Pelvic bones and fetal skull
Understanding of the anatomy of the fetal skull and pelvic bones is important to obstetricians, midwives, and all those involved in attending childbirth as it is the relationship between these two structures that defines the mechanics of normal and abnormal childbirth.
From an obstetric view, the fetal skull is the largest and least compressible part of the fetus that has to pass through the birth canal and is usually the presenting part during labour. The pelvis supports the gravid uterus after the first trimester and is the canal through which a fetus must pass if labour is to be successful.Fetal skull
This consists of the two parietal, frontal, and temporal bones. In addition, there is the occipital bone that is attached to the cervical vertebrae (Figure 3.8). In the fetus, the bones of the skull have not yet fused and are separated by spaces called sutures and fontanelles (Figure 3.8).
There are four named sutures of the skull. The frontal suture represents the space between the two frontal bones at the front of the head and the sagittal suture joins the two parietal bones (Figure 3.8). The coronal suture is the space between the frontal and parietal bones. The lambdoid suture is the space between the parietal and occipital bones.
The two areas where the sutures join are called fontanelles (Figure 3.8). The anterior fontanelle is the junction between the frontal, coronal, and sagittal sutures and is diamond shaped. It is also known as the bregma. The posterior fontanelle is the junction between the sagittal and lambdoid sutures and is triangular in shape. It is also known as the lambda.
Clinical considerations
Understanding the bones, fontanelles, and sutures of the fetal skull helps identify normal and abnormal presentation during labour (see Chapters 26 and 32).
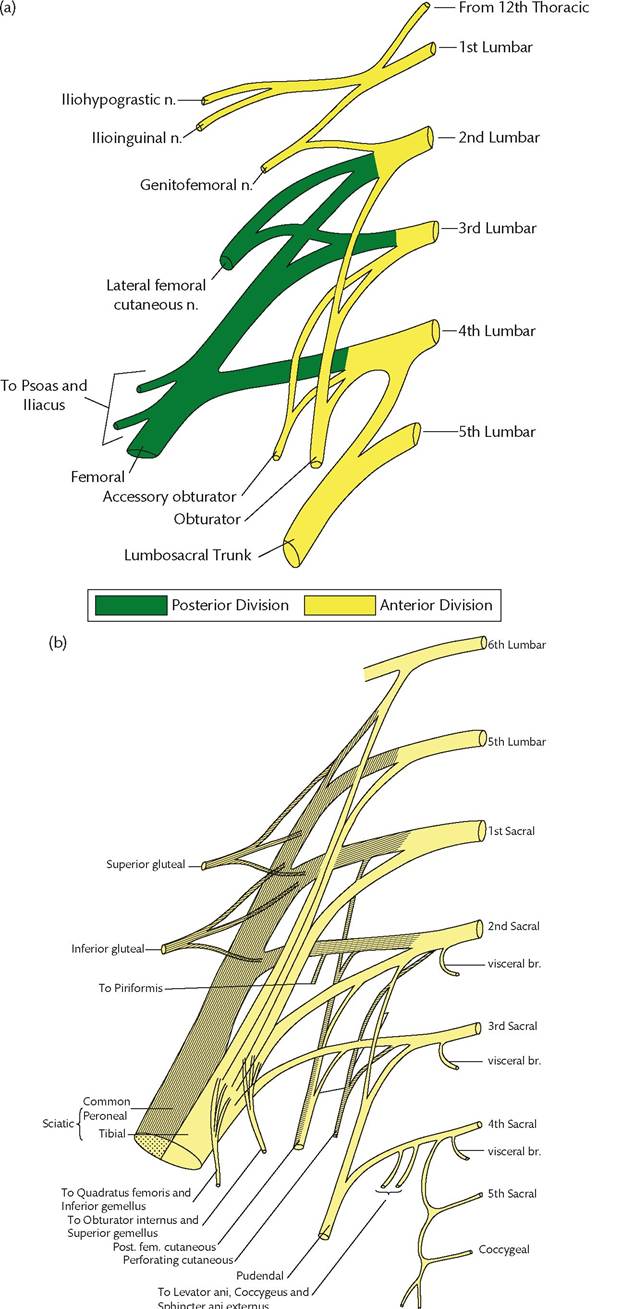
Box 3.6 Nerves of the sacral plexus
• L4 and S1: superior gluteal nerve
• L4-S3: sciatic nerve
• L5-S1: nerve to quadratus femoris
• L5-S2: inferior gluteal nerve
• L5-S2: nerve to obturator internus
• S1-S2: nerve to pyriformis
• S1-S3: posterior femoral cutaneous nerve
• S2-S4: pudendal nerve
• S2-S4: nerve to the external anal sphincter
• S2-S4: pelvic splanchnic nerves
• S3 and S4: nerve to levator ani
• S3 and S4: nerve to coccygeus muscle
The normal presentation is the vertex, which is the area midway between the anterior and posterior fontanelles.
This can be defined on vaginal examination in labour by palpating the fontanelles and bones. When the posterior fontanelle and occipital bones are anterior, this is defined as being ‘occiput anterior’. When there is a malpresentation in the head may be rotated and the position be ‘occiput posterior’ with the anterior fontanelle in the anterior position (Figure 3.8) (see Chapter 32).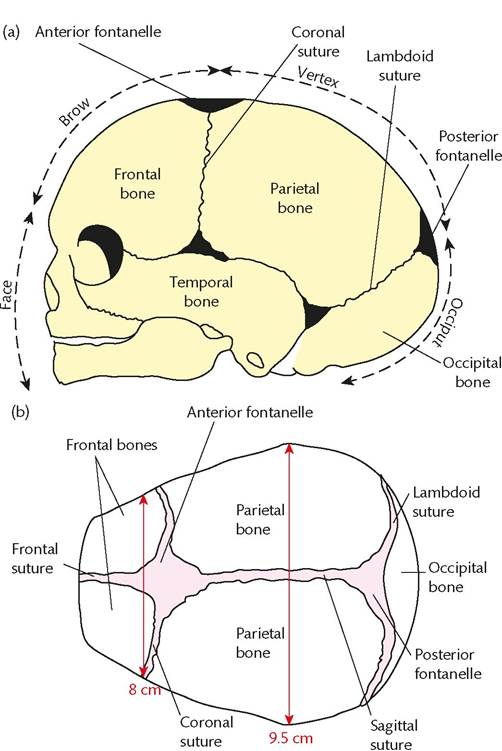
The occiput is the area between the base of the skull and the posterior fontanelle. The brow is the area between the anterior fontanelle and the upper part of the orbits. The face extends from the orbits to the chin. An occipital, brow, or face presentation of the fetus during labour may cause failure to progress (see Chapter 32).
Pelvic bones
These consist of pairs of tightly fused bones (ilium, pubic bone, and ischium) (Figure 3.9a). These are joined together medially and posteriorly by the sacrum and anteriorly in the midline by the pubic symphysis (Figure 3.9a). The bony pelvis in a woman is different to that in the male to accommodate childbirth. The differences are detailed in Box 3.7. In summary, the female pelvis is wider compared to the male pelvis with smaller protuberances (e.g. ischial spines).
The ilium is the largest bone in the pelvis and consists of two parts, the ala and the body (Figure 3.9a). The ala is the large wing that forms part of the greater pelvis. The upper surface of the ala is called the iliac crest which has a spinous process at the front called the Anterior Superior Iliac Spine (ASIS). The two ASISs can be palpated as bony protuberances either side of the lower abdomen and are the lateral- most extremity of the inguinal ligaments on each side. The body of the ilium extends into the acetabulum of which it forms about two-fifths.
The ischium is the most inferior part of the pelvic bones and has a spine (ischial spine) that projects inwards (Figure 3.9a).
This spine can be palpated on vaginal examination and is the constant position against which the descent of the fetal head is measured. The distance between the two ischial spines is the narrowest part of the pelvis through which a fetus must pass during normal labour.The two pubic bones lie at the front and are joined together by the pubic symphysis, which is a cartilaginous joint (Figure 3.9a). During pregnancy, a hormone called relaxin is produced by the placenta. Relaxin helps loosen this joint, allowing some separation during labour.
Pelvic inlet
The pelvic inlet is also termed the pelvic brim. It is bounded posteriorly by the sacral promontory and anteriorly by the superior pubic rami and symphysis pubis. Laterally it is bounded by the iliopectineal lines. The transverse diameter is about 13.5 cm. The shortest diameter and the one most important clinically is that between the sacral promontory and symphysis pubis, which is about 11.5 cm. It is for this reason that, during labour, the fetal head normally passes
Box 3.7 Characteristics of the female pelvic bones compared to those of the male
• Larger and broader
• Inlet oval shaped compared to heart shaped
• Angle of the pubic arch is obtuse (about 100 degrees) compared to acute (about 70 degrees) in men
• Greater sciatic notch is wider
• Smaller ischial spines
• Smaller ischial tuberosities
• Sacrum has less pronounced promontory
• Sacrum is smaller
• Sacrum is more curved
• Acetabula are wider apart and more medial
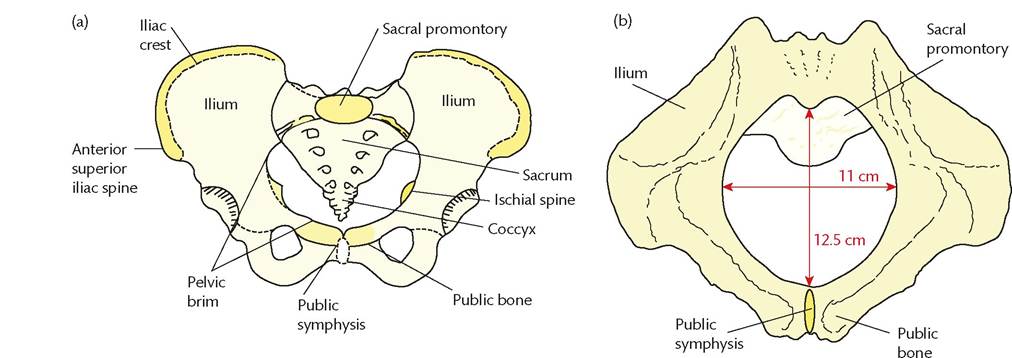
Figure 3.9 Female pelvis, pelvic inlet, and pelvic outlet.
through the pelvic inlet in a left or right Occipitolateral position (see Chapter 32).
Pelvic cavity
The pelvic cavity is bounded superiorly by the zone of inlet (see Figure 3.9) and inferiorly by the outlet (see Figure 3.9). This contains the zone of cavity (plane of greatest dimensions) and the zone of mid pelvis (plane of least dimensions).
The zone of cavity has an anteroposterior and transverse diameter of about 13 cm and extends from the inlet to the junction of the second and third sacral vertebrae. It is within this cavity that the fetal head rotates from an occipitolateral to an occipitoanterior position.
The mid pelvis extends anteroposteriorly between the pubic symphysis and the bottom of the sacrum. The transverse diameter is that between the two ischial spines and this is the narrowest part of the pelvic space, measuring about 10 cm. During labour, the ischial spines are the anatomical position most likely to cause an obstruction. The presentation of the fetal head in relation to the ischial spines can be palpated vaginally during labour and is often used as a measure of progress.
Pelvic outlet
The pelvic outlet is diamond shaped with the tip of the sacrum and sacrotuberous ligaments posteriorly (Figure 3.9b) and the area under the pubic arch anteriorly. The anteroposterior diameter is about 12.5 cm (Figure 3.9b). The transverse diameter of the pelvic outlet is measured between the two ischial tuberosities and is about 11 cm. The narrower transverse diameter is the reason that during childbirth the baby is usually delivered through an occipitoanterior position (see Chapter 26).
Clinical variations
The typical female pelvis is described as gynaecoid. A gynaecoid pelvis has a round pelvic inlet, short ischial spines, and a shallow pelvic cavity that allows for rapid childbirth.
An anthropoid pelvis has an oval-shaped inlet and a smaller transverse diameter comparative to its anteroposterior diameter. It is for this reason that it favours an occiput-posterior position in labour that may lead to a failure to progress. An anthropoid pelvis is more common in African women, but is also found in a significant proportion of Caucasian women. It can be associated with an additional lumbar vertebra and this is called a high assimilation pelvis.
An android pelvis has a heart-shaped inlet and is narrower from front to back. This shape is more associated with the male pelvis than the female (Box 3.7) and it is for this reason that women with an android pelvis often have more problems with childbirth.
A platypelloid pelvis has a narrower anteroposterior diameter compared to its transverse. Due to the position of the sacral promontory, the inlet is slightly kidney shaped. This shape results in difficulty for a fetal head to engage but normally allows for easy childbirth thereafter.