I SEXUALLY TRANSMITTED INFECTIONS ^xv ^229 ^348 ^386
Sexually transmitted infections (STIs) can be acquired through contact during oral, vaginal, or anal sex. The transmission of an STI may result in myriad consequences, including infertility, chronic pelvic pain, cancer, and even death; in addition to its physical effects, it can cause psychologic distress and be a strain on personal relationships.
Sexually transmitted infections are the number one cause of preventable infertility and are strongly associated with ectopic pregnancy. They may increase the risk of human immunodeficiency virus (HIV) acquisition threefold to fivefold, and their management is a critical strategy in the prevention of HIV infection. The Institute of Medicine has highlighted that U.S. STI rates are the highest in the industrialized world, and in some communities they are comparable to infection rates in many developing countries.Prevention
Prevention of STIs includes strategies to decrease exposure through delaying the onset of sexual activity, limiting the number of sexual partners, limiting exposure to high-risk partners, limiting risky sexual practices, encouraging immunization, and increasing the use of condoms. Preventing the spread of STIs in a population also can include partner notification and treatment
and reporting of diseases when required. Gonorrhea, syphilis, chlamydial infection, and HIV and acquired immunodeficiency syndrome (AIDS) are reportable diseases in every U.S. state. Clinicians should be familiar with any federal, state, or local requirements for the screening, follow-up, and reporting of STIs.
Abstinence from sexual activity is the most effective way to avoid STIs, including human papillomavirus (HPV) infection. However, an abstinence-only counseling strategy is not an effective first-line strategy. Clinicians should not condemn or chastise young patients regarding sexual activity.
Instead, they should provide information and counsel patients regarding the risks of STIs and unintended pregnancy. Some patients may not consider themselves to be sexually active or at risk of acquiring STIs if engaged in oral or anal sex, and this perception should be considered when taking a sexual history. Limiting the number of sexual partners may decrease one's risk of STIs, including HPV infection.Recommended immunizations for preventable STIs, such as hepatitis and HPV infection, for various age groups are available at www.acog.org/ wellwoman. A quadrivalent vaccine against HPV types 6, 11, 16, and 18 and a bivalent vaccine against HPV types 16 and 18 are now available. The Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention (CDC) has recommended the initial vaccination target of females aged 11 years or 12 years with either the bivalent or quadrivalent vaccine. In addition, the Advisory Committee on Immunization Practices recommends routine vaccination of males aged 11 years or 12 years with the quadrivalent vaccine. Although obstetrician-gynecologists are not likely to care for many girls in this initial vaccination target group, these clinicians are critical to the widespread use of the vaccine for females aged 13-26 years (see also the “Immunizations” section earlier in Part 3). The HPV vaccine is not intended to treat patients with cervical cytologic abnormalities or genital warts. Patients with these conditions should undergo the appropriate evaluation and treatment (see also the “Abnormal Cervical Cytology” section in Part 4). It is important to note that many early cytologic abnormalities can be detected and managed conservatively, given the significant rate of regression. This is especially true in adolescents and young women.
If used consistently and correctly, latex condoms reduce the likelihood of HPV acquisition and HPV-related cervical dysplasia. Clinician counseling on condoms should include educating patients on the proper use of male condoms.
This education is particularly important in young populations, who have significantly higher rates of breakage and slippage. The following question may guide counseling in noncondom users who are at risk of STIs: “The last time you did not use a condom, what were the reasons?” Answers might include nonavailability, lack of time or knowledge, or partner objection. The CDC recommendations for proper use of male condoms are provided in Box 3-21.Three types of male condoms are available in the United States: 1) natural membrane (sometimes referred to as lambskin), 2) polyurethane, and 3) latex. Natural membrane condoms are not recommended for STI prophylaxis and should be used only for pregnancy prevention, because
Box 3-21. Centers for Disease Control and Prevention Recommendations for Proper Use of Male Condoms
• Use a new condom with each sex act (eg, oral, vaginal, and anal).
• Carefully handle the condom to avoid damaging it with fingernails, teeth, or other sharp objects.
• Put the condom on after the penis is erect and before any genital, oral, or anal contact with the partner.
• Use only water-based lubricants (eg, glycerin) with latex condoms. Oilbased lubricants (eg, petroleum jelly, shortening, mineral oil, massage oils, body lotions, and cooking oil) can weaken latex and should not be used.
• Ensure adequate lubrication during vaginal and anal sex, which might require the use of exogenous water-based lubricants.
• To prevent the condom from slipping off, hold the condom firmly against the base of the penis during withdrawal, and withdraw while the penis is still erect.
Reprinted from Workowski KA, Berman S. Sexually transmitted diseases treatment guidelines, 2010. Centers for Disease Control and Prevention [published erratum appears in MMWR Morb Mortal Wkly Rep 2011;60:18]. MMWR Recomm Rep 2010;59:1-110. they may allow pathogens to pass through their pores. Latex condoms are the optimal choice for most individuals. Polyurethane condoms, which are approximately double the cost of latex condoms but provide similar protection against STIs and pregnancy, are recommended if either sexual partner has a history of latex allergy.
Slippage and breakage rates are significantly higher for polyurethane condoms. The CDC does not recommend condoms lubricated with spermicides for STI and HIV prevention. Condoms lubricated with spermicides are no more effective than other lubricated condoms for STI and HIV prevention. In addition, condoms lubricated with spermicide have been associated with urinary tract infection in young women, and frequent use of spermicides that contain nonoxynol-9 has been associated with a possible higher risk of HIV transmission through disruption of the genital epithelium.Laboratory studies indicate that the female condom, which now consists of a lubricated nitrile sheath with a ring on each end that is inserted into the vagina, is an effective mechanical barrier to viruses, including HIV, and to semen. A limited number of clinical studies have evaluated the efficacy of female condoms in providing protection from STIs, including HIV. Just as the male condom, the female condom substantially reduces the risk of STI acquisition if used consistently and correctly. When a male condom cannot be used properly, sex partners should consider using a female condom. Female condoms are more costly compared with male condoms. The female condom also can be used for STI and HIV protection during receptive anal intercourse. Its efficacy in prevention of STI transmission in this setting is undefined.
Clinicians can arrange directly for partner notification or treatment of STIs or use local or state health departments as referral sites. Treatment of male sexual partners is important in the prevention of transmission and reinfection with certain STIs. Clinicians may be asked to provide a prescription for the patient’s partner without having performed an examination of the individual, an approach known as expedited partner therapy. A CDC review of the evidence has found expedited partner therapy to be a useful option, especially for treatment of male partners of women with gonorrhea or chlamydial infection (see Bibliography).
However, state law and liability standards may prohibit expedited partner therapy in some areas. Clinicians are encouraged to become familiar with local regulations and resources. In addition, the recent changes to CDC treatment recommendations to require an intramuscular cephalosporin as part of the first-line treatment for gonorrhea will be an impediment to expedited partner therapy. In most cases, such a prescription will result in treatment without complication. An adverse reaction to the medication is uncommon but may result in a significant health hazard to the partner. Each clinician must decide whether providing such prescriptions is appropriate. Male partners who receive expedited partner therapy should be encouraged to seek medical evaluation.Screening
Appropriate STI screening in nonpregnant women depends on the age of the patient and assessment of risk factors elicited during the medical and sexual history. Box 3-22 details guidelines on routine screening and screening based on risk factors. Optimal rescreening intervals are ill defined but should take into account any change in sexual partners. The CDC advises that urine or swab specimens from the endocervix or vagina can be used for screening and diagnosis, and that nucleic acid amplification tests are the most sensitive tests for these specimens. Recent studies indicate that self-collected vaginal swabs combined with nucleic acid amplification tests testing are highly acceptable to patients and may result in increased screening rates. An endocervical swab is appropriate when another indication for a pelvic examination is present.
The CDC and the American College of Obstetricians and Gynecologists (the College) recommend that females aged 13-64 years be screened for HIV at least once in their lifetime and then annually thereafter based on factors related to risk (see Box 3-22). In addition, obstetrician-gynecologists should annually review patients’ risk factors for HIV and assess the need for retesting.
Screening after age 64 years is indicated if there is ongoing risk for HIV infection, as indicated by risk assessment (eg, new sexual partners). Ideally, opt-out HIV screening should be performed, in which the patient is notified that HIV testing will be performed as a routine part of gynecologic and obstetric care unless the patient declines testing. However, state and local laws on HIV testing may not be consistent with such an approach;Box 3-22. The American College of Obstetricians and Gynecologists’ Sexually Transmitted Infection Screening Recommendations* ^
Routine Screening:
• Sexually active women aged 25 years and younger should be screened annually for chlamydial infection and gonorrhea. Screening also is recommended for women older than 25 years with risk factors (see “Screening Based on Risk Factors” later in this box). Note that urine-based sexually transmitted infection (STI) screening is an efficient means for accomplishing this without a speculum examination.
• Women with developmental disabilities should be screened for STIs.
• Human immunodeficiency virus (HIV) screening is recommended for females aged 13-64 years. Obstetrician-gynecologists should annually review patients’ risk factors for HIV and assess the need for retesting. Ideally, opt-out HIV screening should be performed, in which the patient is notified that HIV testing will be performed as a routine part of gynecologic and obstetric care unless the patient declines testing.1
• One-time hepatitis C virus testing is recommended for individuals born from 1945 through 1965 and unaware of their infection status.
Screening Based on Risk Factors:
• Women should be regularly screened for STIs if they have a history of multiple sexual partners or a sexual partner with multiple contacts; sexual contact with individuals with culture-proven STIs; repeated episodes of STIs; or attendance at clinics for STIs. Other women who should be screened regularly include asymptomatic women older than 25 years with risk factors for chlamydial infection (eg, new or multiple sexual partners) or for gonorrhea (those who live in a high-prevalence area, have had a previous gonococcal infection, have other STIs, have new or multiple sex partners, use condoms inconsistently, participate in sex work, and use drugs).
• Syphilis testing is recommended for sexually active adolescents who exchange sex for drugs or money, use intravenous drugs, are entering a detention facility, or live in a high-prevalence area.
• Human immunodeficiency virus screening should be offered at least annually to women who are injection drug users; are sex partners of injection-drug users; exchange sex for money or drugs; are sex partners
Box 3-22. The American College of Obstetricians and Gynecologists’ Sexually Transmitted Infection Screening Recommendations[†††] (continued)
of HIV-infected persons; have had sex with men who have sex with men since their most recent HIV test; or have had more than one sex partner since their most recent HIV test. Human immunodeficiency virus testing should be recommended to all women seeking preconception care.
• Hepatitis C virus testing is recommended for all individuals with HIV infection, history of injecting illegal drugs, recipients of clotting factor concentrates before 1987, chronic (long-term) hemodialysis, persistently abnormal alanine aminotransferase levels, recipients of blood from donors who later tested positive for hepatitis C virus infection, recipients of blood or blood-component transfusion or organ transplant before July 1992, or occupational percutaneous or mucosal exposure to hepatitis C virus-positive blood.
therefore, physicians should be aware of, and follow, the HIV screening requirements in their jurisdiction.
Diagnosis and Management
Many infections are asymptomatic, and presenting history and examination findings vary. Table 3-11, Table 3-12, and the following discussion provide a brief overview of the diagnosis and management of some of the most common STIs. Information on bacterial vaginosis and trichomoniasis is provided in the “Vaginitis” section in Part 4. Detailed information on the management of STIs is provided in the most recent STI treatment guidelines published by the CDC (see www.cdc.gov/std).
Pelvic Inflammatory Disease
Pelvic inflammatory disease, a leading cause of infertility, is associated with STIs. No specific finding or test is sensitive and specific for the diagnosis of PID. Many cases go unrecognized and may present with mild, nonspecific symptoms, such as abnormal bleeding or vaginal discharge. The CDC recommends that practitioners have a low threshold for diagnosing PID, given the potential for infertility in what appears to be mild or atypical PID. The CDC advises empiric treatment for PID in sexually active young women and other women at risk of STIs if no other cause of the illness can be identified and any one of the following is present on pelvic examination: uterine tenderness, adnexal tenderness, or cervical motion tenderness. The CDC also recommends that all women with diagnosed acute PID be tested for chlamydial infection, gonorrhea, and HIV infection. Most, but not all, women with PID will have white blood cells in their vagina or a mucopurulent cervical discharge. In patients without these findings, the diagnosis of PID is unlikely, and thorough evaluation should investigate other possible sources of pain.
The routine use of laparoscopy to diagnose PID is not indicated because of cost and operative risk. However, if the diagnosis is uncertain, the patient fails to respond to therapy, or symptoms recur soon after adequate therapy, diagnostic laparoscopy may be indicated to rule out other conditions causing pain, such as endometriosis, ruptured ovarian cyst, or adnexal torsion.
The CDC recommends that therapy with recommended treatment regimens be initiated as soon as the presumptive diagnosis of PID has been
Table 3-11. Diseases Characterized by Genital Ulcers* ^
• Differential diagnosis: genital herpes, syphilis, chancroid, and nonsexually transmitted infections
• Diagnosis: history and physical examination frequently inaccurate; all patients should be tested for syphilis and herpes; consideration given to chancroid
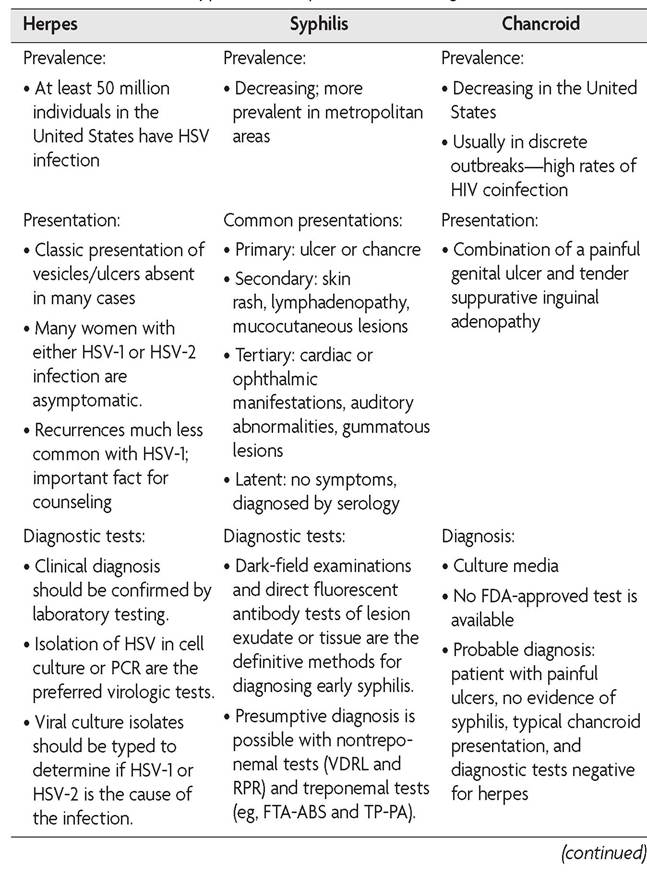
Table 3-11. Diseases Characterized by Genital Ulcers* (continued)
| Herpes | Syphilis | Chancroid |
| Diagnostic tests: • The serologic typespecific glycoprotein G-based assays should be specifically requested when serology is performed. | Diagnostic tests: • The use of only one type of serologic test is insufficient; false-positive nontreponemal test results are sometimes associated with medical conditions unrelated to syphilis. |
*The information in this table is from the 2010 Sexually Transmitted Diseases Treatment Guidelines from the Centers for Disease Control and Prevention. A revision of these guidelines was underway during the production of the fourth edition of Guidelines for Women’s Health Care. For the most up-to-date guidance, please refer to the current Centers for Disease Control and Prevention guidelines, available at www.cdc.gov/std/.
Abbreviations: FDA, U.S. Food and Drug Administration; FTA-ABS, fluorescent treponemal antibody absorbed; HIV, human immunodeficiency virus; HSV, herpes simplex virus; PCR, polymerase chain reaction; RPR, rapid plasma reagin; TP-PA, T pallidum particle agglutination; VDRL, Venereal Disease Research Laboratory.
Data from Workowski KA, Berman S. Sexually transmitted diseases treatment guidelines, 2010. Centers for Disease Control and Prevention [published erratum appears in MMWR Morb Mortal Wkly Rep 2011;60:18]. MMWR Recomm Rep 2010;59:1-110.
Table 3-12. Diseases Characterized by Cervicitis or Urethritis*
| Chlamydial Infection | Gonorrhea |
| Prevalence: | Prevalence: |
| • Most frequently reported infectious disease in the United States • Highest prevalence in individuals 25 years and younger | • Second most commonly reported notifiable infection; it has been estimated that 700,000 new infections occur each year in the United States • Prevalence varies widely among communities and populations. • Women younger than 25 years are at highest risk. |
Tahle 3-12 Diceacec Characterized hv Cerviritic or Hrethritic* (continued
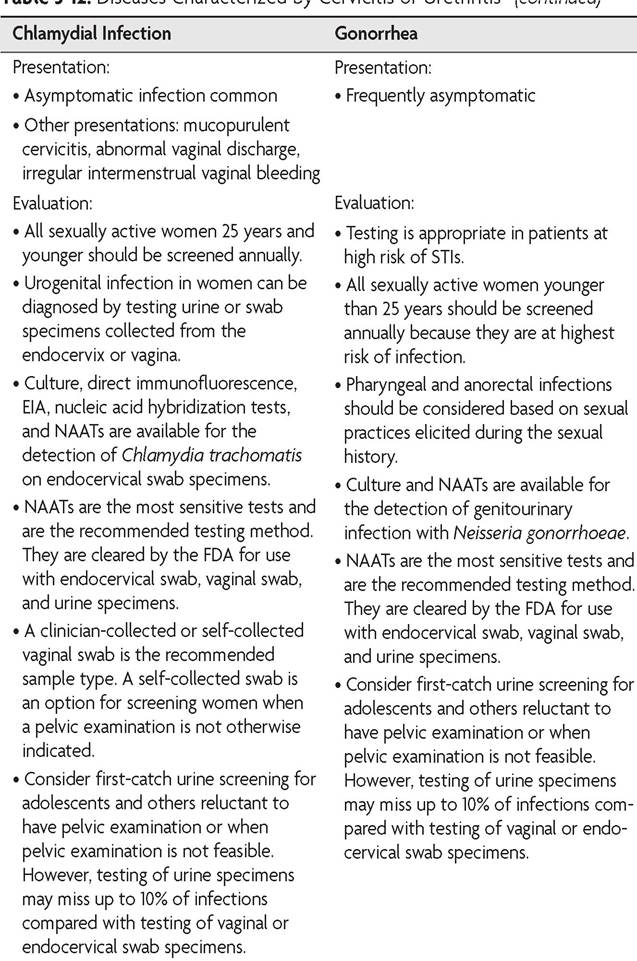
Table 3-12. Diseases Characterized by Cervicitis or Urethritis[‡‡‡] (continued)
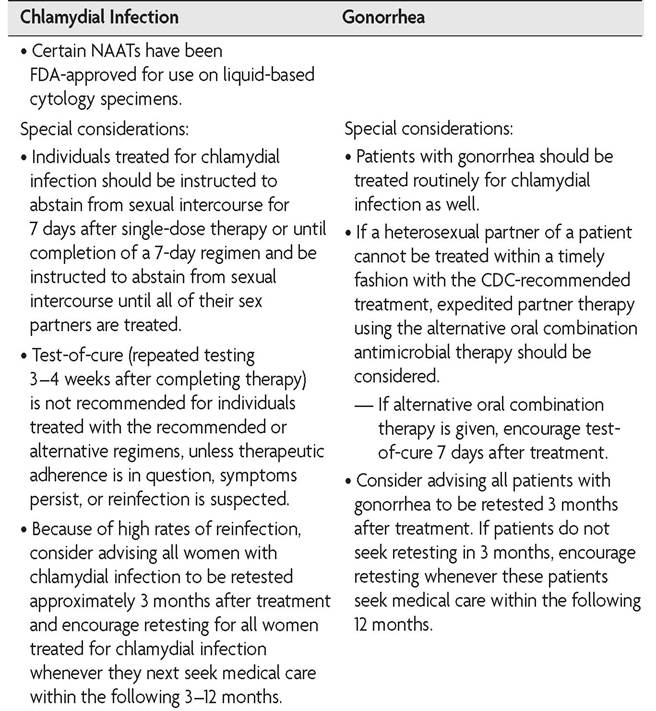
Table 3-12. Diseases Characterized by Cervicitis or Urethritis[§§§] (continued)
Mortal Wkly Rep 2011;60:18]. MMWR Recomm Rep 2010;59:1-110; Update to CDCs Sexually transmitted diseases treatment guidelines, 2010: oral cephalosporins no longer a recommended treatment for gonococcal infections. Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep 2012;61:590-4; and Papp JR, Schachter J, Gaydos CA, Van Der Pol B. Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae-2014. Division of STD Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, CDC. MMWR Recomm Rep 2014;63(RR02):1-19.
made. The CDC also notes that clinicians should consider availability, cost, patient acceptance, and antimicrobial susceptibility when selecting a treatment regimen.
Outpatient therapy can provide similar outcomes to inpatient therapy for women with mild or moderate PID. It is important to assess response to treatment when outpatient therapy is provided. The decision to hospitalize must be individualized. The CDC has listed suggested criteria for hospitalization (see Box 3-23). Adolescents with PID often are hospitalized, but data do not substantiate that they benefit from inpatient therapy
Box 3-23. Suggested Criteria for Hospitalization for Pelvic Inflammatory Disease* ^
• Surgical emergencies (eg, appendicitis) cannot be excluded.
• The patient is pregnant.
• The patient does not respond clinically to oral antimicrobial therapy.
• The patient is unable to follow or tolerate an outpatient oral regimen.
• The patient has severe illness, nausea and vomiting, or high fever.
• The patient has a tuboovarian abscess. more than other age groups. Young women with mild-to-moderate disease have similar outcomes with either inpatient therapy or outpatient therapy, and response to outpatient therapy is similar across age groups. The CDC recommends that the same criteria used to determine the need for hospitalization of older women be used for adolescents with acute PID.
Human Papillomavirus Infection
Infection with one or more HPV subtypes is extremely common, occurring in up to 80% of sexually active women by age 50 years. It appears that most young, sexually active men and women are, or have been, infected with this organism. Most cervical HPV infections appear to be transient, but the proportion of women whose infections are resolved decreases with age. In one prospective study, the time required for 50% of prevalent cases to become HPV DNA-negative was 4.8 months for nononcogenic types and 8.1 months for oncogenic types. This finding may not reflect the true duration of infection because it is unknown how long the women had been infected at the time of enrollment in the study. Infections of the cervix often are diagnosed through assessment of cervical cytology (see also the “Well-Woman Annual Health Assessment” section earlier in Part 3).
Some subtypes (particularly the nononcogenic types, such as types 6 and 11) are associated with the development of genital warts. In most cases, external warts can be treated with the topical application of podo- filox, imiquimod, trichloroacetic or bichloroacetic acid, or podophyllin resin or the use of cryotherapy, laser ablation, or electrocautery. Treatment should be guided by the preference of the patient and the experience of the clinician. Patients who fail to respond to treatment may be immunosuppressed and should be counseled about, and offered, testing for HIV. Patients known to be immunosuppressed (eg, transplant patients, chronic steroid users, and HIV-positive patients) should receive HPV and STI prevention counseling.
Infectious Hepatitis
Infection with hepatitis B virus (HBV) is contracted more often by other routes of exposure, although some studies have suggested that up to 60% of all such infections result from sexual transmission. Women who have active HBV infections or women who are HBV carriers should be counseled to have their partners use condoms during intercourse. They should avoid oral-genital contact. Patients with STIs, all adolescents not previously immunized, and others who are considered to be at high risk (see ACOG Annual Women’s Health Care www.acog.org/About_ACOG/ ACOG_Departments/Annual_Womens_Health_Care/High-Risk_Factors) should be offered HBV vaccination. Hepatitis B vaccination also should be initiated in nonimmunized sexual assault victims.
Human Immunodeficiency Virus Infection
The CDC estimates that approximately 40,000-50,000 new HIV infections occurred annually in the United States from 2006 to 2009. Almost one in five (18.1%) of all individuals infected with HIV are unaware of their HIV status. Heterosexual contact is the leading mode of HIV transmission in women. Women with STIs have an increased risk of HIV infection. In 2010, women accounted for more than 22% of new HIV infections diagnosed.
Women should be counseled routinely regarding HIV infection. The obstetrician-gynecologist should be prepared to educate patients about the modes of transmission of the virus, means of protection from infection, and the significance of HIV infection in pregnancy. Prevention of HIV infection should be a priority. Voluntary and confidential HIV testing should be available to any woman who wishes to be tested.
Physicians should be aware of, and follow, their states’ HIV testing requirements. Clinicians should consult their state medical associations for more information on state laws governing HIV testing and test results. The CDC recommends that patients be notified that testing will be performed, but separate written consent and prevention counseling should not be required.
The CDC recommends that HIV-negative test results may be conveyed without direct personal contact with the patient. Individuals known to be at high risk of HIV infection should be advised of the need for periodic retesting and should be offered, or be referred for, prevention counseling. Individuals with HIV-positive test results should receive confidential communication of test results through personal contact by a clinician, nurse, midlevel practitioner, counselor, or other skilled staff member. Individuals who test positive for HIV should receive, or be referred for, clinical care promptly.
Several U.S. Food and Drug Administration-approved rapid HIV tests are available. With rapid HIV testing, results are available in 10-30 minutes if given at the point of care. Currently, blood and oral fluid rapid tests are used. Positive screening test results should be confirmed. Point-of-care testing facilitates screening in settings with limited access to laboratories but also allows patients in all settings, including the routine visit, to learn their test results during that visit. Such immediate notice not only reduces the number of individuals who do not return to learn their test results but also allows for prompt entry into care. The CDC recommends rapid HIV testing in settings such as emergency departments, STI clinics, and annual visits. Clinicians should develop resources to allow them to provide appropriate counseling and support services if they use rapid testing.
It is unethical for an obstetrician-gynecologist to refuse to accept as patients or to refuse to continue to care for individuals solely because they are, or are thought to be, seropositive for HIV. Health care providers should observe standard precautions to minimize skin, mucous membrane, and percutaneous exposure to blood, secretions, and body fluids from all patients to protect against a variety of pathogens, including HIV. In making decisions about patient-care activities, a health care worker infected with HIV should adhere to the fundamental professional obligation to avoid harm to patients (see also the “Human Resources” section in Part 1).
Sexual Health Risks of Noncoital Sexual Activity
Noncoital sexual behaviors, including activities such as mutual masturbation, oral sex, and anal sex, are common. Although these behaviors carry little to no risk of pregnancy, patients should be counseled that noncoital sexual activity is not necessarily “safe sex.” Anal sex poses a particularly high risk because tissues in the rectum break easily, and organisms can be transmitted through breaks in skin and mucosal surfaces. Oral-genital sex is known to be a method of transmission of several STIs. Because people define sexuality in a variety of ways and may not report noncoital sexual activity, it is important that clinicians ask direct questions regarding sexual activity, including whether the patient has sex with men, women, or both; the number of sexual partners and her partners’ sexual behavior; and frequency of oral and anal sex and mutual masturbation.
Counseling about noncoital sexual activity should address the risk of STIs during noncoital sexual activity and encourage STI prevention efforts. Clinicians also should consider the patient’s history of STIs and patterns of barrier method use with each partner, as well as the local prevalence of STIs (available from local health departments). Use of latex or synthetic condoms during anal-genital intercourse to reduce the risk of STIs should be encouraged. Use of barrier protection during oral sex also should be encouraged. Latex sheets have been approved by the U.S. Food and Drug Administration for use to reduce the risk of transmission of STIs during oral sex; however, no effectiveness data are available. Dental dams (or oral dams), household plastic wrap, and condoms adapted to form a barrier sheet are other options for barrier protection for oral sex; however, these products have not been evaluated or cleared by the U.S. Food and Drug Administration for this use and no effectiveness data are available. Counseling also should include the risk of STI transmission with the use of sex toys and encourage cleaning of and condom use on sex toys.
Bibliography
Adams DA, Gallagher KM, Jajosky RA, Kriseman J, Sharp P, Anderson WJ, et al. Summary of Notifiable Diseases - United States, 2011. Division of Notifiable Diseases and Healthcare Information, Office of Surveillance, Epidemiology, and Laboratory Services, CDC. MMWR Morb Mortal Wkly Rep 2013;60:1-117. [PubMed] [Full Text]
Addressing health risks of noncoital sexual activity. Committee Opinion No. 582. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013; 122:1378-83. [PubMed] [Obstetrics & Gynecology]
American College of Obstetricians and Gynecologists. Sexually transmitted infections in adolescents. In: Guidelines for adolescent health care [CD-ROM]. 2nd ed. Washington, DC: American College of Obstetricians and Gynecologists; 2011. p. 64-72.
American College of Obstetricians and Gynecologists. Annual women’s health care. Available at: http://www.acog.org/wellwoman. Retrieved October 1, 2013.
American College of Obstetricians and Gynecologists. Annual women’s health care: high risk factors. Available at: http://www.acog.org/About_ACOG/ACOG_Depart ments/Annual_Womens_Health_Care/High-Risk_Factors. Retrieved October 1, 2013.
Calonge N. Screening for syphilis infection: recommendation statement. U.S. Preventive Services Task Force [published erratum appears in Ann Fam Med 2004;2:517]. Ann Fam Med 2004;2:362-5. [PubMed] [Full Text]
Centers for Disease Control and Prevention. Expedited partner therapy in the management of sexually transmitted diseases: review and guidance. Atlanta (GA): CDC; 2006. Available at: http://www.cdc.gov/std/treatment/eptfinalreport2006. pdf. Retrieved July 29, 2013.
Centers for Disease Control and Prevention. Guidance on the use of expedited partner therapy in the treatment of gonorrhea. Atlanta (GA): CDC; 2012. Available at: http://www.cdc.gov/std/ept/GC-EPT-GuidanceNov-2012.pdf. Retrieved July 29, 2013.
Centers for Disease Control and Prevention. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data—United States and 6 U.S. dependent areas—2010. HIV Surveillance Supplemental Report 2012;17 (No. 3, part A). Atlanta (GA): CDC; 2012. Available at: http://www.cdc.gov/hiv/pdf/ statistics_2010_HIV_Surveillance_Report_vol_17_no_3.pdf. Retrieved December 11, 2013.
Centers for Disease Control and Prevention. Sexually transmitted diseases. Available at: http://www.cdc.gov/std/. Retrieved July 29, 2013.
Expedited partner therapy in the management of gonorrhea and chlamydia by obstetrician-gynecologists. Committee Opinion No. 506. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;118:761-6. [PubMed] [Obstetrics & Gynecology]
Gynecologic herpes simplex virus infections. ACOG Practice Bulletin No. 57. American College of Obstetricians and Gynecologists. Obstet Gynecol 2004;104:1111-8. [PubMed] [Obstetrics & Gynecology]
Human immunodeficiency virus and acquired immunodeficiency syndrome and women of color. Committee Opinion No. 536. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:735-9. [PubMed] [Obstetrics & Gynecology]
Human papillomavirus vaccination. Committee Opinion No. 588. American College of Obstetricians and Gynecologists. Obstet Gynecol 2014;123:712-8. [PubMed] [Obstetrics & Gynecology]
Marrazzo JM, Cates W. Interventions to prevent sexually transmitted infections, including HIV infection. Clin Infect Dis 2011;53 Suppl 3:S64-78. [PubMed] [Full Text]
Papp JR, Schachter J, Gaydos CA, Van Der Pol B. Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae-2014. Division of STD Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, CDC. MMWR Recomm Rep 2014;63(RR02):1—19. [PubMed] [Full Text]
Prejean J, Song R, Hernandez A, Ziebell R, Green T, Walker F, et al. Estimated HIV incidence in the United States, 2006-2009. HIV Incidence Surveillance Group. PLoS One 2011;6:e17502. [PubMed] [Full Text]
Routine human immunodeficiency virus screening. Committee Opinion No. 596. American College of Obstetricians and Gynecologists. Obstet Gynecol 2014; 123:1137-9. [PubMed] [Obstetrics & Gynecology]
Screening for chlamydial infection: U.S. Preventive Services Task Force recommendation statement. U.S. Preventive Services Task Force. Ann Intern Med 2007;147:128-34. [PubMed] [Full Text]
Screening for gonorrhea: recommendation statement. U.S. Preventive Services Task Force. Ann Fam Med 2005;3:263-7. [PubMed] [Full Text]
Smith BD, Morgan RL, Beckett GA, Falck-Ytter Y, Holtzman D, Teo CG, et al. Recommendations for the identification of chronic hepatitis C virus infection among persons born during 1945-1965. Centers for Disease Control and Prevention [published erratum appears in MMWR Recomm Rep 2012;61:886]. MMWR Recomm Rep 2012;61:1-32. [PubMed] [Full Text]
Update to CDC's Sexually transmitted diseases treatment guidelines, 2010: oral cephalosporins no longer a recommended treatment for gonococcal infections. Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep 2012;61:590-4. [PubMed] [Full Text]
Workowski KA, Berman S. Sexually transmitted diseases treatment guidelines, 2010. Centers for Disease Control and Prevention [published erratum appears in MMWR Morb Mortal Wkly Rep 2011;60:18]. MMWR Recomm Rep 2010;59:1-110. [PubMed] [Full Text]
Resources
American College of Obstetricians and Gynecologists. Annual women's health care: high risk factors. Available at: http://www.acog.org/About_ACOG/ACOG_ Departments/Annual_Womens_Health_Care/High-Risk_Factors. Retrieved October 1, 2013.
American College of Obstetricians and Gynecologists. Barrier methods of contraception. Patient Education Pamphlet AP022. Washington, DC: American College of Obstetricians and Gynecologists; 2011.
American College of Obstetricians and Gynecologists. Genital herpes. ACOG Patient Education Pamphlet AP054. Washington, DC: ACOG; 2008.
American College of Obstetricians and Gynecologists. Gonorrhea, chlamydia, and syphilis. Patient Education Pamphlet AP071. Washington, DC: American College of Obstetricians and Gynecologists; 2013.
American College of Obstetricians and Gynecologists. HIV and women. ACOG Patient Education Pamphlet AP082. Washington, DC: ACOG; 2008.
American College of Obstetricians and Gynecologists. How to prevent sexually transmitted diseases. Patient Education Pamphlet AP009. Washington, DC: American College of Obstetricians and Gynecologists; 2013.
American College of Obstetricians and Gynecologists. Human papillomavirus infection. Patient Education Pamphlet AP073. Washington, DC: American College of Obstetricians and Gynecologists; 2013.
American College of Obstetricians and Gynecologists. Pelvic inflammatory disease. Patient Education Pamphlet AP077. Washington, DC: American College of Obstetricians and Gynecologists; 2010.
Branson BM, Handsfield HH, Lampe MA, Janssen RS, Taylor AW, Lyss SB, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. Centers for Disease Control and Prevention. MMWR Recomm Rep 2006;55(RR-14):1-17; quiz CE1-4. [PubMed] [Full Text]
Centers for Disease Control and Prevention. Expedited partner therapy. Available at: http://www.cdc.gov/std/ept/default.htm. Retrieved July 29, 2013.
Centers for Disease Control and Prevention. HIV/AIDS. Available at: http://www. cdc.gov/hiv. Retrieved July 29, 2013.
Centers for Disease Control and Prevention. National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. Available at: http://www.cdc.gov/nchhstp/ Default.htm. Retrieved July 30, 2013.
Centers for Disease Control and Prevention. Peer review plan for “US PHS preexposure prophylaxis for the prevention of HIV infection in the United States-2013: a clinical practice guideline and US PHS preexposure prophylaxis for the prevention of HIV infection in the United States-2013: clinical providers’ supplement.” Atlanta (GA): CDC; 2013. Available at: http://www.cdc.gov/hiv/pdf/policies_PRP_ PrEP.2.pdf. Retrieved March 28, 2014.
Chou R, Selph S, Dana T, Bougatsos C, Zakher B, Blazina I, et al. Screening for HIV: systematic review to update the U.S. Preventive Services Task Force recommendation. Evidence Synthesis No. 95. AHRQ Publication No. 12-05173-EF-1. Rockville (MD): Agency for Healthcare Research and Quality; 2012. Available at: http://www. uspreventiveservicestaskforce.org/uspstf13/hiv/hivadultes.pdf. Retrieved July 30, 2013.
Interim guidance for clinicians considering the use of preexposure prophylaxis for the prevention of HIV infection in heterosexually active adults. Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep 2012;61:586-9. [PubMed] [Full Text]
Mast EE, Weinbaum CM, Fiore AE, Alter MJ, Bell BP, Finelli L, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) Part II: immunization of adults. Advisory Committee on Immunization Practices (ACIP).Centers for Disease Control and Prevention [published erratum appears in MMWR Morb Mortal Wkly Rep 2007; 56:1114]. MMWR Recomm Rep 2006;55(RR-16):1-33; quiz CE1-4. [PubMed] [Full Text]
Moyer VA. Screening for HIV: U.S. Preventive Services Task Force Recommendation Statement. U.S. Preventive Services Task Force. Ann Intern Med 2013;159:51-60. [PubMed] [Full Text]
Smith DK, Grohskopf LA, Black RJ, Auerbach JD, Veronese F, Struble KA, et al. Antiretroviral postexposure prophylaxis after sexual, injection-drug use, or other nonoccupational exposure to HIV in the United States: recommendations from the U.S. Department of Health and Human Services. U.S. Department of Health and Human Services. MMWR Recomm Rep 2005;54(RR-2):1-20. [PubMed] [Full Text] University of California San Francisco. National HIV/AIDS Clinicians’ Consultation Center. Available at: http://www.nccc.ucsf.edu/. Retrieved July 30, 2013.