Neonatal Care Aspects of Multiple Pregnancy
Alejandra Barrero-Castillero and DeWayne M. Pursley
The Issues
Few clinical events are more challenging than the resuscitation and stabilisation of a critically ill patient.
In paediatrics, the management of multiple-gestation newborns can present an even more formidable task. While the majority of these infants will only require routine nursery care, because of their greater prevalence of high-risk conditions, the likelihood of emergent care is higher in multiple births. This is owing to higher rates of complications during pregnancy, delivery and the neonatal period. Sound preparation is essential, as is the need for the nursery staff to quickly identify these conditions and provide effective neonatal management. Multiple-pregnancy newborns make up only 3.5% of all live births but account for up to 15% of neonatal intensive care unit (NICU) admissions.1,2Adverse Outcomes (Compared to Singletons)
Multiple pregnancies have an increased risk of adverse outcomes, including intrauterine growth restriction, preterm delivery (PTD), preterm and premature rupture of membranes (PPROM) and congenital anomalies, compared to singleton pregnancies. All have potential clinical implications for the multiple infant.
Perinatal Morbidity and Mortality
Morbidity
A study evaluating a comprehensive financial and health services evaluation of multiplepregnancy and higher-order multiples in 2014 found that multiple-pregnancy infants consume significantly more health resources during the newborn period and the first year of life.3 Even though multiple-gestation newborns are statistically at a higher risk for morbidity, this association is highly confounded by the associated adverse factors.
In general, multiple-pregnancy newborns, especially twins, do well, experience little morbidity and develop normally. Because of the association between morbidity and longterm development, this relationship is important to examine.
Newborns born from multiple pregnancy may experience serious complications associated with prematurity, including respiratory distress syndrome, that may progress to chronic lung disease, apnoea, hypoglycaemia, intraventricular and intra-parenchymal haemorrhage, periventricular leukomala- cia, asphyxia and other complications that can result in long-term developmental problems. These are described in more detail later in this chapter.Mortality
Most complications and adverse outcomes of multiple-pregnancy newborns are associated with gestational age and birthweight, the most important predictors of infant mortality. Overall mortality in premature infants has declined due to developments in neonatal and obstetric care, including the use of antenatal glucocorticoids, exogenous surfactant and improved ventilatory care.
In 2017 almost three-quarters of all infant deaths in the United States occurred in preterm infants, with the highest rates experienced by extremely premature infants born at 28 weeks or less (183 times the rate for term infants).4 Among higher-order multiple births, the increased risk of infant mortality appears to be largely due to the lower birthweight distribution and shorter gestation among these infants. When matched for gestational age, race, gender and mode of delivery, preterm twins appear to have similar outcomes to singleton infants. On the other hand, monochorionic and monoamniotic twins have higher risk for both morbidity and mortality compared to dichorionic twins. Death of both twins is higher with gestation associated with monochorionic placentation.5
Prematurity
Prematurity (birth before 37 weeks of gestation) is one of the leading causes of morbidity and mortality in children younger than five years worldwide. It is well known that multiple pregnancies are associated with a higher risk of preterm delivery compared to singleton pregnancies. The pathogenesis of premature delivery remains unclear, and it is difficult to predict which multiple pregnancies will result in preterm birth.6 Some suggest that uterine over-distension, mechanical stretching of the cervix and decreased uterine blood flow - consistent with the observation that the number of fetuses present is inversely proportional to the gestational age at birth - may explain the increased risk of prematurity in multiples.
In the United States in 2018, when preterm births accounted for 10% of all live births, twins were almost eight times more likely to be born preterm than singletons: 60.3% compared with 8.2%. The incidence of preterm birth increases with plurality. Of all live births in the United States in 2018, 96.6% were singletons and 3.4% were multiple births. In 2005 the mean gestational age for twin delivery was 35.2 weeks, and for triplet delivery it was 31.9 weeks, for quadruplet delivery it was 29.8, and for quintuplet delivery and higher it was 27.4 weeks compared to 38.7 weeks for singletons.7
Complications in premature infants after birth are mainly due to difficulties in extra- uterine life adaptation as well as to a spectrum of multiple organ immaturity that is inversely proportional to gestational age at birth. Thanks to advanced intensive care, even infants who are born very prematurely are more likely to survive today than some years ago. Figure 26.1 describes the classification of prematurity by gestational age and birthweight and the most common and expected complications after birth. It is important to note that incidence and severity of complications decrease as gestational age increases.
Abnormal Fetal Growth (Intrauterine Growth Restriction and Discordant Growth)
We use several terms that describe the overall weight at birth independent of gestational age (low birthweight, very low birthweight and extremely low birthweight), and we use others to describe weight by gestational age, which include small for gestational age (SGA) (weight at < 10th
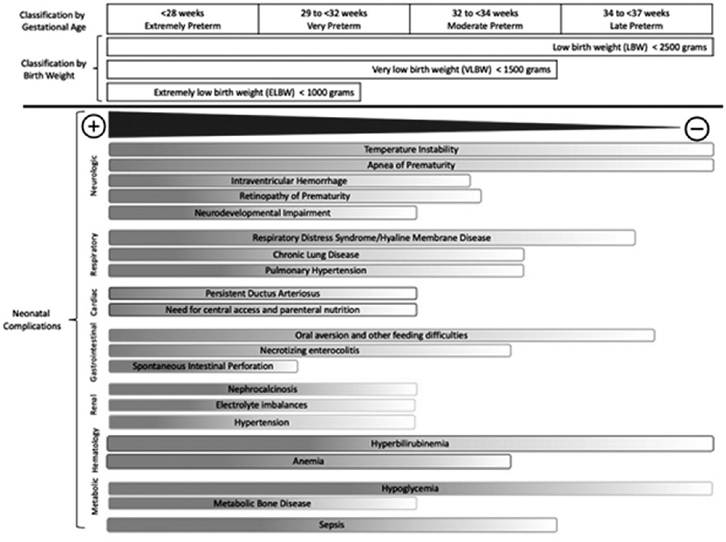
Figure 26.1 Neonatalcomplications broadly associated with gestationalage and birthweight ranges
percentile for gestational age), large for gestational age (LGA) (weight at > 90th percentile for gestational age) and appropriate for gestational age (AGA). Additionally, we use either fetal growth restriction (FGR) or intrauterine growth restriction (IUGR) to describe delayed growth in utero.
While many SGA infants have evidence of IUGR and many IUGR infants are SGA, they are not exclusive.The weight at birth of multiple-pregnancy infants is less than the weight of singletons, in part due to shorter gestational age at birth. The birthweight of multiples is comparable to singletons up to 30-34 weeks of gestation, at which point multiples begin to have delayed growth. This growth restriction in twins and higher-order multiples may be explained by limited placental growth due to overcrowding, relative utero-placental insufficiency with inadequate nutrition consumption and insufficient blood flow to support the rate of growth seen in singletons.
Discordant growth in multiples is generally indicative of growth restriction in one of the fetuses and is defined as a difference in weight of more than 15%, 20% or 25% between fetuses, depending on the classification used. Individual IUGR is when one of the fetuses' weight falls below the 10th percentile of weight for gestational age. Growth restriction in both twins may reflect utero-placental dysfunction while discordant growth may be due to several factors like selective placental dysfunction (only in one placenta), genetics or an unequal vasculature share in a monochorionic placenta.8 A growth discordance of more than 30% has been associated with higher mortality in the smaller twin and higher morbidity in both twins.9
Congenital Anomalies and Early Malformations
Congenital anomalies are more likely to occur in multiple-pregnancy infants than in singletons. This increased rate is largely associated with monozygotic twins. These defects can develop early in gestation due to abnormal placental vascular anastomoses (discussed later in this chapter), or late in gestation due to constraints in the physical environment. The anomalies developed early in gestation may be incompatible with life and account for the overrepresentation of monozygotic twins among spontaneous abortions. Severe structural defects in monozygotic twins include acardia or hemicardia, anencephaly, holoprosencephaly malformation sequence, sacrococcygeal teratoma, exstrophy of the cloaca malformation sequence, VACTERL association, caudal regression syndrome (including sirenomelia) and conjoined twins.
Most of these cases are present in one twin but occur in both in 5-20% of cases. Even in cases where both infants have the defect, one may be less affected than the other. Finally, due to environmental constraints and uterine crowding, some twins may present with deformations like positional plagiocephaly, bowing of the limbs or clubfeet, developing later in gestation.6,10Conjoined Twins
Conjoined twins (see Chapter 10) are a rare event and represent an infrequent complication of monozygotic twinning. Two theories explain conjoined twins. The first one is ‘fission theory', where it occurs around day 13 to 15 after fertilisation when the embryonic discs (monozygotic twins) fail to separate. A second theory, called ‘fusion theory', describes two separated embryonic discs that fuse in areas where ectoderm is absent.11 Most commonly these twins are joined at the thorax, but they can be joined at the head, buttocks and other sites. Partial or complete duplication of only the upper or lower body parts may also take place. There is a 10-20% occurrence of major defects in addition to the defect related to the site of juncture, and this condition is more common in females than in males (3:1).11,12
Adverse Events due to Placental Vascular Anastomoses
Placentation is a major determinant of mortality in twins, with monochorionic twins experiencing greater morbidity and mortality than dichorionic-monozygotic or dizygotic twins. Vascular interconnections occur in almost all monochorionic twins and rarely in dichorionic multiples.6 Vascular connections between the two fetal circulations can be artery-to-vein shunts (twin-twin transfusion syndrome and twin anaemia-polycythaemia sequence), which are more common, and artery-to-artery shunts, which can range from no clinical significance to very severe disorders such as twin-reversed arterial perfusion (TRAP) sequence.
Twin-Twin Transfusion Syndrome and Twin Anaemia-Polycythaemia Sequence: Artery-to-Vein Anastomoses
Occurring in monochorionic twinning, artery-to-vein anastomoses are the basis of twintwin transfusion syndrome (TTTS) in which blood vessels connect within the placenta and divert blood from one fetus to the other.
During pregnancy, anastomoses are common and usually go through a placental cotyledon. Their size, number and direction, as well as the period of time over which the transfusion occurs, determine their consequences. Twin-twin transfusion syndrome has a spectrum of possible clinical outcomes and happens in about 15% of twins with a shared placenta. Clinically, the vascular shunt with many or large anastomoses will appear as hypovolemia, anaemia and paleness at birth in the ‘donor’ twin and hypervolemia, polycythaemia and plethora in the ‘recipient’ twin. An inter-pair difference in haemoglobin may be more than 5 grams/100 ml, and there may be discordant amniotic fluid volumes (polyhydramnios and oligo- or anhydramnios) and birthweight differences of more than 1,000 grams.6Over time, the cardiovascular system of the recipient fetus may become overloaded from chronic transfusion, and increased urine output may result in polyhydramnios. These infants are usually larger and they may develop polycythaemia (which may lead to jaundice or thrombosis postnatally), hypervolemia and cardiac hypertrophy. The volume overload may result in cardiac dysfunction that may progress to anasarca and hydrops. In the meantime, the donor fetus may develop a severely low blood volume, decreased urine output and oligo- or anhydramnios. These infants tend to be smaller (severe growth restriction) and may develop anaemia, hypovolemia that may progress to renal insufficiency, decreased organ mass and amnion nodosum (impacted vernix). While there are therapies to treat TTTS during pregnancy (discussed in previous chapters), these twins often must be delivered early to avoid stillbirth.
Management in the delivery room and after birth depends on the clinical presentation. The recipient twin with polycythaemia may have severe hyperviscosity syndrome that may require partial exchange transfusion. The donor twin may present with hypotension or poor perfusion due to chronic hypovolemia that may require immediate volume expansion and, at times, red blood cell transfusion. Both infants may present with severe respiratory distress, cyanosis, poor feeding, hypoglycaemia, jitteriness, lethargy, hypotonia and seizures. Later they are at risk for hyperbilirubinemia.
In some cases there is a recently described atypical chronic and milder form of TTTS, called twin anaemia-polycythaemia sequence (TAPS) that may be spontaneous, or a result of laser therapy for TTTS, where the arterio-venous placental shunt is through very narrowcalibre vessels causing a very slow transfusion that only causes anaemia and polycythaemia in the donor and recipient, respectively. Management in the NICU may include transfusion for the donor twin and partial exchange transfusion for the recipient twin.13 Additionally, the donor twin may present with growth restriction and hypoglycaemia.
Vascular Disruption Sequence (Artery-to-Artery Shunts)
Artery-to-artery anastomoses between two fetal circulations are common and often have no major clinical significance. However, on some rare occasions these connections may cause acute problems during labour and delivery, causing exsanguination of the donor twin. If this shunt develops early in gestation, it may lead to severe hemodynamic shifts, chronically perfusing the lower part of the recipient twin’s body, resulting in deterioration of tissues and severe malformations. This vascular disruption is variable, but in extreme cases it may result in an acephalic, acardiac or amorphous twin. This disorder is called twin-reversed arterial perfusion (TRAP) sequence. While the recipient twin may present with acardia, the donor twin (called the pump twin) may present with a structurally normal heart but with an excessive cardiovascular load that may result in cardiac dysfunction and progress to hydrops with very high mortality.6 Given the risk for cardiac overload, if surviving, donor (pump) twins in TRAP sequence should be evaluated for congestive heart failure.
Cord Complications in Monoamniotic Twins
In addition to the baseline risk factors and potential complications of multiple-pregnancy newborns, monoamniotic twins have unique risk for severe complications that contribute to a higher risk of perinatal morbidity and mortality among all multiple-pregnancy newborns, including cord complications. Cord complications and accidents include rupture of a vasa previa, cord entanglement and cord prolapse.
Respiratory Distress and Perinatal Depression to the Non-presenting Twin
Non-presenting newborns are generally considered at higher risk for morbidity and mortality. In infants born via vaginal delivery respiratory distress syndrome and perinatal depression tend to occur less frequently in the first or presenting twin, who may receive the full benefits from labour (the presenting twin has a higher lecithin-sphingomyelin ratio in amniotic fluid and higher cord-blood cortisol compared to the non-presenting twin after labour). This effect is particularly seen in premature infants who are at higher risk of respiratory distress syndrome and perinatal depression at baseline.14 The effects of perinatal depression can be ameliorated with readily available team(s) present at delivery and neonatal intensive care.
Increased Risk for the Surviving Twin in the Presence of Fetal Demise
As noted previously, monochorionic twins are at increased risk of mortality. In some cases one of the fetuses will die, placing the surviving twin at higher risk of mortality and adverse outcomes after birth. Co-twin demise may result in a capacitance effect or disseminated intravascular coagulation from emboli of the demised twin entering the surviving twin's circulation. This may increase the risk of serious defects like porencephalic cyst, hydranen- cephaly, limb amputation, aplasia cutis, gastroschisis or intestinal atresia. This presentation has been associated with an increased risk of cerebral palsy.
Long-Term Outcomes
In addition to the increased risks of morbidity and mortality during the neonatal period, multiple-pregnancy newborns are at increased risk for long-term neurodevelopmental deficits and poor growth. These deficits, however, may be largely explained by the multitude of genetic, perinatal and neonatal morbidity and the associated medical and social risk factors that can affect multiples, not associated with plurality. For example, preterm delivery is associated with increased risk for short-term outcomes such as high-grade intraventricular haemorrhage and periventricular leukomalacia15 and long-term neurodevelopmental deficits. Further, congenital anomalies are more common in twins and some anomalies like congenital heart disease are independently associated with increased risk of neurodevelop- mental delays.
Long-term outcomes are difficult to evaluate, much less apply to a single infant or group of infants. Systematic reviews of long-term neurodevelopmental outcomes of multiples compared with singleton newborns have not reported conclusive findings. Most studies control for birthweight and gestational age, have poor or borderline power to detect differences, and fail to include additional variables that may contribute to neurodevelopmental delays.16 While overall the prevalence of cerebral palsy is low, some populationbased studies have shown an increased risk of developing cerebral palsy in twins compared to singletons. Prospective cohort studies, however, have not found a higher incidence of cerebral palsy or seizure disorders in twins.17
One exception has been seen in fetal demise of a twin and history of TTTS (with or without fetal demise) where there is a risk of long-term neurodevelopmental outcomes like cerebral palsy (cognitive and neuromotor disabilities) reported in the surviving twin. Intrauterine therapies (e.g. amnioreduction) are not consistently associated with improvements in long-term neurodevelopment.17 As with other outcomes, no studies have reported increased risk in autism among multiples when adjusted for prematurity and older parental age.
Though not specific for twins, in addition to the increased risk for neurodevelopmental delay, premature and very low birthweight babies have an increased risk of rehospitalisation in the first year of life compared to newborns with normal weight.18 These infants may also be at a greater risk for child abuse and neglect.
Recent studies have shown that the majority of adults who were born preterm are healthy and well with a slight but significant increased risk of developing chronic and metabolic disorders, as well as neuropsychological and behavioural problems earlier in life compared to adults who were born at term, but there is little evidence that this is an independent risk factor for former multiple-pregnancy infants.19
Management of Multiple-Pregnancy Newborns
Multiple-pregnancy deliveries should occur in hospitals with appropriate staff to provide the appropriate level of care and ensure optimal outcomes. Although potential complications can never be fully anticipated for any delivery, given the range of risks for multiples, it is essential that the staff are fully aware of and prepared to respond to potential concurrent clinical challenges. The delivery site must be capable of providing risk-appropriate care for known fetal or anticipated delivery complications, and this may require transfer to a higher level of perinatal care.
Antenatal Consultation
The anticipated birth of multiple-pregnancy newborns may result in questions and uncertainly about possible outcomes, type of delivery and complications that may develop during pregnancy, at the time of birth or in the neonatal period. Referral to a paediatric provider or neonatal intensive care team should be considered, depending on the potential need for specialised care. Antenatal consultation provides an opportunity to create a relationship between the parents and the neonatal clinicians, setting the groundwork for a therapeutic relationship and a shared decision-making approach to care before and after the delivery, as well as an opportunity to educate and support decisions like breastfeeding. The maternal medical record should be carefully reviewed by the neonatal care team prior to the consultation to provide appropriate care recommendations and initiate planning for
delivery room management and immediate neonatal care. Additionally, if there are significant conditions or congenital anomalies that will require early paediatric medical subspecialty or surgical specialty care consultation, referral should be directed to those specific disciplines for counselling, planning and follow-up care.
Delivery Room Management
Delivery room management is especially important for multiple-gestation newborns given their higher likelihood of preterm delivery and greater risk for perinatal depression. Appropriately trained personnel must be in attendance, and in complex cases preparation may benefit from a pre-delivery huddle of the multidisciplinary team. Problems must be anticipated and prevented if possible, not simply treated. In infants for whom NICU admission is likely, a NICU delivery room team is required for each newborn.
The immediate postnatal goals are the same for multiples as for singletons, including resuscitation and stabilisation. Interventions in the delivery room will depend on gestational age at birth and clinical presentations. Resuscitation principles, as outlined in the Neonatal Resuscitation Program, include establishing an airway to support adequate oxygenation and ventilation, ensuring an effective cardiac output and maintaining appropriate temperature through drying and providing radiant heat. When respiratory support is necessary, a pulse oximeter and, at times, a cardiac monitor should be used for continuous respiratory and cardiac monitoring.
A physical assessment should be undertaken in the delivery room to identify malformations that were not prenatally diagnosed. A detailed newborn examination and careful observation may reveal subtle or delayed findings associated with a variety of anomalies and conditions.
Neonatal Intensive Care Unit Admission
Because multiple-pregnancy newborns are at greater risk of preterm birth, low birthweight, anomalies and other pathologic conditions, NICU admission is common. Preterm multiples of course require the same attention and care as preterm singletons, but the concurrent admission of high-risk multiplies may tax the personnel and resources of some units.
During the first hours of life in the NICU, multiple-pregnancy infants may require an array of diagnostic studies and procedures - including x-rays, central line insertion, endotracheal intubation, surfactant therapy and respiratory support - which may happen simultaneously and demand the specialised efforts of a limited group of individuals. Even after clinical acuity subsides, nurses at the bedside must constantly strive to ensure every opportunity for substantive family involvement by synchronising feeding schedules and coordinating bed placement so that siblings are proximately located in the unit.
After the initial hours and days of stabilisation, close monitoring for common setbacks must occur:
• Preterm, SGA and growth-restricted infants will require a thermal neutral environment with either a radiant warmer or a closed incubator that additionally will offer the advantage of decreased insensible water loss and provide a barrier to infection.
• Oxygen therapy, exogenous surfactant and assisted ventilation may be required to maintain adequate oxygenation. Continuous positive airway pressure or surfactant therapy may be indicated for infants with respiratory immaturity.
• A patent ductus arteriosus will often develop in the second to third hospital day. Some will require a prostaglandin antagonist such as indomethacin or ibuprofen, and surgical ligation may rarely be indicated should medical treatment fail.
• Whether enteral or parenteral, early nutrition is recommended. This may be limited by the inability of the preterm infant to suck and swallow effectively or to tolerate enteral feedings and may require parental nutrition and/or gavage feeding. Feedings should be initiated early and advanced cautiously, especially in growth-restricted newborns.
• Hyperbilirubinemia is inevitable in the smallest preterm infants and is generally managed effectively through careful monitoring of bilirubin concentrations and thoughtful use of phototherapy.
• Infection should always be considered in the preterm infant and many infants may receive short courses of antibiotics until blood cultures return negative.
• Immunisations should be administered in a full dose based on chronologic, not post- conceptional age.
• Infants at risk for retinopathy of prematurity, intraventricular haemorrhage and hearing deficit should be screened.
Admission of multiple-pregnancy newborns may present additional logistical challenges, particularly when the infants are at varying stages of illness and may require bed locations in the acute and convalescent sections of the unit. Some of these infants may qualify for transfers closer to the family's home or back to the birth hospital. Siblings seldom meet discharge criteria simultaneously and one infant is ready to be discharged or transferred before the other or others, separating multiples for days or even weeks. The NICU staff must make efforts to support parents through these difficult and vulnerable times in a caring and compassionate way.
Discharge Home and Follow-Up
Multiple-pregnancy infants born prematurely may be vulnerable and have an increased risk for long-term neurodevelopmental deficits.20 These infants are not only at increased risk for post-neonatal illness and rehospitalisation, particularly in the first year of life, but they may also be at greater risk for child abuse and neglect.18 Close follow-up by a primary care provider specialised in paediatrics or a medical provider with experience in complex care when appropriate, early intervention services and multidisciplinary infant follow-up may improve the infants' potential for normal development. Focused discharge planning is essential to ensure the family is ready and well supported for the transition to home.
Breastfeeding
Human milk and breastfeeding is the recommended standard infant nutrition by the World Health Organization (WHO) and the American Academy of Pediatrics (AAP). Evidence has demonstrated short- and long-term benefits of breast milk, particularly in preterm infants, including gut and lung anti-inflammatory properties, better cognitive outcomes, breast cancer protection for mothers and even lower risk for long-term adverse health outcomes like diabetes and obesity in adulthood. While there is strong evidence to support breastfeeding among all infants, women may have unique challenges associated with multiple birth, including frequent suckling, coordinating multiple needs and prematurity, where acute illness, NICU admission and mother-infant separation may delay and restrict breastfeeding. There are multiple options to support mothers with breast milk expression, lactation, use of pasteurised donor breast milk and different methods of supplementary feedings that may be considered.
A recent Cochrane review on breastfeeding education and support for women with twins or higher-order multiples found little consistent evidence about effective education and support practice, with evidence particularly lacking for effective interventions to support multiples.21 On the other hand, support and education have been found to improve the duration of breastfeeding in healthy term infants.
Parental Support
Having a child admitted to the NICU can be very stressful and isolating, due not only to the very technical environment, but also to the uncertainty and disrupted parental bond. Parents of multiple infants may have additional stressors compounded by having more than one infant, possibly at varying stages of illness. Many families in the NICU may have social and cultural backgrounds that may add additional barriers. Barriers like communication with families with limited local language proficiency can be bridged with translated materials and trained interpreters.
Occasionally infants may be placed in different areas of the unit and very frequently one of the infants meets discharge criteria before the sibling. The NICU staff must make efforts to support families through the stresses inherent in ‘leaving a baby (or babies) behind' and managing time between the baby(ies) at home and the one(s) still in the NICU. In worse circumstances, some families experience the emotional trauma resulting from the loss of one or more of the infants.
The mental health impact on parents, particularly of mothers, has been studied as the rate of multiple pregnancies has increased. Most studies that have compared mental health outcomes in parents of multiples versus parents of singletons found that parents of multiples experience heightened symptoms of stress, anxiety and depression. In the outpatient setting after discharge the paediatric provider should be attentive to identifying and addressing maternal depression in multiple-birth families.22
Financially, compared with singletons, multiple-birth infants consume significantly more hospital resources (e.g. increased length of stay and readmissions), particularly during the neonatal period and the first year of life. This might represent to the families a burden not only from healthcare costs, but also from lost days of earning.4
Key Points
• Multiple pregnancy is relatively common and most infants do well.
• The most common neonatal complication of multiple births is prematurity, which is the primary factor for elevated morbidity and mortality risk.
• Overall, morbidity and mortality in premature infants, including multiple-pregnancy infants, has improved due to advances in obstetric and neonatal care.
• Problems more likely to be seen in multiples compared to singletons include congenital anomalies, intrauterine growth restriction, placental complications, hypoxia and prematurity-related conditions.
• Because of the prevalence of high-risk conditions of multiple-gestation newborns, nursery staff must be prepared to identify and effectively manage the complications seen in these infants.
• Delivery room management of multiples requires individual teams to attend to the needs of the individual newborns.
• Parents of multiples may require specialised teaching, counselling and additional psychosocial support.
References
1. Martin JA, Osterman MJK. Is twin childbearing on the decline? Twin births in the United States, 2014-2018. NCHS Data Brief. 2019.
2. Murray SR, Stock SJ, Cowan S, Cooper ES, Norman JE. Spontaneous preterm birth prevention in multiple pregnancy. Obstet Gynaecol J Contin Prof Dev from R Coll Obstet Gynaecol 2018;20(1):57-63. https:// doi.org/10.1111/tog.12460
3. Adashi EY, Gutman R. Delayed childbearing as a growing, previously unrecognized contributor to the national plural birth excess. Obstet Gynecol 2018; 132 (4):999-1006. https://doi.org/10.1097/AOG.0000000000002853
4. Chambers GM, Hoang VP, Lee E et al. Hospital costs of multiple-birth and singleton-birth children during the first 5 years of life and the role of assisted reproductive technology. JAMA Pediatr 2014; 168(11):1045-53. https://doi.org/10.1001/jamapediatrics.2014.1357
5. Ely DM, Driscoll AK. Infant mortality in the United States, 2017: data from the period linked birth/infant death file. Natl Vital Stat Reports 2019;68(10):1-20.
6. Benirschke K, Kim CK. Multiple pregnancy. 1. N Engl J Med 1973;288(24):1276-84. https:// doi.org/10.1056/NEJM197306142882406
7. Fuchs F, Senat M-V. Multiple gestations and preterm birth. Semin Fetal Neonatal Med 2016;21 (2):113-20. https://doi.org/10.1016Zj.siny.2015.12.010
8. Martin JA, Hamilton BE, Osterman MJK, Driscoll AK. Births: Final data for 2019. Natl Vital Stat Reports 2021 Apr;70(2):1-51.
9. Hubinont C, Lewi L, Bernard P, Marbaix E, Debieve F, Jauniaux E. Anomalies of the placenta and umbilical cord in twin gestations. Am J Obstet Gynecol 2015;213(4 Suppl):S91-S102. https://doi.org/10.1016/j.ajog.2015.06.054
10. Boghossian NS, Saha S, Bell EF, et al. Birth weight discordance in very low birth weight twins: mortality, morbidity, and neurodevelopment. J Perinatol 2019;39 (9):1229-40. https://doi.org/10.1038/ s41372-019-0427-5
11. Benirschke K, Kim CK. Multiple pregnancy. 2. N Engl J Med 1973;288 (25):1329-36. https://doi.org/10.1056/ NEJM197306212882505
12. Spitz L, Kiely EM. Conjoined twins. JAMA 2003;289(10):1307-10. https://doi.org/10.1001/jama.289.10.1307
13. Tollenaar LSA, Slaghekke F, Middeldorp JM et al. Twin anemia polycythemia sequence: current views on pathogenesis, diagnostic criteria, perinatal management, and outcome. Twin Res Hum Genet Off J Int Soc Twin Stud 2016;19(3):222-33. https://doi.org/ 10.1017/thg.2016.18
14. Arnold C, McLean FH, Kramer MS, Usher RH. Respiratory distress syndrome in second-born versus first-born twins:
a matched case-control analysis. N Engl J Med 1987;317(18):1121-5. https://doi.org/ 10.1056/NEJM198710293171805
15. Leonard CH, Piecuch RE, Ballard
RA, Cooper BA. Outcome of very low birth weight infants: multiple gestation versus singletons. Pediatrics 1994;93 (4):611-15.
16. Babatunde OA, Adebamowo SN, Ajayi IO, Adebamowo CA. Neurodevelopmental outcomes of twins compared with singleton children: a systematic review. Twin Res Hum Genet Off J Int Soc Twin Stud 2018;21(2):136-45. https://doi.org/10.1017/thg.2018.3
17. Lorenz JM. Neurodevelopmental outcomes of twins. Semin Perinatol 2012;36(3):201- 12. https://doi.org/10.1053/j.semperi.2012.02.005
18. McCormick MC, Shapiro S, Starfield BH. Rehospitalization in the first year of life for high-risk survivors. Pediatrics 1980;66 (6):991-9.
19. Raju TNK, Buist AS, Blaisdell CJ, Moxey- Mims M, Saigal S. Adults born preterm:
a review of general health and system-specific outcomes. Acta Paediatr 2017; 106(9):1409- 37. https://doi.org/10.1111/apa.13880
20. Litt JS, McCormick MC. Preterm infants are less likely to have a family-centered medical home than term-born peers. J Perinatol 2018;38
(10):1391-7. https://doi.org/10.1038/s413 72-018-0180-1
21. Whitford HM, Wallis SK, Dowswell T, West HM, Renfrew MJ. Breastfeeding education and support for women with twins or higher order multiples. Cochrane Database Syst Rev 2017 Feb 28;2(2): CD012003.https://doi.org/10.1002/ 14651858.CD012003.pub2
22. Wenze SJ, Battle CL, Tezanos KM. Raising multiples: mental health of mothers and fathers in early parenthood. Arch Womens Ment Health 2015;18(2):163-76. https:// doi.org/10.1007/s00737-014-0484-x