I QUALITY IMPROVEMENT ^s
Many organizations, including the American College of Obstetricians and Gynecologists and The Joint Commission, have promoted quality improvement in hospitals and other health care organizations for many years.
Quality improvement starts from the premise that although most medical care is good, it always can be better. As shown in Figure 1-1, the goal is to reduce unwarranted variation in care and improve performance. Quality improvement accepts that good care depends on more than just the judgment of the individual.In its report, “Crossing the Quality Chasm,” the Institute of Medicine set forth a list of performance characteristics that, if addressed and improved, would lead to better health and function for the people of the United States. There are six specific qualities of good care, which can be helpful in designing a quality improvement program:
1. Safe—avoids injuries to patients from care that is intended to help them
2. Effective—provides services based on scientific knowledge to all who could benefit and refrains from providing services to individuals not likely to benefit (avoiding underuse and overuse)
3. Patient centered—provides care that is respectful of and responsive to individual patient preferences, needs, and values, and ensures that patient values guide all clinical decisions
4. Timely—reduces waiting times and sometimes harmful delays for those who receive and those who give care
5. Efficient—avoids waste, in particular waste of equipment, supplies, ideas, and energy
6. Equitable—provides care that does not vary in quality because of personal characteristics, such as gender, ethnicity, geographic location, and socioeconomic status
B. Continuous improvement: Reduce variation, improve global performance (eg, evidence-based clinical guidelines)
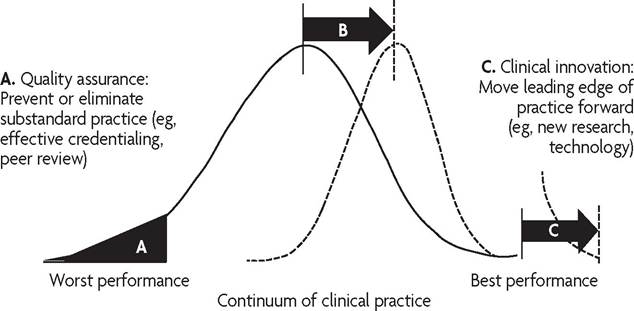
Fig.
1-1. Approaches to quality: clinical improvement strategies. (Reprinted with permission from ProMedica.) ^Quality care focuses on the following aspects of care: structure, process, and outcomes. To provide the structure, there must be adequate space, equipment, and staffing. The process refers to the use of these resources, policies and procedures, the provision of medical care, data collection, and continuous chart and record review. Finally, even with adequate structures and an efficient process, quality care requires that the desired outcomes be achieved. Any or all of these three components—structure, process, or outcome, with an emphasis on patient safety—may be the focus of a quality improvement program.
Quality Improvement in the Inpatient Setting
An institutional quality improvement program evaluates the systems, processes, and outcomes of care, including those that are not under the direct control of health care providers. Because the process is meant to be continuous, there must be a way to assess the effectiveness of changes that are made. These findings can be a major mechanism for future quality improvement.
Quality measurement should determine whether the care provided to a single patient or population of patients achieved good outcomes (outcomes measurement) or represented those processes that are thought or known to be associated with achievement of good outcomes (process measurement). All physicians have the professional and ethical responsibility to participate in quality improvement, peer review, and proctoring activities appropriate to their skills and qualifications. Their active roles in the quality improvement process can be rotated to distribute the burden of uncompensated time and effort. Hospitals or outpatient practices may choose to offer incentives to physicians who actively volunteer to take part in this process as long as it does not create a conflict of interest for participating physicians.
Leadership
A quality improvement program requires both openness to feedback and a willingness to change existing practices.
Because of this characteristic, a quality improvement program requires effective, responsive leadership in the department of obstetrics and gynecology, with support from the chief executive officer, the medical executive committee, and the governing board. The establishment of effective leadership is essential in developing a quality improvement program. The head of the department is responsible for overseeing quality improvement activities. In some cases, heads of departments or chief medical officers also may delegate specific quality improvement responsibilities to other physicians, such as patient safety officers, peer review committee chairs, or physician champions. When physicians accept leadership positions, such as a chief medical officer, chief of staff, or department chair, one of their primary responsibilities is to establish an environment in which quality improvements can thrive. As a corollary to the physician’s time commitment, the hospital should consider providing a stipend for these leadership positions.Quality Improvement Committee
The quality improvement process should be multidisciplinary in nature and involve participation of all practitioners who provide care at the hospital, group, and private practice levels. A departmental quality improvement committee may include the following members, with consideration given to the vice chair of the department serving as the committee chair:
• Representative physicians with varying levels of clinical experience (junior and senior staff) within the department
• Representative licensed independent practitioners, physician assistants, and other health care providers
• A house staff member, when appropriate
• The department head (ex officio)
Participants in case reviews must be sensitive to potential conflicts of interest and scrupulously adhere to a consistent and unbiased process. When appropriate, physicians (including those from other specialties), physician assistants, certified nurse-midwives, nurse practitioners, registered nurses, pharmacists, hospital administrative and quality control personnel, social workers, or other health care providers may need to form a multidisciplinary task force to address specific issues identified during the quality improvement review process.
These individuals also may be invited to the regular quality improvement committee meetings, as appropriate. At all times, confidentiality must be maintained. Minutes of previous meetings in which peer review activities are documented should be circulated only during the meetings themselves. Cases should be referenced by patient number to preserve confidentiality in accordance with the Health Insurance Portability and Accountability Act regulations.The rules and regulations of the department should outline the responsibilities of the quality improvement committee and provide information on committee size, composition of membership, term of office, and method of appointment. Meeting guidelines also should be established. Part of the role of this committee and the department head is to create an atmosphere whereby clinicians and other members of the department are able to raise quality issues in a confidential manner. Committee meetings should be scheduled at regular intervals, often monthly, to allow sufficient time for concurrent and retrospective case analysis.
Department Meetings and Communication
Regular departmental meetings can be used to educate practitioners about improvement of quality of care. These meetings can be a good forum to discuss the importance of documentation; errors in documentation, such as failure to include a treatment plan or failure to sign and date all notes in the record; and making corrections in the record. Regular meetings of the department also can be used to address specific clinical issues. Some of the typical formats for discussing these topics include the following:
• Presentations by a team member of problem cases or near misses, including a discussion of the issues and a review of the literature and the methods that have been used by others to resolve the problems
• Presentations by outside guest experts
• Discussion of which practice guidelines can and should be incorporated into the department and how to implement those changes.
This method of teaching reinforces the need to improve processes at a departmental level rather than addressing problems on an individual basis.• Presentations that review complicated cases or difficult situations that were handled appropriately. These cases serve to identify which methods and treatments work well and can be used as the basis for protocols and improvement of care.
• Use of variances identified through the ongoing quality improvement process to determine topics for continuing education programs, such as grand rounds and morbidity and mortality conferences
Meetings can be organized into distinct sessions. Quality improvement can be discussed with a broader committee audience to allow for more collaborative exploration of processes. Case review can be attended by a more limited membership that will promote a more thorough and confidential discussion of the items presented.
Feedback is an essential part of quality improvement. Periodic presentation of morbidity and other departmental statistics helps department members see how they, as a department and individually, are doing. Staff members thus can understand the importance of what they are doing and how the changes they have instituted have had an effect on quality of care.
Staff also can be informed about changes and new protocols through staff letters or departmental e-mails. Reminders about quality of care, trends in the department, and the need for documentation can be included regularly. Electronic communications can be used to reinforce education and teaching. This technology allows new information to be disseminated more rapidly and efficiently. The staff can be informed quickly about a newly identified problem, the recall of drugs, or defective instruments. The medical staff office should maintain a database that includes contact information, and the contact information should be regularly verified and updated to ensure that physicians and other practitioners receive information that needs to be communicated and disseminated.
Reducing Variation
Experts suggest that substantial improvements in quality can be achieved by eliminating unnecessary variation in treatment plans. This standardization can be accomplished by drafting a protocol or algorithm or by using an existing protocol to address the issue. The department may choose to apply or develop clinical pathways or protocols for high-volume, resourceintensive, or costly procedures. Protocols may take the form of a multidisciplinary plan of care or a simple decision tree. As appropriate, national evidence-based guidelines should provide the basis for the development of clinical protocols. Deviations from the finalized protocol may occur, but documentation should reflect an awareness of the protocol and include the rationale for not following the standard procedure. All disciplines involved in providing care under a protocol should be involved in the design and implementation of the protocol.
Quality Measurement
Quality improvement programs must focus on measurable dimensions of care to identify areas in need of improvement and should evaluate the department as a whole, as well as individual physicians. A department should consider the dimensions of care when selecting indicators to track (see Box 1-4). Cases identified by one of these indicators may not necessarily indicate substandard care but do require careful review by physicians. Quality measurement should determine whether the care provided to a single patient or population of patients achieved good outcomes (outcomes measurement) or represented those processes that are thought or known to be associated with achievement of good outcomes (process measurement).
Box 1-4. Examples of Gynecologic Clinical Quality Indicators ^
• Unplanned readmission within 14 days
• Admission after a return visit to the emergency department for the same problem
• Cardiopulmonary arrest, resuscitated
• Infection that was not present on admission
• Unplanned admission to special (intensive) care unit
• Unplanned return to the operating room for surgery during the same admission
• Ambulatory surgery patient admitted or retained for complication of surgery or anesthesia
• Failure to administer appropriate deep vein thrombosis prophylaxis for gynecologic surgery
• Gynecologic surgery, except radical hysterectomy, cytoreductive surgery, or exenteration, using 2 or more units of blood, or postoperative hematocrit of less than 24% or hemoglobin of less than 8 g
• Wrong site, wrong patient, or wrong surgical procedure
• Unplanned removal, injury, or repair of organ during operative procedure
• Initiation of antibiotics more than 24 hours after surgery
• Discrepancy between preoperative diagnosis and postoperative tissue report
• Removal of uterus that weighs less than 280 g for leiomyomas
• Removal of follicular cyst or corpus luteum of ovary
• Hysterectomy performed on women younger than 30 years except for malignancy
• Prolonged hospitalization (more than two standard deviations from the mean stay for that diagnosis)
• Unanticipated death
Modified from American College of Obstetricians and Gynecologists. Quality and safety in women's health care. 2nd ed. Washington, DC: American College of Obstetricians and Gynecologists; 2010. p.17.
The methods used to determine quality or efficiency of care are called by many different names, such as rates, instruments, elements, standards, indicators, or measures. Although differences in definitions are nuanced depending on the audience, for this section, they will simply be referred to as indicators or measures.
Quality Indicators
The primary purpose of quality indicators is to stimulate discussion (and action if needed) around improving the care of and services for patients. Quality indicators are defined as follows[*]:
...specific and measurable elements of practice that can be used to assess the quality of care. They are usually derived from retrospective reviews of medical records or administrative claims and enrollment data. Measures are also being incorporated into and between electronic health records and data registries. Some authorities differentiate “quality” from “activity” or “performance” indicators. The important issue is that a good quality indicator should define care that is attributable and within the control of the person who is delivering the care.
It is important to note that indicators are not direct measures of quality; quality is multi-dimensional, and many different measurements must be made before it can be fully assessed. Quality indicators are best used as a means of improving a system of care, not judging performance or being used solely as a management tool.
Quality indicators may focus on structural elements, process components, or outcomes in the health care system or setting under study. Except for the most common outcomes, there are multiple technical and practical difficulties in assessing outcomes. As a result, quality is most often measured in the form of process indicators. It is important to note, however, that process indicators do not signify quality until their relationship to the desirable outcome is validated. Process indicators are particularly helpful when quality improvement is the goal of the assessment process, when short time frames for measurement are needed, or when tools to adjust or stratify for patient factors are not available.
Evidence-based clinical indicators can be developed by following a six- step system:
1. Identify the outcome of interest.
2. Form a measurement team to provide an overview of existing evidence and practice.
3. Choose quality indicator(s) on the basis of research evidence.
4. Determine the standard of quality being sought.
5. Design a reliable and valid system of measurements that can be applied consistently.
6. Conduct preliminary testing for reliability and validity.
Several sources of benchmarks of quality indicators are available for individual health care providers or practices, such as Healthy People 2020, National Committee for Quality Assurance Healthcare Effectiveness Data and Information Set (also known as HEDIS) data, and the Agency for Healthcare Research and Quality National Healthcare Quality Report (see Resources).
Indicators may be monitors of sentinel events, such as retained foreign objects; if so, every case should be reviewed frequently on an expedited basis. Indicators may monitor specific rates, such as with excess blood loss. If the frequency of a rate-based indicator exceeds the departmental threshold or there are changes in frequency over time, an in-depth review may be needed. Indicators may be positive and desirable, such as detection and treatment of chlamydial infection, or negative, such as an unplanned return to the operating room.
Indicators should be clearly and specifically defined so that they can be benchmarked and the results can be compared with regional or national norms. Risk-adjustment methods (eg, body mass index, comorbidities, diabetes, and hypertension) should be used when possible. Deviations from the norm can then be readily identified. Physician profiles also may be developed so that an individual’s practice pattern for each indicator can be compared with department and national or regional benchmarks. Such profiles will form part of the database used to make decisions on granting
or renewing clinical privileges and can be used to show improvement over time. Deviations from the norm do not necessarily indicate inappropriate care. Use of a clinical indicator may flag cases managed by a particular physician that, when peer reviewed, appear to show plausible reasons for the variations. However, continued monitoring over time (referred to as trending) may demonstrate that this physician has a much higher rate of variation than the department as a whole. Therefore, trending data may suggest a problem, such as surgical technique, that an individual case review does not identify.
Institutions may wish to define acceptable levels of care (ie, thresholds) for different indicators. A threshold is a data point that, when reached or crossed, signals an outlier that needs further investigation and evaluation. Using thresholds is a method for deciding when an issue should be addressed and where first to look for possible problems without requiring peer review of all records. The threshold level chosen as the standard for the institution should be supported by the best available clinical and quality improvement literature. Information on local and national rates of complications may be obtained from the respective state health data organization, the National Center for Health Statistics, or the Agency for Healthcare Research and Quality. Hospital departments also may participate in data registries, such as the National Surgical Quality Improvement Programs through the American College of Surgeons or the U.S. Department of Veterans Affairs, for risk-adjusted benchmarks. Thresholds may need to be changed as new technology evolves and treatments improve.
Performance Measures
Performance measures are designed to guide physicians in their evaluation, reporting, and delivery of quality care to patients. Although they may measure different components of quality, they should ultimately be linked in a meaningful way to outcomes. Currently, the major obstacle to improving the quality of health care in the United States is the lack of a coherent and consistent system for assessing and reporting on the performance of the health care system. Regardless, stakeholders want more information about how the health care system is performing, and they want to know that health care delivery actually is improving health outcomes. The Institute of Medicine report on performance measures, payment, and performance improvement noted that current performance measurement systems are limited because it is not always clear that the criteria being measured are truly or solely responsible for improvements that may be seen (see Bibliography). Types of Performance Measures. Performance measures include measures of the health care process (eg, hemoglobin A1C testing for patients with diabetes), health outcomes (eg, surgical-site infections), perceptions of care (eg, patient satisfaction with physician interactions), and organizational structure and systems (eg, electronic order entry). Standardized performance measures have detailed specifications; they may require risk adjustment or stratification of results across key subgroups. A key element of any performance measurement system is ensuring that data for performance measures are reported accurately.
Performance measures should be designed to be used as a guide by physicians in their evaluation, reporting, and delivery of quality care to patients. They should be linked in a meaningful way to outcomes, but they do not necessarily have to measure outcomes. Performance measures and process measures may have some fundamental advantages over outcomes measures:
• Reduce case mix bias—Performance measures use opportunity for error rather than the number of patients treated as the denominator.
• Avoid stigma—Performance measures are more likely to be perceived as suggestions for improvement, rather than criticisms of performance.
• Prompt wider action—Process measures encourage action at every level of the organization, not just by a few individuals or the outliers.
• Evaluate delayed events—Process measures are more useful for evaluating events that may take longer to appear.
Process measurements can be precisely defined and are often very specific; hence, they are not usually subject to risk adjustment. They are ideal measures to include as performance measures, but only if there is an evidence-based link to quality improvement. It is not practical to set the threshold for measurement at 100%—too many exclusion criteria would need to be incorporated and result in increased data burdens on health care providers—but levels may be based on aggregate national data.
Data for Performance Measurement. There are three main sources of data for performance measurements: 1) administrative claims and enrollment data, 2) medical records (paper and electronic) and registries, and 3) surveys. Administrative claims systems are not designed to be specific and reliable tools for quality measurement and reporting. Paper medical record abstraction of data is time consuming and expensive, and electronic medical records are in their infancy in regards to interoperability, standardization, and use. Surveys of patient perception of patient care are attributed to a specific practice because either the patient identified one of the health care providers as her primary care provider or computerized algorithms based on claims designate a practitioner as the primary care provider. All of these approaches are subject to error.
Quality Measurement Tools
A quality improvement program also requires tools to assess and determine overall performance. Failure mode and effects analysis and root cause analysis are tools that may be used in the process of setting up systems or procedures in order to evaluate these systems for possible errors. They also may be used for continued surveillance of ongoing systems and procedures to effect change and corrective actions designed to make them safer.
Failure Mode and Effects Analysis
Failure mode and effects analysis is a prospective risk assessment tool that is used to analyze proposed systems, production lines, or processes for possible unanticipated faults, defects, and errors. This tool generally is used during the planning or organizing process for these systems or procedures. The potential errors or faults are identified and rated by levels of severity or potential harm that they may cause. This tool also assesses the effect of these errors on the system or procedure that is being considered.
Failure mode and effects analysis initially was used by the military and in aerospace development. It is widely used in manufacturing industries in various phases of production. Medical device and drug delivery systems have added failure mode and effects analysis procedures as a means to understand the potential risks and defects that may not be considered by individual designers. Failure mode and effects analysis is now increasingly finding use in the service industry, and hospitals also have begun to use this technique to prevent the possibility of process errors and mistakes, which lead to incorrect surgery or medication administration. This use is driven by The Joint Commission.
Failure mode and effects analysis allows a team of individuals to review the design or process at key points in its development and make comments and changes to the design of the system or process well in advance of actually experiencing the failure. The U.S. Food and Drug Administration has recognized failure mode and effects analysis as a design verification method for drugs and medical devices.
In a failure mode and effects analysis, failures and errors are prioritized according to how serious their consequences are, how frequently they occur, and how easily they can be detected. This analysis also documents and updates current knowledge about the process being monitored and is used as a tool for continuous improvement. Failure mode and effects analysis begins during the earliest conceptual stages of design of a process or system and then continues throughout the life of that system. It is used during the design stage with an aim to avoid future potential or actual complications and errors. Later it is used for monitoring and modification before and during ongoing operation of the process.
The Department of Veterans Affairs National Center for Patient Safety developed a hybrid prospective risk analysis system, Healthcare Failure Mode and Effect Analysis, which includes a five-step process that uses an interdisciplinary team to proactively evaluate a health care process. The team uses process flow diagramming, a Hazard Scoring Matrix, and the Healthcare Failure Mode and Effect Analysis Decision Tree to identify and assess potential vulnerabilities. Information on this system is publicly available through the National Center for Patient Safety (see www.patient safety.va.gov/).
Root Cause Analysis
Root cause analysis is a group of problem-solving methods aimed at identifying the underlying causes of problems or events. The theory of root cause analysis is that problems are best solved by correcting or eliminating root (underlying) causes of the problem and not merely addressing the obvious symptoms. Root cause analysis is a tool used to identify process and system failures that result in sentinel events, medical error, or near misses. A root cause analysis should identify the reason for the presence of a defect or problem that, if eliminated, would prevent recurrence. There is recognition that complete prevention of recurrence of an error by a single intervention is not always possible, and as a result, a root cause analysis often is considered to be an iterative process and viewed as a tool of continuous improvement.
There are several general principles that apply to a root cause analysis. The process is a retrospective tool that is applied systematically. It is also an interdisciplinary tool and is performed with the ultimate goal of concentrating on the systems and processes rather than the performance of individuals. It is a learning tool that is used to promote teamwork, facilitate open communication, prevent similar errors in the future, and enhance patient safety and quality of care. Relevant data and literature must be used in drawing conclusions that are evidence based. There is frequently more than one root cause for any given problem. This tool looks into determining human factors as well as related processes and systems.
Performing a root cause analysis often is triggered as a requirement of The Joint Commission. The Joint Commission requires that specific sentinel events that trigger a root cause analysis include an evaluation of very specific processes as part of the root cause analysis. In addition to The Joint Commission, there may be other state and local regulatory agencies that could require a root cause analysis in response to a medical error or some other poor outcome. In some cases, a professional liability carrier might require a root cause analysis as a result of a poor patient outcome that could potentially increase a liability exposure for the carrier and its clients. Hospitals should incorporate the root cause analysis and its resultant monitoring into the ongoing quality improvement process.
Data Collection and Analysis
The quality improvement process requires accurate collection and analysis of meaningful data. Data collection is important not only to formulate the problem statement, but also to support the team’s belief that a planned change will result in improvement. Initial data collection is key for problem identification. Data also are critical for demonstrating that changes will result in system improvement. This is particularly helpful because not all change results in improvement. It may not be necessary to collect volumes of data before effecting change. For example, sampling can be used to demonstrate the change being tested. Another suggestion is to use both qualitative and quantitative data. Process and outcome measures also may be used to help determine whether a change has led to improvement.
Historically, data have been collected by retrospective chart review. Quality improvement ideally includes concurrent data collection as well. Clinical indicators should guide the abstraction of data by trained individuals. Cases identified through application of the indicators should be reviewed by physicians with judgment and experience in the clinical issues and the peer review process.
The data obtained by this process also can be used for educational purposes:
• To inform all staff members of the performance of the unit as a whole
• To inform individual clinicians how their care compares with that of their peers
• To update staff about current techniques to improve outcomes
The ultimate objective is to encourage behavioral changes, system changes, or both to reduce unwarranted variation and improve patient safety. Results may be shared through departmental meetings, quarterly summaries of trends, and letters directed at the medical staff. Continuing medical education should focus on correcting deficiencies in knowledge or unexplained variations in care identified through the quality improvement process.
Although screening medical records for indicators can aid in identifying practice variations that might indicate the need for further review, documentation, or justification, more often than not, cases that are identified through this process have no quality of care issues. Peer review can determine whether such variations are appropriate. Therefore, identified cases should be reviewed by physicians with the knowledge, experience, and judgment to assess the clinical appropriateness of practice variations.
Peer Review
Small departments face a variety of challenges to conduct effective peer review because of several factors, which might include the following:
• Competitive interests
• Fear of reprisal
• Conflict of interest
• Lack of objectivity
• Personal relationships
• Lack of qualified reviewers
These factors may have a real or perceived effect on the efficacy of the review. Therefore, it may be helpful to develop a relationship with another hospital to conduct peer review. An alternative would be to use the services of an outside, independent reviewer. In either case, it is important to remember that responsibility for peer review and quality improvement rests with the hospital medical staff and, ultimately, the governing board.
Departments of any size may face these challenges and consider developing a relationship with another hospital or an outside peer review organization. A specialty-specific program that can assist with issues related to quality assessment and peer review is the Voluntary Review of Quality of Care Program of the American Congress of Obstetricians and Gynecologists (see Box 1-5).
Both federal and state laws provide some protection for physician peer review. The Health Care Quality Improvement Act, passed by the U.S. Congress in October 1986, grants immunity from damages under federal and state laws (including antitrust provisions) to health care providers engaged in good faith peer review. Most states also have adopted laws to encourage and protect physician peer review, although the type of immunity offered and the class of individuals protected from personal liability for participating in peer review vary from state to state.
Most states safeguard the confidentiality of records used in peer review actions. Again, the extent of the protection varies from jurisdiction to jurisdiction, and anyone engaged in peer review should know the laws of his or her state. For example, some states recognize confidentiality only for the
Box 1-5. Voluntary Review of Quality of Care ^
The Voluntary Review of Quality of Care (VRQC) program of the American Congress of Obstetricians and Gynecologists is available to assist hospitals and physicians in assessing the quality of care provided in their departments of obstetrics and gynecology as well as the quality improvement process within the department. The VRQC peer review teams consist of five reviewers: three obstetrician-gynecologists, one nurse, and one medical writer. When requested, these review teams also can include individuals with expertise in midwifery, anesthesiology, and family medicine. The reviews are conducted over 4 days and include one-on-one interviews, chart reviews, an introductory entrance conference as well as an exit conference, and a detailed report that includes an analysis of data submitted by the hospital, the VRQC review team's findings, and recommendations for improvement based on the American Congress of Obstetricians and Gynecologists' guidelines.
For more information about the VRQC Program, send an email to vrqc@acog. org, call (800) 266-8043, or visit www.acog.org/goto/vrqc.
American Congress of Obstetricians and Gynecologists. VRQC program overview. Available at: http://www.acog.org/About_ACOG/ACOG_Departments/VRQC_ and_SCOPE/VRQC_Program_Overview. Retrieved July 10, 2013.
peer review records of a hospital review committee, whereas others protect all information reported to the committee. In some states, the information is not admissible as evidence in a trial but may be discoverable in pretrial proceedings. To ensure the maximum protection of records, individuals formulating a hospital’s quality review program should seek legal advice.
Correcting a Deficiency
When a quality improvement process identifies deficiencies in the quality of care provided by a specific individual, the department head or other responsible person has the responsibility, and should have the authority, to take steps to correct the deficiency. The identification of the problem, how it was addressed, and what action was instituted should be documented. This documentation should include a statement of the expectations for change, the means by which change will be measured, and if appropriate, a time line. Most opportunities for improvement can be handled under the authority of the department head or other responsible person. When the recommended action requires the involvement of the appropriate institutional governing board, established procedures should facilitate necessary decision making. When the action required involves a reduction or revocation of privileges, it is critical to have legal consultation to ensure that the process is handled appropriately.
Timely discussion and counseling with the practitioner always should be the first step in the process. In certain circumstances it may be all that is required. The following are other possible actions that may be instituted:
• Observation of the practitioner’s skills. Observation is either by the department head or by a designated staff member who may have the skills required to assess a particular procedure or treatment.
• Trending. Continued monitoring over time can determine whether the physician has a much higher rate of variation than the department as a whole. Trending data may identify a problem, such as surgical technique, that an individual case review does not identify.
• Remedial education. This education may take the form of special programs focused on need. Remedial education may be necessary because of an identified deficiency in care, in which case a remedial program for the individual may be provided or obtained elsewhere. When a deficiency involves several staff members, it is more appropriate to direct the education toward the unit as a whole. This process, along with resulting findings, should be reported to the institutional quality improvement committee.
• Proctoring. Proctoring requires the direct observation of an individual’s practice by a peer or a chart review of current or recently treated patients to ensure that the deficiencies are being corrected.
• External peer review. This action may be used when there is interpersonal conflict, disagreement as to the appropriate action, or a lack of comparable skill within the department.
When the quality improvement process or other mechanisms have identified unwarranted variation, a specific problem, an opportunity to improve care, concerns about patient safety, or individual performance problems, a plan should be formulated. When data gathered suggest that change will lead to improvement, the changes then can be implemented in a systemwide manner.
When the deficiency is considered more serious, privileges may be reduced. Reducing privileges requires formal proceedings, which should be prescribed in the medical staff bylaws and may be subject to reporting to the National Practitioner Data Bank (see also the “Evaluating Credentials and Granting Privileges” section earlier in Part 1).
Quality Improvement in the Office
The medical office or clinic is well suited to modern methods of quality improvement, and programs and resources that address quality improvement in the office continue to evolve. Ideally, a written quality management plan should be established. In the outpatient setting, whether in a solo office practice or a multispecialty ambulatory surgery center, a physician should be designated as the chief medical officer to be responsible for the patient safety and quality improvement initiatives. As with hospitals, outpatient settings should consider providing a stipend for these leadership positions. The office staff (including clinicians and administrative staff) should meet periodically as a team to discuss methods of measuring and improving the quality of the care administered by the office. Larger practices may want to designate an interdisciplinary quality management team.
Each office should establish a simple, reliable tracking and reminder system to improve patient safety and quality of care and to minimize missed diagnoses. The use of an electronic health record may be used as a realtime, evidence-based support tool that can help obstetrician-gynecologists improve the quality of care they provide through improved care coordination, communication, and documentation.
The office can develop specific indicators to evaluate one or more systems (see Box 1-6). Quality management activities within the medical office may concentrate on assessing and improving function in one specific system at a time. Once that function has improved to a level of quality acceptable to the practice, the quality management team can move to another system for review. Several systems may be monitored optimally by regular tracking (eg, patient complaints or complications of office procedures). Medical practices also may wish to evaluate the quality of care
Box 1-6. Examples of Systems to Monitor for Quality Improvement in the Office ^
Medical Records and Information Systems
• Legibility
• Organization
• Documentation—general (including problem list)
• Lost medical records
• Misfiled medical records
• Breach of confidentiality
• List of current medications
• Health Insurance Portability and Accountability Act compliance
Appointments and Scheduling—Patient Flow
• Acceptable waiting time for appointments
• Appropriate waiting time in office to see clinician
Billing
• Precertification
• Timeliness
• Accurate coding
Patient Communications
• Method of informing patients of a delayed or rescheduled appointment
• Monitoring of appropriateness of method of terminating patientpractitioner relationship
Telephone Communications
• Excessive busy signals (data are available from telephone company)
• Excessive holding time
• Documentation of telephone contact in medical records, with disposition documented
• Monitoring of telephone prescription refills for doctor approval
• Monitoring of “dropped” or lost calls
(continued)
Box 1-6. Examples of Systems to Monitor for Quality Improvement in the Office (continued)
Personnel Management
• Employee morale
• Absenteeism
• Periodic employee performance assessment
• Maintenance of patient confidentiality
Equipment and Drugs
• Periodic equipment check for proper function
• Maintenance logs of equipment repair
• Security system for controlled drugs
• Security system for syringes and needles
• Method of monitoring drugs for expiration dates (including samples)
Patient Safety and Medical Error Reduction
• Tracking systems for laboratory, radiology, and cytology results
• Safe medication use
• Wound infections
• Delayed complications from hospitalized patients
• Equipment failure
administered by their practitioners in the hospital setting separate from the hospital’s quality management program. These issues may include continuity of care, consistency of care, cross-coverage, and communication.
Efforts made to improve quality and patient safety also will have positive effects on risk reduction; therefore, the two programs may be carried out in tandem. An example of a program that can assist with issues related to quality assessment and peer review in the outpatient setting is the Safety Certification in Outpatient Practice Excellence program of the American Congress of Obstetricians and Gynecologists (Box 1-7). Professional liability carriers also may have useful tools for improving quality and patient safety.
Box 1-7. Safety Certification in Outpatient Practice Excellence ^
The Safety Certification in Outpatient Practice Excellence (SCOPE) for Women's Health program of the American Congress of Obstetricians and Gynecologists is a voluntary, comprehensive, patient safety review program available to medical practices in which obstetric services, gynecologic services, or both are provided. Through the two-step application and site-review process, the SCOPE for Women's Health program assesses the implementation and use of patient safety concepts and techniques in an individual office setting. For more information about the SCOPE for Women's Health program, send an e-mail to scope@acog.org, call (800) 266-8043, or visit www.scopeforwomenshealth.org. American Congress of Obstetricians and Gynecologists. Safety Certification in Outpatient Practice Excellence (SCOPE). Available at: http://www.scopeforwomens health.org. Retrieved July 10, 2013.
There are a number of challenges to developing a performance measurement framework for physician practices. Listed are questions to consider at the beginning of the development process:
• What will be the specific purposes of the measurement system?
• How should the specific aspects of performance (for which individual physicians or physician organizations will be held accountable) be measured?
• What specific information should be part of the performance measurement system and included in the reporting system? What are the optimal formats for disseminating performance information?
• How will performance measures for physicians or physician practices be implemented in an ongoing and feasibly sustainable way? Who will bear the costs?
Meaningful reporting at the practice level is a challenge. For example, the challenges for measuring performance in small practices include lack of infrastructure, lack of health information technology, lack of support staff, and increased burden of data collection. A 2003 survey found that less than 24% of physicians were able to compare their performance with their peers either within their specialty or within health plans. Only 11% were able to meet the benchmark of physicians nationally.
Public and private payor data must be pooled to yield meaningful information for small practice settings. Individual insurers do not account for a large enough share of a practice’s population to provide meaningful measures of performance. Some aspects of practice performance are quite difficult to assess; this is particularly true if a practitioner sees a low volume of patients, in which case there will not be enough data to provide meaningful or valid assessments of performance. When sample sizes are small, there are problems with risk adjustment and bias, and although these issues may be dealt with, there is currently no mechanism for pooling data across purchasers. Whereas all health care providers involved in the care of a patient share in the responsibility for providing quality care, designing measurement systems that accurately reflect the degree of influence and responsibility of each practitioner is problematic at best.
Bibliography
Berwick DM. Continuous improvement as an ideal in health care. N Engl J Med 1989;320:53-6. [PubMed]
DeRosier J, Stalhandske E, Bagian JP, Nudell T. Using health care Failure Mode and Effect Analysis: the VA National Center for Patient Safety’s prospective risk analysis system. Jt Comm J Qual Improv 2002;28:248-67. [PubMed]
Institute of Medicine (U.S.). Health literacy: a prescription to end confusion. Washington, D.C.: The National Academies Press; 2004.
Institute of Medicine (U.S.). Performance measurement: accelerating improvement. Washington, D.C.: National Academies Press; 2006.
Institute of Medicine (U.S.). Priority areas for national action: transforming health care quality. Washington, D.C.: National Academies Press; 2003.
Institute of Medicine (U.S.). Crossing the quality chasm: a new health system for the 21st century. Washington, D.C.: National Academy Press; 2001.
Kongnyuy EJ, Uthman OA. Use of criterion-based clinical audit to improve the quality of obstetric care: A systematic review. Acta Obstet Gynecol Scand 2009;88: 873-81. [PubMed] [Full Text]
Marshall M, Campbell S, Hacker J, Roland M, editors. Quality indicators for general practice: a practical guide for health professionals and managers. London (UK): Royal Society of Medicine Press; 2002.
Patient safety and the electronic health record. Committee Opinion No. 472. American College of Obstetricians and Gynecologists. Obstet Gynecol 2010; 116:1245-7. [PubMed] [Obstetrics & Gynecology]
Standardization of practice to improve outcomes. Committee Opinion No. 526. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;119:1081-2. [PubMed] [Obstetrics & Gynecology]
Tracking and reminder systems. Committee Opinion No. 546. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:1535-7. [PubMed] [Obstetrics & Gynecology]
Resources
ABIM Foundation. Choosing Wisely: Five things physicians and patients should question. Available at: http://www.choosingwisely.org/doctor-patient-lists. Retrieved July 10, 2013.
Agency for Healthcare Research and Quality. National healthcare quality and disparities reports. Available at: http://www.ahrq.gov/research/findings/nhqrdr/index. html. Retrieved July 10, 2013.
American College of Obstetricians and Gynecologists. Quality and safety in women’s health care. 2nd ed. Washington, DC: American College of Obstetricians and Gynecologists; 2010.
Audet AJ, Doty MM, Shamasdin J, Schoenbaum SC. Physicians’ views on quality of care: findings from the Commonwealth Fund National Survey of Physicians and Quality of Care. New York (NY): The Commonwealth Fund; 2005. Available at: http://www.commonwealthfund.org/Publications/Fund-Reports/2005/May/ Physicians-Views-on-Quality-of-Care--Findings-From-The-Commonwealth-Fund- National-Survey-of-Physicia.aspx. Retrieved July 10, 2013.
Department of Health and Human Services. Healthy People 2020. Available at: http://www.healthypeople.gov/2020/default.aspx. Retrieved July 10, 2013.
National Committee for Quality Assurance. HEDIS and performance measurement. Available at: http://www.ncqa.org/tabid/59/Default.aspx. Retrieved July 10, 2013.
More on the topic I QUALITY IMPROVEMENT ^s:
- SOME CONCLUSIONS ON OPPORTUNITIES AND CHALLENGES WITH A POLICY VIEW
- REVIEW OF FORENSIC ASSESSMENT INSTRUMENTS