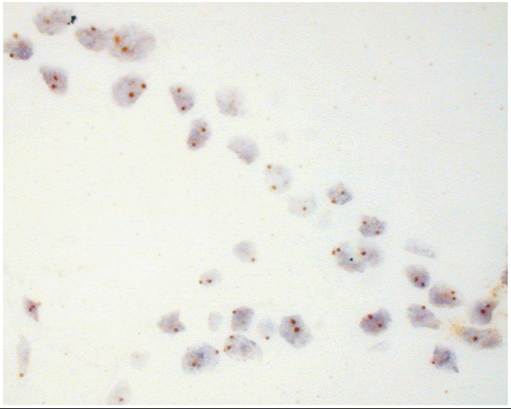
Figure 66.6 Chromosome/ n situ hybridization of a diploid complete hydatidiform mole: two hybridization signals, as detected by DNA probes for chromosome 16, were found in the majority of nuclei.
Reproduced from Cheung AN, Khoo US, Lai CY, Chan KY, Xue WC, Cheng DK et al. Metastatic trophoblastic disease after an initial diagnosis of partial hydatidiform mole: genotyping and chromosome in situ hybridization analysis. Cancer 2004;100:1411-17.
a one in four risk of another mole (13) and have a higher risk of persistent GTN (14). The risk of further molar pregnancies in women with a partial mole was only slightly increased (1 in 350). Women should be reassured that the majority of women have a normal pregnancy and delivery following a molar pregnancy. A small proportion has ‘familial recurrent hydatidiform moles’, which is a rare autosomal recessive disorder caused by mutations in the NLRP7 (NLR family, pyrin domain containing 7) and the KHDC3L (KH domain containing 3-like, subcortical maternal complex member) genes.
Mole with coexisting normal twin
Rarely, molar pregnancy is found on ultrasonography together with a normal twin pregnancy. Although the risk of spontaneous miscarriage is high, about 40% achieve live births. There is no increase in the risk of developing GTN (15). Thus, pregnancy need not be terminated after confirming normal karyotype and an otherwise normal pregnancy.