Nutrition in pregnancy
The average weight gain in pregnancy in a woman of a normal BMI is 12.5 kg although this varies greatly between individuals. This increase in weight is due to increased blood volume and retention of water, the increased size of maternal tissues such as uterus and breasts, the products of conception, and greater maternal fat stores.
The basal metabolic rate increases by approximately 5% by term in a woman of a normal BMI (56). Total fat deposited by the mother is between 2 and 6 kg. This is stored during the second trimester in preparation for the increased metabolic demands of late pregnancy and lactation (57). This process is regulated by the hormone leptin which alerts the brain to the extent of the fat stores. Recent studies suggest that the sensitivity of the brain to the effects of leptin is reduced in pregnancy, allowing the mother to deposit greater fat stores (58).Following delivery there is immediate weight loss of 6 kg associated with delivery of the baby and other products of conception. Diuresis of the water retained in pregnancy occurs in the days following delivery. From day 3, body weight decreases by 0.3 kg a day until day 10. This stabilizes at 10 weeks after delivery where weight is approximately 2.3 kg greater than prepregnancy weight. The average weight gain at 6-18 months after delivery is 1-2 kg but in approximately 20% of women this is greater than 5 kg (59).
In pregnancy, the total protein concentration decreases by about 1 g/dL during the first trimester and then plateaus. This represents a reduction from 7 to 6 g/dL. Albumin concentration decreases more dramatically in the first and second trimester then more slowly until late pregnancy. Typically, this represents a reduction from 3.5 to 2.5 g/ 100 mL. It is this that causes the majority of the decrease in total protein content; the reason is unknown.
The decrease in albumin concentration causes a reduction in total plasma calcium but unbound ionized calcium levels are unchanged. Increased synthesis of 1,25- dihydroxycholecalciferol promotes increased calcium absorption from the intestines. This is doubled by 24 weeks but then plateaus.In contrast, pregnancy is associated with a considerable rise in circulating free fatty acids and most plasma lipids. The main components of total lipids are triglycerides, cholesterol, phospholipids, and free fatty acids. In total, the serum lipid concentration rises from 600 to 1000 mg/100 mL. The greatest changes are the threefold increase in very low-density lipoprotein (VLDL) triglycerides and 50% increase in VLDL cholesterol (60). The levels of VLDL triglyceride directly correlates to the birthweight and placental weight at term. Lipids undergo peroxidation as part of normal cellular function. Excess production of lipid peroxidases causes oxidative stress. In normal pregnancy, the plasma lipid peroxidases increase in the second trimester but there are also increased endogenous antioxidants which are thought to protect the mother and prevent the atherogenic effects of hyperlipidaemia (61).
Glucose is the main substrate for fetal growth and nutrition and it readily crosses the placenta. Fetal glucose levels are closely correlated with maternal levels but are 15-20% lower. Blood glucose levels in the mother are regulated by insulin which is increased in pregnancy. Longitudinal studies demonstrate a decrease in plasma glucose levels in pregnancy, a nadir is reached at 12 weeks of gestation at 0.5-1 mmol less than the prepregnancy level (62). By the end of the first trimester, the increase in blood glucose following a carbohydrate load is less than outside pregnancy (62). Increased resistance to the action of insulin develops from mid pregnancy and plasma glucose concentrations rise towards term, although normally remaining below that of non-pregnant levels—this is shown in Figure 8.4.
This reduced sensitivity to insulin is thought to be driven by human placental lactogen or cortisol. As well as moving glucose into cells, transport of amino acids and free fatty acids is also increased.Clinical considerations
Obesity is associated with pre-existing insulin resistance which increases under the influence of pregnancy hormones, therefore much higher insulin levels are required to prevent glucose levels from rising. More marked insulin resistance in pregnancy will cause chronically elevated blood glucose and be classified as gestational diabetes.
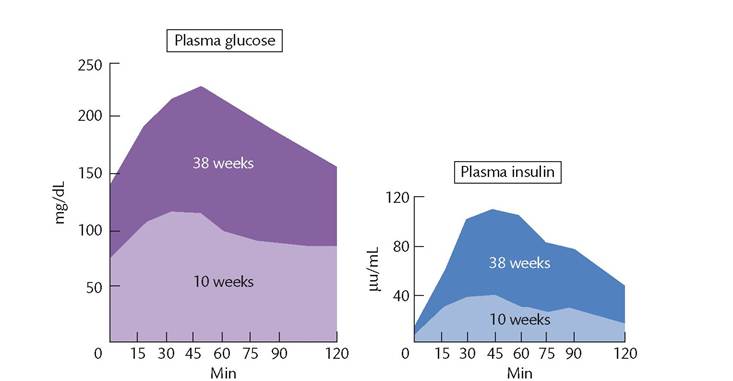
Figure 8.4 Responses in normal pregnant women to a 50 g oral glucose load during early and late pregnancy. During early pregnancy, there is a normal plasma insulin response with a relative reduction in plasma glucose concentration compared to the non-pregnant state. In contrast, during late pregnancy, plasma glucose concentrations reach higher levels after a delay despite a considerably enhanced insulin response, a pattern which could be explained by relative resistance to insulin.