I PATIENT SAFETY ^147 ^167 ^208 ^738
Patient safety shares many characteristics with a well-designed quality improvement model. However, patient safety emphasizes a systems analysis of medical errors and minimizes individual blame and retribution while still maintaining individual accountability.
Patient safety is an explicit principle that must be embraced as a core value in patient care. This is an ongoing process that requires health care providers to continually strive to learn from problems, identify system deficiencies, redesign processes, and implement change in their daily practice. Patient-centered care, open communication, and teamwork provide the foundation for optimal patient care and safety.National Patient Safety Goals
The Joint Commission recognizes the importance of patient safety. In 2003, it created the first set of National Patient Safety Goals. These goals, derived from Sentinel Event Alerts and other sources, are designed to be explicit, evidence based, and measurable. Each year, The Joint Commission modifies existing goals based on public comment and the experience of its reviewers, and new goals are added. In this way, over time, The Joint Commission will develop a compendium of recommended practices that will improve patient safety (see www.jointcommission.org/standards_ information/npsgs.aspx).
Patient Safety Principles
The American College of Obstetricians and Gynecologists (the College) continues to emphasize its longstanding commitment to quality improvement and patient safety by codifying a set of objectives to improve patient care and reduce medical errors. The College encourages all obstetriciangynecologists to promote the following principles in all practice settings:
• Develop a commitment to encourage a culture of patient safety.
• Implement recommended safe medication practices.
• Reduce the likelihood of surgical errors.
• Improve hand hygiene.
• Improve communication with health care providers and patients.
• Make safety a priority in every aspect of practice.
Develop a Culture of Patient Safety
A culture of patient safety (see Box 1-8) continuously evolves and should be the framework for every effort to reduce medical errors. Patient safety focuses on systems of care, not individuals. Confidential reporting and analysis of errors and near misses will reveal areas that require system changes, not individual punishment, to improve patient safety. State and
Box 1-8. A Culture of Patient Safety
Although an exact definition of a culture of patient safety does not exist, a recurring theme in the literature is that organizations with effective safety cultures share a constant commitment to safety as a top-level priority, which permeates the entire organization. Noted components include the following:
• Acknowledgment of the high-risk nature of an organization’s activities and the determination to achieve consistently safe operations
• A blame-free environment where individuals are able to report errors or near misses without fear of reprimand or punishment
• Encouragement of collaboration across ranks and disciplines to seek solutions to patient safety problems
• Organizational commitment of resources to address safety concerns
Data from Agency for Healthcare Research and Quality. Patient safety primers: Safety Culture. Available at: http://psnet.ahrq.gov/primer.aspx?primerID=5. Retrieved October 28, 2013.
federal laws may have an effect on the level of confidentiality and the manner of reporting.
A culture of patient safety starts at the top with strong leadership that provides the necessary human and financial resources to maximize patient safety. Additionally, a culture of patient safety recognizes the importance of team function in optimizing individual performance. Essential to this team effort is effective leadership, communication, collaboration, situational awareness, and mutual respect.
Associated with a safety culture is the concept of a “just culture,” which recognizes that competent professionals make mistakes and acknowledges that even competent professionals may develop unhealthy norms, such as shortcuts or routine rule violations, but has zero tolerance for reckless behavior.Implement Recommended Safe Medication Practices
Medication errors are one of the most common types of preventable adverse events. Automated systems for prescribing and dispensing medication can reduce, but will not eliminate, these errors; however, many “low- tech” solutions can be implemented rapidly, with minimal costs:
• Improve the legibility of written orders.
• Ensure the completeness of medical orders, including the name of the drug, dose, route of administration, frequency or rate, reason or conditions under which the drug should be administered (if prescribing with directions to take as required), and patient’s weight and age (if relevant to dosing).
• Avoid nonstandard abbreviations, as recommended by The Joint Commission (see Table 1-1).
• Always use a leading 0 for doses less than 1 unit (eg, 0.1, not.1), and never use a trailing 0 after a decimal point (eg, 1 mg, not 1.0 mg): “Always lead, never follow.”
• Provide the reasons for giving the medication or the parameters for giving a pro re nata (p.r.n.) dose. This is particularly helpful in preventing errors with medications that sound alike and look alike or for medications that are to be given on an as-needed basis (eg, p.r.n. for moderate-to-severe cramping, rather than simply p.r.n.).
• Ensure that all verbal orders are written by the individual receiving the order and then read back to the prescriber. Verbal orders should be limited to urgent situations in which written or electronic orders are not feasible. Because many drugs have soundalike names, it is also helpful to include the indication for the drug in verbal medication orders.
Table 1-1. The Joint Commission’s Official “Do Not Use” Abbreviations List*
| Do Not Use | Potential Problem | Use Instead |
| U, u (unit) | Mistaken for “0” (zero), the number “4” (four), or “cc” | Write “unit” |
| IU (International Unit) | Mistaken for IV (intravenous) or the number 10 (ten) | Write “International Unit” |
| Q.D., QD, q.d., qd (daily) | Mistaken for each other | Write “daily” |
| Q.O.D., QOD, q.o.d., qod (every other day) | Period after the Q mistaken for “I” and the “O” mistaken for “I” | Write “every other day” |
| Trailing zero (X.0 mg)t | Decimal point is missed | Write “X mg” |
| Lack of leading zero (.X mg) | Decimal point is missed | Write “0.X mg” |
| MS | Can mean morphine sulfate or magnesium sulfate | Write “morphine sulfate” |
| MSO4 and MgSO4 | Confused for one another | Write “magnesium sulfate” |
*Applies to all orders and all medication-related documentation that is handwritten (including free-text computer entry) or on preprinted forms.
tException: A “trailing zero” may be used only where required to demonstrate the level of precision of the value being reported, such as for laboratory results, imaging studies that report size of lesions, or catheter and tube sizes. It may not be used in medication orders or other medication-related documentation.
Copyright The Joint Commission, 2013. Reprinted with permission. The Joint Commission. Facts about the official “Do Not Use” List. Oakbrook Terrace (IL): Joint Commission; 2013. Available at: http://www.jointcommission.org/assets/1/18/Do_Not_Use_List.pdf. Retrieved July 10, 2013.
Reduce the Likelihood of Surgical Errors
In 2003, The Joint Commission published “Universal Protocol for Preventing Wrong Site, Wrong Procedure, Wrong Person Surgery” (see www.jointcommission.org/standards_information/up.aspx). This protocol complements the World Health Organization Surgical Safety Checklist, last revised in 2009 (see Fig.1-2).
The Universal Protocol involves the completion of three principal components before initiation of any surgical procedure:
1. Preprocedure verification process. The health care team ensures that all relevant documents and studies are available before the procedure starts; are correctly identified, labeled, and matched to the patient’s identifiers; and are reviewed and are consistent with the team’s understanding of the intended patient, procedure, and site. The team must address missing information or discrepancies before starting the procedure.
2. Marking the operative site. Procedures that require marking of the incision or insertion site include those in which there is more than one possible location for the procedure or when performing the procedure in a different location would negatively affect quality or safety. Although The Joint Commission does not require a specific site-marking method, each facility should be consistent in the method it uses to ensure that the mark is unambiguous. Only the correct site should be marked; an “X” or “No” should never be used on the wrong side.
3. Performing a “time out” before the procedure. The operative team (anesthesia personnel, surgeons, and nurse) conducts a final assessment to verify that the correct patient, site, and procedure are identified; admittedly, this is problematic in emergency situations.
An essential element of this overall process is the formal enlistment of active involvement by the patient to avert errors in the operative arena. Involving the patient in this manner requires personal effort by the surgeon to educate the patient during the preoperative evaluation process. The patient, who has the greatest stake in avoiding errors, thus becomes integrally involved in helping ensure that errors are avoided.
Surgical Safety Checklist
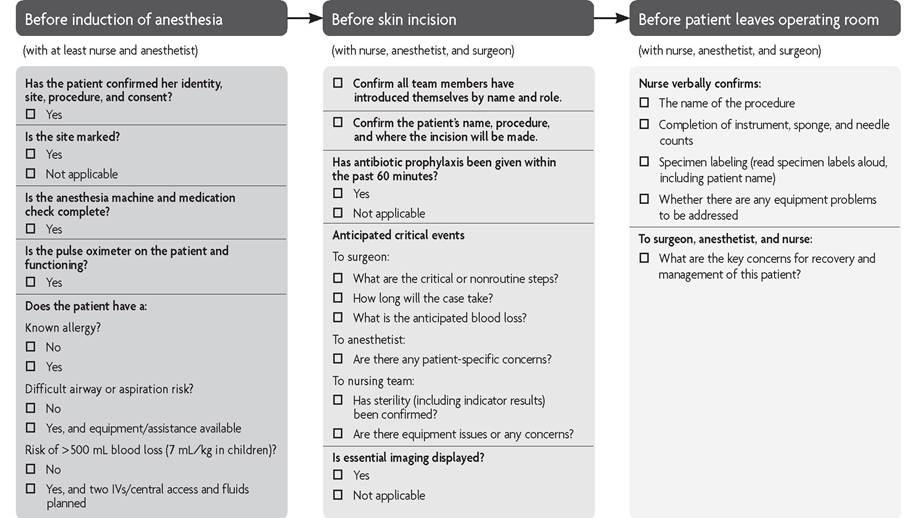
Fig. 1-2. World Health Organization’s surgical safety checklist. Abbreviation: IV, intravenous. This checklist is not intended to be comprehensive. Based on the WHO Surgical Safety Checklist, URL http://whqlibdoc.who.int/publications/2009/9789241598590_eng_ Checklist.pdf. Copyright World Health Organization 2009. All rights reserved, The Joint Commission’s National Patient Safety Goal 7 requires adherence to current World Health Organization or Centers for Disease Control and Prevention hand hygiene guidelines. Other organizations have endorsed effective hand washing guidelines, including the American Medical Association, the American Academy of Family Physicians (four principles of hand awareness), Agency for Healthcare Research and Quality, the Institute for Healthcare Improvement, and the College. The critical importance of proper hand hygiene, especially for prevention of methicillin-resistant Staphylococcus aureus, is well known and documented throughout the medical literature.
Numerous suggestions have been found to help improve hand hygiene campaigns in hospitals across the country. A hand hygiene awareness program may include posters, buttons, lapel pins, stickers, posted signs at every sink, and frequent reminders for all members of the health care team.
Some institutions have encouraged patient involvement with information in every patient care area asking patients to remind caregivers to cleanse their hands before and after each patient contact, especially with systems of “gel in, gel out” that utilize convenient hand sanitizer dispensers in every patient care location.Improve Communication With Health Care Providers and Patients
Physicians should be aware that complete and accurate communication of medical information is imperative for reducing preventable medical errors. Improving communication skills merits the same attention as improving surgical skills. According to information gathered from The Joint Commission in collecting sentinel event information, the most common cause of preventable adverse outcomes is communication error. Additionally, patient-physician communication problems may increase professional liability actions. Optimal communication to improve patient safety has many dimensions, including the following:
• Communication with patient and family
• Communication among all individuals caring for the patient
• Availability of information necessary for coordination of care
Communication With Patients
The key to a good patient-clinician relationship is the ability to listen, explain, and empathize. The U.S. Preventive Services Task Force defines shared decision making as a process in which the patient and clinician share information, participate in the decision-making process, and agree on a course of action. Patients who are involved in making their health care decisions have better outcomes than those who are not. Patients should be encouraged to ask questions about medical procedures, the medications they are taking, and any other aspect of their care.
According to an Institute of Medicine report, “nearly half of all American adults—90 million people—have difficulty understanding and acting upon health information.” To have a meaningful discussion with an individual about her health care, it is imperative that one recognize and address her level of understanding and knowledge. Consider the following options to improve communication, elevate the level of understanding, and improve health literacy:
• Listen to the patient and understand her concerns and issues.
• Ask open-ended questions using the words “what” or “how” to start the sentence. (For example: “What questions do you have for me?” rather than “Do you have any questions?”)
• Use familiar language and avoid jargon. (For example, “You may have itching” instead of “You may experience pruritus.”)
• Have patients bring a family member or friend when difficult and crucial discussions are held.
• Check for comprehension by asking patients to restate the health information given in their own words. (For example: “Tell me how you are going to take this medication.”) This is particularly useful during the informed consent process.
• Limit the amount of information provided.
• Use visual aids such as drawings or models for key points. Make sure the visual messages are culturally relevant.
• Do not rush encounters. Take as much time as is needed for patient comprehension.
A very important part of patient-physician communication is when and how to disclose medical errors. The Joint Commission requires that accredited hospitals inform patients of adverse events. When an error contributed to the injury, the patient and the family or representative should receive a truthful and compassionate explanation about the error and the remedies available to the patient. They should be informed that the factors involved in the injury will be investigated so that steps can be taken to reduce the likelihood of similar injury to other patients. The improvement of the disclosure process through policies, programmatic training, and available resources will enhance patient satisfaction, strengthen the patientphysician relationship, potentially decrease litigation, and most importantly promote higher quality health care.
Cultural Sensitivity and Awareness
Cultural sensitivity and awareness in the delivery of health care can improve patient communication and care. Cultural competency encompasses gender, sexual orientation, socioeconomic status, faith, profession, tastes, disability, age, as well as race and ethnicity. Physicians should be sensitive to the unique needs of women in the communities they serve. Sensitivity to patients’ reactions and possible behavioral differences will alert clinicians to ask appropriate questions and take appropriate actions. The National Standards for Culturally and Linguistically Appropriate Services in Health Care, published by the U.S. Department of Health and Human Service’s Office of Minority Health, provide a framework for all health care organizations to best serve the nation’s increasingly diverse communities. These standards and their guide for implementation (known as The Blueprint) offer guidance on how to advance health equity, improve quality, and help eliminate health care disparities under three main areas: 1) governance, leadership, and workforce; 2) communication and language assistance; and 3) engagement, continuous improvement, and accountability.
In general, family and friends should not be used to provide interpretation services. For those who do not speak English, efforts should be made to provide assistance, such as offering medically trained interpreters and written translations of forms and patient education materials. In some circumstances, federal and state laws and regulations impose responsibilities on health care providers to accommodate individuals with limited English proficiency. Appropriate measures for overcoming communication barriers will depend on the circumstances of the individual practice and patient population. Various options may be available, including hiring bilingual staff for clerical or medical positions, using appropriate community resources, or using translation telephone services. Because patients interact with many individuals in the office and hospital, it is important to educate the front desk, billing, nursing, and ancillary medical staff in cultural sensitivity.
The Americans With Disabilities Act requirement to provide “auxiliary aids and services” includes a responsibility of making aurally delivered materials accessible for hearing disabled patients. This may be accomplished through multiple means, including qualified interpreters, note taking, written materials, and telecommunications devices for deaf individuals. The Americans With Disabilities Act does not mandate the use of interpreters in every instance. The health care provider can choose alternatives to interpreters, as long as the result is effective communication.
Communication With Health Care Providers
A culture of patient safety fosters open communication and welcomes input from team members at every level. Care must be taken to ensure that hierarchical systems do not hamper free communication among clinicians. Good communication promotes and fosters better medical care. It requires that all members of the team work in concert. A successful team includes the administrative staff and clinicians. Open communication, collaboration, mutual respect, and trust are necessary to provide quality patient care. As noted in the Code of Professional Ethics of the American College of Obstetricians and Gynecologists, “The obstetrician-gynecologist’s relationships with other physicians, nurses, and health care providers should reflect fairness, honesty, and integrity, sharing a mutual respect and concern for the patient” (see also Appendix A). There should be an established policy to resolve conflicts.
Patient Handoffs and Coordination of Care
Physician-to-physician handoff of patient information is one of the most important factors to focus on to prevent discontinuity of care, eliminate preventable errors, and provide a safe patient environment. Competing clinical demands, interruptions, and distractions are inherent in clinical practice. Specific effort is needed to ensure that issues are understood and that meaningful information is transferred. Certain clinical communications should be verified, such as reading back medication orders. Relevant communications should be documented appropriately.
Make Safety a Priority in Every Aspect of Practice
The discipline of obstetrics and gynecology has a long tradition of leadership in quality improvement activities, which have been associated with an increase in patient safety.
Patient safety is an explicit principle that must be embraced as a core value in patient care. This ongoing process requires health care providers to strive continually to learn from problems, identify system deficiencies, redesign processes, and implement change in their daily practice. Opportunities to improve patient safety should be used whenever identified. Emphasizing compassion, communication, teamwork, and patient- focused care will aid in creating a culture of excellence and provide the foundation for optimal patient care and safety.
Bibliography
Agency for Healthcare Research and Quality. Patient safety primers: Safety Culture. Available at: http://psnet.ahrq.gov/primer.aspx?primerID=5. Retrieved on October 28, 2013.
American College of Obstetricians and Gynecologists. Code of professional ethics of the American College of Obstetricians and Gynecologists. Washington, DC: American College of Obstetricians and Gynecologists; 2011. Available at: http:// www.acog.org/~/media/Departments/National%20Officer%20Nominations%20 Process/ACOGcode.pdf?dmc=1&ts=20130715T1226302728. Retrieved July 15, 2013.
American College of Obstetricians and Gynecologists. Quality and safety in women's health care. 2nd ed. Washington, DC: American College of Obstetricians and Gynecologists; 2010.
Communication strategies for patient handoffs. Committee Opinion No. 517. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012; 119:408-11. [PubMed] [Obstetrics & Gynecology]
Cultural sensitivity and awareness in the delivery of health care. Committee Opinion No. 493. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;117:1258-61. [PubMed] [Obstetrics & Gynecology]
Department of Health and Human Services, Office of Minority Health. National standards for culturally and linguistically appropriate services (CLAS) in health and health care. Available at: https://www.thinkculturalhealth.hhs.gov/pdfs/ EnhancedNationalCLASStandards.pdf. Retrieved September 26, 2013.
Department of Health and Human Services, Office of Minority Health. National standards for culturally and linguistically appropriate services in health and health care: a blueprint for advancing and sustaining CLAS policy and practice. Rockville (MD): OMH; 2013. Available at: https://www.thinkculturalhealth.hhs.gov/pdfs/ EnhancedCLASStandardsBlueprintpdf Retrieved September 26, 2013.
Disclosure and discussion of adverse events. Committee Opinion No. 520. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;119:686-9. [PubMed] [Obstetrics & Gynecology]
Effective patient-physician communication. Committee Opinion No. 587. American College of Obstetricians and Gynecologists. Obstet Gynecol 2014;123:389-93. [PubMed] [Obstetrics & Gynecology]
Fatigue and patient safety. Committee Opinion No. 519. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;119:683-5. [PubMed] [Obstetrics & Gynecology]
Health literacy. Committee Opinion No. 585. American College of Obstetricians and Gynecologists. Obstet Gynecol 2014;123:380-3. [PubMed] [Obstetrics & Gynecology]
Informed consent. ACOG Committee Opinion No. 439. American College of Obstetricians and Gynecologists. Obstet Gynecol 2009;114:401-8 [PubMed] [Obstetrics & Gynecology].
Partnering with patients to improve safety. Committee Opinion No. 490. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;117:1247-9. [PubMed] [Obstetrics & Gynecology]
Patient safety and the electronic health record. Committee Opinion No. 472. American College of Obstetricians and Gynecologists. Obstet Gynecol 2010; 116:1245-7. [PubMed] [Obstetrics & Gynecology]
Patient safety in obstetrics and gynecology. ACOG Committee Opinion No. 447. American College of Obstetricians and Gynecologists. Obstet Gynecol 2009; 114:1424-7. [PubMed] [Obstetrics & Gynecology]
Patient safety in the surgical environment. Committee Opinion No. 464. Obstet Gynecol 2010;116:786-90. [PubMed] [Obstetrics & Gynecology]
Improving medication safety. Committee Opinion No. 531. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:406-10. [PubMed] [Obstetrics & Gynecology]
Shekelle PG, Wachter RM, Pronovost PJ. Making health care safer II: an updated critical analysis of the evidence for patient safety practices. Evidence report/tech- nology assessment; number 211 AHRQ publication; no. 13-E001-EF. Rockville (MD): Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services; 2013.
Sheridan SL, Harris RP, Woolf SH. Shared decision-making about screening and chemoprevention. a suggested approach from the U.S. Preventive Services Task Force. Shared Decision-Making Workgroup of the U.S. Preventive Services Task Force. Am J Prev Med 2004;26:56-66. [PubMed] [Full Text]
The Joint Commission. Comprehensive accreditation manual for hospitals: CAMH. Oakbrook Terrace (IL): The Commission; 2014.
The Joint Commission. Introduction to the universal protocol for preventing wrong site, wrong procedure, and wrong person surgery. Comprehensive accreditation manual for hospitals: CAMH. Oakbrook Terrace (IL): The Commission; 2014. p. NPSG-18-NPSG-24.
Weinstein RA. Nosocomial infection update. Emerg Infect Dis 1998;4:416-20. [PubMed] [Full Text]
Resources
Agency for Healthcare Research and Quality. Health literacy universal precautions toolkit. AHRQ Publication No. 10-0046-EF. Rockville (MD): AHRQ; 2010. Available at: http://www.ahrq.gov/professionals/quality-patient-safety/quality- resources/tools/literacy-toolkit/healthliteracytoolkit.pdf. Retrieved July 10, 2013.
Agency for Healthcare Research and Quality. Medications at transitions and clinical handoffs (MATCH) toolkit for medication reconciliation. Rockville (MD): AHRQ; 2012. Available at: http://www.ahrq.gov/professionals/quality-patient-safety/ patient-safety-resources/resources/match/match.pdf. Retrieved September 26, 2013. American College of Obstetricians and Gynecologists. Report of the presidential task force on patient safety in the office setting: appendix G. Quality and safety in women's health care. 2nd ed. Washington, DC: American College of Obstetricians and Gynecologists; 2010. p. 91-108.
Boyce JM, Pittet D. Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society
Patient Safety 77 for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. MMWR Recomm Rep 2002;51(RR-16):1-45, quiz CE1-4. [PubMed] Institute of Medicine (US). Crossing the quality chasm: a new health system for the 21st century. Washington, D.C.: National Academy Press; 2001.
The Joint Commission. Facts about the official “Do Not Use” List. Oakbrook Terrace (IL): Joint Commission; 2013. Available at: http://www.jointcommission.org/ assets/1/18/Do_Not_Use_List.pdf. Retrieved July 10, 2013.
World Health Organization. Surgical safety checklist. Geneva: WHO; 2009. Available at: http://whqlibdoc.who.int/publications/2009/9789241598590_eng_ Checklist.pdf. Retrieved July 10, 2013. Copyright WHO, 2009.