Overview of treatment at primary presentation
Surgical staging and treatment of primary epithelial ovarian and fallopian tube cancers
Surgery is the cornerstone of management for early and advanced ovarian cancer. For early ovarian cancer the aim of surgery is to remove the primary tumour and perform adequate staging to exclude occult advanced disease in the omentum and lymph nodes.
In advanced stage the aim is maximal tumour reduction, as this has clearly been shown to be associated with a better prognosis. Nonfertility-sparing surgery for disease macroscopically confined to the ovary consists of peritoneal washings or cytology, ideally taken prior to manipulation of the tumour, bilateral salpingo-oophorectomy, hysterectomy, multiple peritoneal biopsies from the paracolic and subdiaphragmatic spaces bilaterally, infragastric omentectomy, and pelvic and bilateral para-aortic lymph node dissection up to the level of the renal vessels. If mucinous carcinoma is suspected, an appendicectomy should be considered. Depending on the histological grade and subtype, up to 30% of the patients with apparently early epithelial ovarian cancer will be upstaged after comprehensive surgical staging (11). The extent of lymph node dissection remains controversial but one prospective randomized trial showed that systematic lymph node dissection compared to sampling in early disease identified an additional 13% of patients (from 9% to 22%) with occult lymph node disease (12). No clear evidence exists to suggest that systematic lymph node dissection is therapeutic and improves survival. In stage IA mucinous cancer, the incidence of lymph node spread is extremely low and there is no value in performing a lymphadenectomy.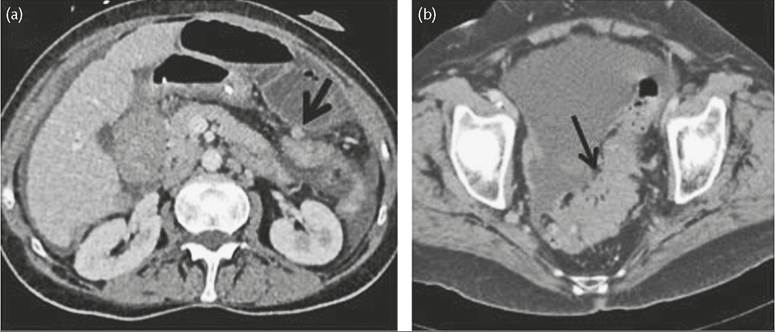
Figure 64.1 False-positive tumour involvement described preoperatively on CT on transverse colon (a); which was intraoperatively part of the omental cake, and of sigmoid colon (b) which was a parasigmoid nodule without affecting the bowel.
Fertility-sparing surgery should be considered and discussed with patients of childbearing age who have early-stage disease, informing patients of the risks and benefits of such an approach. Patients with stage IA and favourable histology, that is, low-grade, mucinous, serous, endometrioid, or mixed histology have been shown to have a lower risk of recurrence after fertility-preserving surgery compared to patients with a higher stage (IC3) or grade, or clear cell histology (13). Retrospective studies showed a risk of 3.5-11% of positive contralateral pelvic lymph nodes in women with unilateral disease despite negative ipsilateral nodes (14, 15). Thus, pelvic lymph node staging should be bilateral.
Total macroscopic tumour clearance of advanced disease has consistently been shown to be associated with a significantly better progression-free survival (PFS) and overall survival (16-18). However, it is unclear if this association is causal or whether resectable tumours intrinsically respond better to chemotherapy and have a more favourable prognosis (19). In a systematic meta-analysis based on 53 studies with 6885 patients overall (period: 1989-1998), Bristow and colleagues (20) showed how the degree of surgical tumour resection influenced the overall survival of patient cohorts. Those with over a 75% rate of ‘optimal’ cytoreduction (defined as <2 cm residual disease) had a median overall survival of 36.8 months. By contrast, patient cohorts with a maximum tumour reduction rate of less than 25% had a median overall survival of only 23 months. Every 10% reduction in tumour burden was associated with a 6.3% prolongation of median overall survival. In order to achieve total macroscopic tumour clearance of peritoneally disseminated disease, a maximal surgical effort is required, incorporating multivisceral resection techniques such as extensive peritoneal stripping, fullthickness diaphragmatic resection, removal of bulky pelvic and para-aortic lymph nodes, splenectomy, and bowel resection.
In a randomised trial the value of systematic lymph node dissection as a therapeutic procedure has been shown not to improve outcome (LION Trial, AGO-OVAR OP.3 (NCT00712218))(21). Increasingly, more extra-abdominal cytoreductive techniques are being applied, including resection of cardiophrenic or paracardiac lymph nodes, pleurectomy, and supraclavicular and axillary lymph node dissection. Surgical expertise and training with continuous feedback of surgical outcome, morbidity, and survival have been proven to be important tools to make extensive surgery safer for the patient (22). There is now a national and international trend towards specialization of such procedures in centres with adequate infrastructure, resources, and training.Interval debulking surgery after merely a biopsy, or little or low- effort surgical debulking at diagnosis has been shown to improve survival (17), but in situations where maximal effort primary surgery has been undertaken but no total macroscopic tumour clearance could be achieved, there is no survival benefit in interval cytoreductive surgery after three cycles of chemotherapy to clear any remaining disease and it should therefore not be attempted (23). Similarly, a ‘second-look’ diagnostic laparoscopy or laparotomy after completion of treatment to assess intraperitoneal status should not be routinely performed, except in the context of clinical trials, as its impact on survival has not been demonstrated.
There is internationally ongoing debate as to the best timing of surgery in relation to first-line chemotherapy. Two prospective randomized trials (18, 24) have demonstrated lower surgical morbidity and mortality and equivalent overall survival using a neoadjuvant (primary chemotherapy) approach. The weakness of both studies was, however, that the rate of complete resection was low and operation time, a surrogate marker of surgical effort, was short. Accordingly, it is difficult to adopt neoadjuvant chemotherapy for patients with good performance status who can be rendered tumour free by surgery in specialized centres.
A trial comparing neoadjuvant chemotherapy and upfront radical surgery in such centres where surgical quality is established is being planned. There is, however, a significant value of using neoadjuvant chemotherapy in patients with unresectable FIGO IVB disease, low performance status, and significant comorbidities that would make radical debulking surgery impossible.Systemic treatment of high-grade serous epithelial ovarian, fallopian tube, and peritoneal cancers
Adjuvant therapy for early-stage ovarian cancer
Cytotoxic chemotherapy plays a key role in the treatment of ovarian cancers. Postoperative chemotherapy should be distinguished from adjuvant chemotherapy used to treat some women with FIGO stage I disease. In this group, platinum chemotherapy has been shown in two trials to reduce the recurrence rate and prolong overall survival (25). However, these trials were done many years ago when the quality of surgical staging was less good, and the studies are likely to have included women with occult FIGO stage III disease. Nevertheless, with a 10-year median follow-up of the ICON1 trial there was in absolute terms a 10% (from 60% to 70%) improvement in recurrence- free survival and a 9% (from 64% to 73%) improvement in overall survival. Patients with high-grade tumours appeared to derive the greatest benefit (26). However, the long-term results of the EORTC ACTION trial still cast doubt on the value of adjuvant chemotherapy as the 10-year follow-up data showed that only patients who had ‘suboptimal’ surgery benefited from chemotherapy (27).
Chemotherapy for advanced ovarian cancer and recent trial results
Advanced ovarian cancer is one of the most chemosensitive epithelial malignancies and platinum-based therapy has been the mainstay of cytotoxic treatment since the late 1970s. Carboplatin has equivalent activity to cisplatin, but has less neurotoxicity and renal toxicity, and is the key drug used to treat ovarian cancer. The addition of paclitaxel improves tumour response rates, prolongs PFS, and probably increases overall survival (28).
Since the late 1990s, the standard of care has been a combination of carboplatin and paclitaxel, given three-weekly for six cycles. The key additional toxicities of paclitaxel are hair loss and peripheral neuropathy. Single-agent carboplatin is used in a minority of women through choice to avoid the additional side effects, or concern about the extra toxicity from paclitaxel. However, carboplatin and pegylated liposomal doxorubicin (PLD) is an alternative combination (29). Over the last 15 years, trials adding additional drugs, either as triplet therapy, sequential doublets, maintenance post carboplatin-paclitaxel, or the use of very high-dose chemotherapy have failed to improve the median PFS. Intraperitoneal delivery is an approach that has been investigated for many years and is discussed in the ‘Intraperitoneal chemotherapy and hyperthermic intraperitoneal chemotherapy’ section.Recently, modification of paclitaxel administration, using a weekly (dose-dense) schedule has been shown to increase median PFS from 17.5 to 28.1 months and median overall survival from 62.2 to 100.5 months compared to the three-weekly schedule (30). These data in a Japanese population are provocative and have generated further studies to try and confirm the results. Two trials used a similar design but had key differences to the Japanese study (weekly carboplatin and lower dose of paclitaxel in one, and the addition of bevacizumab in the other) and they failed to confirm a benefit of weekly paclitaxel (31, 32). A third study, ICON8 (NCT01654146), which directly compares the arms in the Japanese trial and has a third arm where both drugs are given weekly has also shown no benefit for weekly paclitaxel (33). Currently, three-weekly carboplatin and paclitaxel remains the standard schedule.
Novel targeted approaches
Targeting the complex molecular pathways responsible for tumour growth is now believed to be the best strategy to improve treatment outcome. Remission of tumours to first-line cytotoxic therapy is not uncommon but eradication is unusual.
What happens to tumours from this time until progression is poorly understood, but two main theories predominate: there is evidence that tumour growth is dependent upon angiogenesis and once an antiangiogenic ‘switch’ or other complex micro-environmental changes occurs, tumour will regrow (34). Another hypothesis is that tumour growth arrest may be partly under immunological control. Antiangiogenic therapy with a monoclonal antibody, bevacizumab, that targets circulating vascular endothelial growth factor-A (VEGF-A), one of the key ligands driving angiogenic growth, has been shown to result in tumour shrinkage and delayed progression of ovarian cancer. Two key large randomized studies in first-line treatment after surgery, Gynecologic Oncology Group (GOG) 218 and ICON7, showed that median PFS was extended in both trials (by 3.8 and 1.7 months respectively) by giving bevacizumab with chemotherapy and then as maintenance for a year or more (35, 36). There was no difference in overall survival although in a subgroup of women at ‘high risk’ of recurrence (stage IV; ≥1 cm residual disease stage III, or no surgery) in ICON7, which used half the dose of bevacizumab compared to GOG 218, there was a significant survival benefit favour of bevacizumab (37). The interpretation of the results differed between Europe, where bevacizumab is licensed for use in first-line treatment and the United States, where it was licensed almost 7 years later. Bevacizumab is generally well tolerated; hypertension and proteinuria are the most common adverse effects, and the most serious but rare event is bowel fistula or perforation. It is generally used after surgery although trials in the neoadjuvant setting are in progress. However,the greatest improvement has been in the first-line treatment of advanced BBCA-mutated ovarian cancer where post chemotherapy treatment with olaparib, a PARP inhibitor led to a 70% reduction in the risk of progression (60% patients free of progression at 3 years compared to 27% in the control arm) (38).Intraperitoneal chemotherapy and hyperthermic intraperitoneal chemotherapy
The concept of using intraperitoneal (IP) chemotherapy remains controversial with conflicting data relating to its efficacy compared to intravenous therapy, and its toxicity. However, randomized clinical trials have consistently favoured an improvement in survival with IP chemotherapy, comprehensively reviewed by Trimble et al. (39). Long-term follow-up of the most recently published trial, GOG 172, demonstrated a survival benefit extending beyond 10 years (40). Cisplatin and paclitaxel are the two drugs usually used. However, because of concerns about toxicity and the complexity of treatment, IP chemotherapy has not been widely adopted. Carboplatin is less toxic and the results of a Japanese trial comparing IP and intravenous carboplatin are awaited (NCT01506856). Uncertainty about the benefit of the IP strategy remains following the recent negative preliminary results from GOG 252, a phase III trial comparing IP and intravenous therapy with the inclusion of bevacizumab (41).
There are even fewer data to support the use of HIPEC (hyperthermic intraperitoneal chemotherapy), a high dose ofintraperitoneal chemotherapy under hyperthermic conditions. Most publications are from single centres in a heterogeneous patient population with primary or recurrent disease. Only one randomised trial has supported this approach, so, data should be interpreted with caution (42). Currently, treatment should only be encouraged within the context of trials and several randomized trials are in progress.
Low-grade serous tumours
These represent about 10% of ovarian cancer cases and have a different biological behaviour from the more common high-grade tumours, with slower growth and less frequent spread beyond the ovary. Surgery for primary or recurrent disease is the mainstay of treatment; the role of chemotherapy is less clear. In the absence of randomized trials, therapeutic decisions are based largely on case series. Low-grade serous tumours do respond to platinum-based therapy but less well and frequently than high-grade tumours (43). A large meta-analysis showed a response to platinum-based chemotherapy of approximately 24% in patients with advanced, primary, low-grade ovarian cancer after upfront surgery (44). Chemotherapy, hormone therapy, and observation are all options to consider in women with low-volume residual disease after primary surgery. Even less is known about the activity of cytotoxic drugs for recurrent disease. Inoperable recurrent disease is more chemoresistant; tamoxifen or aromatase inhibitors are often used and bevacizumab may also be active in modifying growth (45-47).
Recently, there has been interest in exploiting mutations in the BRAF and KRAS pathways and the constitutive activation of the MAPK-ERK pathway using inhibitors of MEK. Initial results have shown some activity of these compounds (48) that are now being investigated in randomized trials.
Non-serous tumours
Classification of this group is becoming more complex, particularly for endometrioid tumours, some of which behave more like high-grade serous cancers while others have clear cell components. Pure clear cell tumours represent about 5% of ovarian cancers, but are more common in Japan and the Far East. They respond less well to platinum-based therapies than serous tumours. Many clear cell tumours present with early-stage disease and these have a relatively good prognosis (49, 50). For advanced disease, the outlook is much less good although carboplatin and paclitaxel are usually given. A recent trial comparing this combination with cisplatin and irinotecan failed to show any difference in outcome (51). Future treatment needs to be directed against molecular targets and work to identify these is underway (52). True mucinous tumours of the ovary are rare, and most present at an early stage with a good prognosis. Advanced mucinous cancers carry a poor prognosis. Carboplatin and paclitaxel are often given although there are good reasons to consider drugs such as oxaliplatin and fluoropyrimidine-based therapy that are active in gastrointestinal mucinous tumours. Because of the rarity of these tumours, it has been difficult to complete randomized trials comparing these combinations (53).