I PEDIATRIC GYNECOLOGY ^228 ^436 ^573
Pediatric gynecology includes the care of prepubertal and peripubertal girls. A small percentage of this group will come to the attention of the obstetrician-gynecologist. The most common presenting problem is vulvovaginitis.
Other problems include labial adhesions and labial agglutination, prepubertal bleeding (usually not caused by precocious puberty), and sexual abuse.The Pediatric Gynecologic Examination
Pediatric gynecologic examinations should be conducted with patience and sensitivity by health care providers with interest and experience in this area. The examination in prepubertal girls is approached differently from that in reproductive-aged women, but it still may include examination of the vagina and internal genital organs. A speculum examination is generally not indicated during the office examination of a prepubertal girl. Forcible restraint never is indicated, and sedation rarely is necessary. The American Academy of Pediatrics recommends that, in general, the examination of a younger girl should be chaperoned by the girl’s parent or caregiver. As girls become older, their caregivers and the children themselves should participate in the decision of whether to use a chaperone. As with adults, a full explanation of the examination and the reason for it is always warranted. The American Academy of Pediatricians states that it is wise for male health care providers to have a chaperone during female genital examinations.
The clinician should be familiar with state statutes regarding the need for consent by a parent or guardian for a pediatric gynecologic examination. All states require that findings of signs of physical or sexual abuse in minors be reported to state authorities.
A girl can be positioned in a froglike or lithotomy position, depending on her age. Gentle lateral and downward traction of the labia with the examiner's fingers will allow visualization of the external genitalia, including the hymeneal tissue.
The vagina can be examined by placing the child in a knee-chest position (see Fig. 3-3). In this position, the vagina fills with air and generally can be visualized with an otoscope, which acts as a magnifying lens and light source but is not inserted into the vagina. Visualization is enhanced by lateral and superior traction of the labia majora.A gentle digital rectal examination can be performed, if necessary given the patient's symptoms. It allows for assessment of the cervix, uterus, solid foreign bodies, or other masses. Cultures of the vagina can be accomplished by using small cotton-tipped swabs moistened with nonbacteriostatic saline or by using lavage systems.
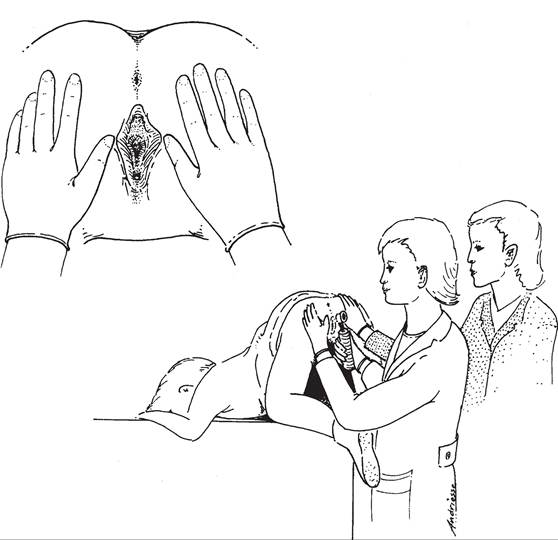
Fig. 3-3. Examination of the prepubertal child in the knee-chest position.
(Reprinted with permission from Emans SJ, Laufer MR, Goldstein DP, editors. Pediatric and adolescent gynecology. 5th ed. Philadelphia [PA]: Lippincott Williams & Wilkins; 2005. p. 13.)
Vulvovaginitis
The most common pediatric gynecologic problem an obstetriciangynecologist is likely to encounter is vulvovaginitis, an inflammatory process that involves the vulva and vagina. Symptoms involve the vulva more than the vagina—the opposite of what is typically seen in reproductive-aged females. Girls may present with a variety of symptoms, including irritation, discomfort, pruritus, dysuria, and discharge.
Vulvovaginitis can be divided into two groups based on etiology: 1) nonspecific vulvovaginitis, and 2) specific infectious vulvovaginitis. Most cases are nonspecific. Yeast is not a common cause of vulvovaginitis in this age group because the prepubertal nonglycogenated vagina is alkaline and generally does not support fungal growth.
Nonspecific Vulvovaginitis
Nonspecific vulvovaginitis is common in prepubertal girls and has been attributed to the proximity of the anus and vulva, poor hygiene, and the hypoestrogenic state.
Chemical irritants, such as soaps, laundry detergents, and chemicals associated with the use of swimming pools or hot tubs, also may play a role. Nonspecific vulvovaginitis is a diagnosis of exclusion after pathogens have been ruled out. In a child with no history of vulvovaginitis, no purulent discharge, and no historical findings suggestive of abuse, the obstetrician-gynecologist may opt to treat the patient for nonspecific vulvovaginitis, avoiding the cost of cultures. However, many pediatric patients with symptoms of vulvovaginitis who visit gynecologists have had a previous evaluation and failed treatment, and they deserve a thorough evaluation with cultures and testing, as well as consideration of the presence of a foreign body.Treatment is primarily aimed at improving perineal hygiene, such as careful wiping from front to back after bowel movements. Using sitz baths and avoiding chemical or traumatic irritation also are important. Regular bathing, as opposed to taking showers, is beneficial to perineal hygiene in prepubescent girls. Young girls also should be advised to wear cotton-only underwear and limit time spent in tights, leotards, and wet swimsuits.
Infectious Vulvovaginitis
Infectious vulvovaginitis, in which a specific pathogen is isolated as the cause of symptoms, may be caused by fecal or respiratory pathogens, such as Escherichia coli, Streptococcus pyogenes, Staphylococcus aureus, Haemophilus influenzae, and rarely Candida species. These organisms may be transmitted by the child using improper toilet hygiene and manually from the nasopharynx to the vagina. Neisseria gonorrhoeae or Chlamydia trachomatis also are causes of specific infectious vulvovaginitis, the presence of which strongly suggests sexual abuse (see “Sexual Abuse” later in this section). Trichomonas vaginalis is an uncommon cause of specific infectious vulvovaginitis in the unestrogenized prepubertal female. Other causes of infectious vulvovaginitis include Shigella species (which often presents with a blood-tinged purulent discharge) and Yersinia species of bacteria.
Pinworms are the most common helminthic infestation in the United States, with the highest rates in school-aged and preschool children. Perianal itching may lead to excoriation and, rarely, bleeding. Vulvar and perianal erythema often is present.Cultures with sensitivities to test for specific pathogens may be obtained with cotton swabs or urethral (calcium alginate tipped applicator) swabs moistened with nonbacteriostatic saline. Use of a swab can cause discomfort or, rarely, minimal bleeding. To distract the patient, the child can be asked to cough. A topical anesthetic can be applied before placing the swab into the vagina. Alternatively, a small feeding tube attached to a syringe with a small amount of saline for vaginal wash and aspiration can be used. This allows for examination of the fluid under the microscope as well as sending the fluid off for culture. A minimal amount of normal saline should be used to avoid dilution of the specimen. The CDC recommends performing a culture instead of a nucleic acid amplification test (NAAT) for the detection of C trachomatis and N gonorrhoeae in girls because data are limited on the use of NAATs in children. (For more information, see the CDC guidelines for the detection of C trachomatis and N gonorrhoeae at http://www.cdc.gov/std/.) Tests for Shigella may require special media and collection procedures. If pinworms are suspected, transparent adhesive tape or an anal swab should be applied to the anal region in the morning before defecation or bathing and then placed on a slide. Eggs seen on microscopic examination confirm the diagnosis.
The treatment of specific vulvovaginitis should be directed at the organism causing the symptoms. Treatment guidelines are available from the CDC, the North American Society for Pediatric and Adolescent Gynecology, and the American Academy of Pediatrics (see Resources).
Vulvar Disorders
Vulvar disorders in children may be infectious (eg, molluscum contagio- sum, condyloma, or herpes) or noninfectious (eg, labial agglutination, lichen sclerosus, psoriasis, atopic dermatitis, contact dermatitis, or seborrheic dermatitis).
The diagnosis and management of these disorders are discussed here.Infectious Vulvar Disorders
Molluscum contagiosum is characterized by 1-5-mm discrete, skin-colored, dome-shaped, smooth papules with a central cheesy plug, sometimes referred to as “umbilicated lesions.” The area surrounding the lesions may be erythematous or pruritic. It is common in school-aged children, especially among those who live in overcrowded areas or have poor hygiene. Secondary spread of lesions may occur by autoinoculation. Diagnosis usually is made by visual inspection. The disease generally is self-limited and the lesions may resolve spontaneously and, for this reason, treatment usually is not necessary in the young child. If treatment is indicated, however, it should not be excessive or overly aggressive. Treatment choices in children may include cryosurgery, application of topical anesthetic and curettage, and topical silver nitrate. Successful use of topical 5% imiquimod cream also has been reported and it is approved by the U.S. Food and Drug Administration for use in patients 12 years and older.
Condyloma acuminata, or warts, result from perinatal transmission of the human papillomavirus (HPV) or close sexual or nonsexual contact with an infected individual or object. Diagnosis usually is made by visual inspection. Biopsy has a limited place in management and should be reserved for those cases in which the diagnosis is in question or operative treatment is planned. Human papillomavirus DNA testing is not helpful. Nonintervention is a reasonable approach in asymptomatic children because lesions may resolve spontaneously or decrease in size over time.
A variety of treatment options are available for symptomatic children, although none are uniformly effective, and the recurrence risk is high with all modalities. Destructive and excisional options, which may require general or local anesthesia, include topical trichloroacetic acid, local cryotherapy, electrocautery, excision by scalpel or scissors, and laser ablation.
Successful use of topical 5% imiquimod cream also has been widely reported. Referral to a specialist should be considered for children in need of extensive treatment. Because condylomata acuminata frequently are sexually transmitted, the possibility of sexual abuse should be addressed (see “Sexual Abuse” later in this section).The herpes simplex virus (HSV) can spread by autoinoculation or close nonsexual or sexual contact. Beyond the neonatal period, the presence of genital HSV indicates the need for a sexual abuse evaluation. Herpes simplex virus type 1 and HSV type 2 may involve the genitalia. The condition begins as clusters of painful vesicles on an erythematous base that may be accompanied by malaise, fever, and myalgia. Rupture results in ulcerations covered with a hemorrhagic yellowish-gray crust. According to the CDC, cell culture and polymerase chain reaction are the preferred HSV tests for individuals who seek medical treatment for genital ulcers. Viral culture isolates and polymerase chain reaction samples should be typed to determine which type of HSV is causing the infection. Accurate type-specific HSV serologic assays are based on HSV-specific glycoprotein G2 (HSV-2) and glycoprotein G1 (HSV-1). Children older than 2 years may be treated with oral acyclovir. If HSV is not detected as the etiologic agent, other possible causes of genital ulcers include cytomegalovirus, Epstein-Barr virus, and Behcet disease.
Noninfectious Vulvar Disorders
Labial adhesions are not uncommon in prepubertal girls and have been noted in children as young as 3 months old. They typically resolve spontaneously by menarche. The combination of vulvar irritation and hypoestro- genic environment can lead to labial adhesions. On examination, the line of agglutination can be visualized between the two labia minora. Labial adhesions should be observed unless they are symptomatic. If the condition produces symptoms (eg, frequent urinary tract infections, dysuria, or inability to void), the usual treatment is topical estrogen cream applied twice daily for 6 weeks directly over the line of agglutination. The caregiver should be instructed how to apply the cream, taking care to apply only a small amount to the semitranslucent line of adhesions by rubbing the cream into the skin using a cotton swab while applying gentle labial traction. Girls should be monitored for adverse effects of estrogen therapy, including breast budding and vaginal bleeding. To decrease the risk of recurrence and to prevent reagglutination of raw opposing skin surfaces, an emollient can be applied nightly for at least 1 month after the initial separation. Labial adhesions should not be separated manually in the office without anesthesia, as it can be very painful and may preclude subsequent examinations because of fear of pain.
Lichen sclerosus produces a sclerotic, atrophic, parchment-like plaque with an hourglass or keyhole appearance that can affect the vulvar, perianal, or perineal skin. The affected area breaks down easily; thus, girls may present with vulvar bleeding. Accompanying subepithelial hemorrhages may be misinterpreted as sexual abuse or trauma. Alternatively, the patient may experience perineal itching, soreness, or dysuria. The etiology of lichen sclerosus is unknown, although a relationship to autoimmune disease is currently the most accepted theory. In the past, it was believed that childhood lichen sclerosus resolved at puberty; however, there are now many reports of childhood lichen sclerosus persisting into adulthood (see also “Vulvar Skin Disorders” in Part 4). Treatment includes avoidance of trauma by having the patient avoid irritation to the vulvar area. Ultrapotent topical corticosteroids are considered first-line therapy. Once symptoms are under control, the patient should be tapered off the drug unless therapy is required for a flare-up.
Precocious Puberty
Onset of puberty is affected by race, family history, birth weight, nutrition, international adoption, and exposure to estrogenic chemicals. Precocious puberty was defined previously as sexual development in girls younger than 8 years. However, the Lawson Wilkins Pediatric Endocrine Society guidelines for the evaluation of premature development state that pubic hair or breast development requires evaluation only when it occurs before age 7 years in non-African American girls and before age 6 years in African American girls.
Precocious puberty is classified based on the underlying pathologic mechanism. Central precocious puberty, also known as gonadotropinreleasing hormone (GnRH)-dependent precocious puberty, results from early reactivation of the hypothalamic-pituitary-gonadal axis. Peripheral (or GnRH-independent) precocious puberty is the result of excess estrogen or androgen from overproduction by the ovaries or adrenal glands or from external sources. Possible causes of each type are listed in Box 3-24.
Box 3-24. Causes and Classifications of Sexual Precocity in Females
Complete Isosexual Precocious Puberty (GnRH-dependent)
Familial
Idiopathic
Central nervous system tumors
• Harmartoma of the tuber cinereum
• Neurofibromatosis type I (cranioptic glioma)
• Hypothalamic astrocytoma
• Ependymoma
Other central nervous system disorders
Infections (eg, encephalitis or abscess)
Infiltrative disease (eg, sarcoid or tuberculousis)
Trauma
High intracranial pressures (eg, hydrocephalus or subarachnoid cyst)
Radiation
Androgen exposure (late onset congenital adrenal hyperplasia)
Children adopted from developing countries
Incomplete Isosexual Precocious Puberty (GnRH-independent)
Gonadotropin-secretory tumors
• Central nervous system (eg, germinoma)
• Not related to the central nervous system (eg, choriocarcinoma)
Excess androgen production
• Congenital adrenal hyperplasia
• Adrenal neoplasm
• Leydig cell adenoma
(continued)
Box 3-24. Causes and Classifications of Sexual Precocity in Females (continued)
Excess estrogen production
• Ovarian cysts and follicles
• Estrogen producing neoplasms of the ovary or adrenal gland
• McCune-Albright syndrome
• Peutz-Jeghers syndrome
Exogenous (eg, steroid hormones or foods)
Hypothyroidism
Variants
• Premature thelarche or adrenarche
• Premature isolated menarche
Abbreviation: GnRH, gonadotropin-releasing hormone.
Modified with permission from Styne DM, Cuttler L. Abnormal pubertal development. In: Rudolph CD, Rudolph AM, Lister GE, First LR, and Gershon AA, editors. Rudolph’s pediatrics. 22nd ed. New York (NY): McGraw-Hill Medical; 2011. p. 2077-86.
The clinician should strive to determine the cause and mechanism by evaluation of clinical findings and laboratory testing or refer the patient to a pediatric gynecologist or pediatric endocrinologist for diagnosis and management. The child may require observation of progression from one stage of pubertal development to the next in less than 3-6 months. Diagnostic studies include measurement of accelerated growth velocity demonstrated by growth charts and advanced bone age. Pelvic ultrasonography may show presence of ovarian or adrenal pathology or uterine maturation. Serum estradiol levels should be measured. A level above 100 pg/mL may be associated with an ovarian cyst or tumor. It is appropriate to check basal and GnRH-stimulated luteinizing hormone levels. Pubertal girls should show no, or minimal, increase in luteinizing hormone and follicle-stimulating hormone in response to GnRH. An increase in luteinizing hormone into the adult range occurs in central precocious puberty. In all cases of central precocious puberty, magnetic resonance imaging of the brain is needed to determine if a central nervous system lesion is present. Treatment is dependent on cause and includes medical suppression of puberty with GnRH agonists or surgery for pelvic or pituitary tumors.
Benign variants of precocious puberty include isolated secondary sexual characteristics without increased growth velocity. Isolated precocious the- larche refers to unilateral or bilateral breast development. Isolated precocious pubarche is associated with pubic hair development, adult body odor, axillary hair, or mild acne with normal cortisol precursors in serum, including normal 17α-hydroxyprogesterone level after corticotrophin stimulation. Isolated precocious menarche—defined as vaginal bleeding without breast or pubic hair development, a vaginal lesion (tumor or foreign body), or trauma—is a rare event and usually is attributed to transient ovarian activity. Patients with benign variants of precocious puberty have normal prepubertal pelvic anatomy by ultrasonography and prepubertal hormonal responses to stimulation studies. Follow-up is recommended because progression can occur.
Sexual Abuse ^426
Approximately one in five girls is a victim of some type of sexual abuse during childhood. Most perpetrators are males who are known and trusted by the family (eg, fathers, male relatives, friends of the family, and babysitters). Abductions and abuse by strangers are rare.
Urgent evaluation is required for collection of forensic evidence if the reported abuse has occurred within 72 hours. It is critical to vigorously pursue the collection of clothing and linens. In one study of children evaluated for sexual abuse in the emergency department, most of the forensic evidence collected 24 hours or more after the assault was obtained from clothing and linens. If the abuse occurred more than 72 hours earlier and the child is currently not in danger and free from injuries, she can be evaluated on a nonemergent basis.
The obstetrician-gynecologist should be aware of resources in the community for the evaluation of sexual abuse. Often, departments of children’s services or local pediatric hospitals can help refer the child and her family to professionals with experience in interviewing and examining children suspected to be victims of sexual abuse.
Every state requires suspected and known sexual abuse to be reported. In situations in which the gynecologist is unsure if a report should be filed, local child protective service personnel can be helpful. A goal is to avoid filing vague and unnecessary reports that overburden the system but to file borderline reports when any child’s safety is unclear. Many signs and symptoms consistent with abuse, such as nightmares or prepubertal bleeding, also have other causes. The state statutes do not imply that every observation of these signs and symptoms in a child requires a report of possible sexual abuse. The American Academy of Pediatrics has developed guidelines on appropriate filing (see Resources). Liability issues related to false reporting have not been problematic and should never impede filing.
Most children who have been sexually abused will have normal findings on examination. Findings that suggest abuse include lacerations of the vulva, posterior fourchette, or anus and transection of the hymen. However, hymen diameters are not a reliable marker of abuse. Prepubertal bleeding may be seen but usually is not present in abused children.
Approximately 5% of abused children will acquire a sexually transmitted infection; the clinician must decide if culturing for sexually transmitted infections is appropriate by evaluating the individual situation and taking into account community standards. Children with gonorrhea or chlamydial infection generally are symptomatic and have vaginal discharge. Gonorrhea and chlamydial infection cause vaginitis (not cervicitis) in children, so if a culture is performed, it should be taken from the vagina rather than the endocervix. If testing is done, the CDC recommends performing a culture instead of indirect or DNA testing (specifically, NAATs) because there are limited data on the use of these tests in children and these tests may not be admissible in courts because they are not labeled for use in children.
Psychologic support and therapy with a qualified mental health professional are often critical. For more information see the “Abuse” section later in Part 3.
Bibliography
American College of Obstetricians and Gynecologists. General management of pediatric gynecology patients. In: Guidelines for Adolescent Health Care. Washington, DC: ACOG; 2011. pp. 172-192.
Bayerl C, Feller G, Goerdt S. Experience in treating molluscum contagiosum in children with imiquimod 5% cream. Br J Dermatol 2003;149 Suppl 66:25-9. [PubMed] Carel JC, Eugster EA, Rogol A, Ghizzoni L, Palmert MR, Antoniazzi F, et al. Consensus statement on the use of gonadotropin-releasing hormone analogs in children. ESPE-LWPES GnRH Analogs Consensus Conference Group. Pediatrics 2009;123:e752-62. [PubMed] [Full Text]
Davis AJ, Emans SJ. Human papilloma virus infection in the pediatric and adolescent patient. J Pediatr 1989;115:1-9. [PubMed]
Emans SJ, Laufer MR, Goldstein DP. Pediatric and adolescent gynecology. 5th ed. Philadelphia (PA): Lippincott Williams & Wilkins; 2005.
Kaplowitz PB. Treatment of central precocious puberty. Curr Opin Endocrinol Diabetes Obes 2009;16:31-6. [PubMed]
Kaplowitz PB, Oberfield SE. Reexamination of the age limit for defining when puberty is precocious in girls in the United States: implications for evaluation and treatment. Drug and Therapeutics and Executive Committees of the Lawson Wilkins Pediatric Endocrine Society. Pediatrics 1999;104:936-41. [PubMed] [Full Text]
Lewin LC. Sexually transmitted infections in preadolescent children. J Pediatr Health Care 2007;21:153-61. [PubMed]
Liota E, Smith KJ, Buckley R, Menon P, Skelton H. Imiquimod therapy for molluscum contagiosum. J Cutan Med Surg 2000;4:76-82. [PubMed]
Majewski S, Pniewski T, Malejczyk M, Jablonska S. Imiquimod is highly effective for extensive, hyperproliferative condyloma in children. Pediatr Dermatol 2003;20:440-42. [PubMed]
Nelson KC, Morrell DS. Spreading bumps: molluscum contagiosum in the pediatric population. Pediatr Ann 2007;36:814, 816-8. [PubMed]
Papp JR, Schachter J, Gaydos CA, Van Der Pol B. Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae-2014. Division of STD Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, CDC. MMWR Recomm Rep 2014;63(RR02):1-19. [PubMed] [Full Text]
Poindexter G, Morrell DS. Anogenital pruritus: lichen sclerosus in children. Pediatr Ann 2007;36:785-91. [PubMed]
Protecting children from sexual abuse by health care providers. American Academy of Pediatrics Committee on Child Abuse and Neglect. Pediatrics 2011;128:407-26. [PubMed] [Full Text]
Sanfilippo JS, Lara-Torre E, Edmonds DK, Templeman C, editors. Clinical pediatric and adolescent gynecology. New York (NY): Informa Healthcare; 2009.
Siegfried EC, Frasier LD. Anogenital warts in children. Adv Dermatol 1997;12: 141-66; discussion 167. [PubMed]
Smolinski KN, Yan AC. How and when to treat molluscum contagiosum and warts in children. Pediatr Ann 2005;34:211-21. [PubMed]
Styne DM, Cuttler L. Abnormal pubertal development. In: Rudolph CD, Rudolph AM, Lister GE, First LR, Gershon AA, editors. Rudolph's pediatrics. 22nd ed. New York (NY): McGraw Hill Medical; 2011. p. 2077-86.
Tschudy MM, Arcara KM, editors. The Harriet Lane handbook: a manual for pediatric house officers. The Harriet Lane Service, Children's Medical and Surgical Center of the Johns Hopkins Hospital. 19th ed. Philadelphia (PA): Elsevier Mosby; 2012.
Vaginitis. ACOG Practice Bulletin No. 72. American College of Obstetricians and Gynecologists. Obstet Gynecol 2006;107:1195-206. [PubMed] [Obstetrics & Gynecology]
Resources
American Academy of Pediatrics. Bright Futures™. Available at: http://brightfutures. aap.org/index.html. Retrieved September 27, 2013.
American Academy of Pediatrics. Red book: report of the Committee on Infectious Diseases. 29th ed. Elk Grove Village (IL): American Academy of Pediatrics; 2012.
Kellogg N. The evaluation of sexual abuse in children. American Academy of Pediatrics Committee on Child Abuse and Neglect. Pediatrics 2005;116:506-12. [PubMed] [Full Text]
North American Society for Pediatric and Adolescent Gynecology. Available at: http://www.naspag.org. Retrieved September 27, 2013.
Sexual assault. Committee Opinion No. 592. American College of Obstetricians and Gynecologists. Obstet Gynecol 2014;123:905-9. [PubMed] [Obstetrics & Gynecology] Workowski KA, Berman S. Sexually transmitted diseases treatment guidelines, 2010. Centers for Disease Control and Prevention [published erratum appears in MMWR Morb Mortal Wkly Rep 2011;60:18]. MMWR Recomm Rep 2010;59:1-110. [PubMed] [Full Text]