Pneumonia
Lower respiratory tract infections are a leading cause of maternal and fetal morbidity and mortality (8). Pneumonia is the commonest reason for antenatal admission to critical care units (9).
The reported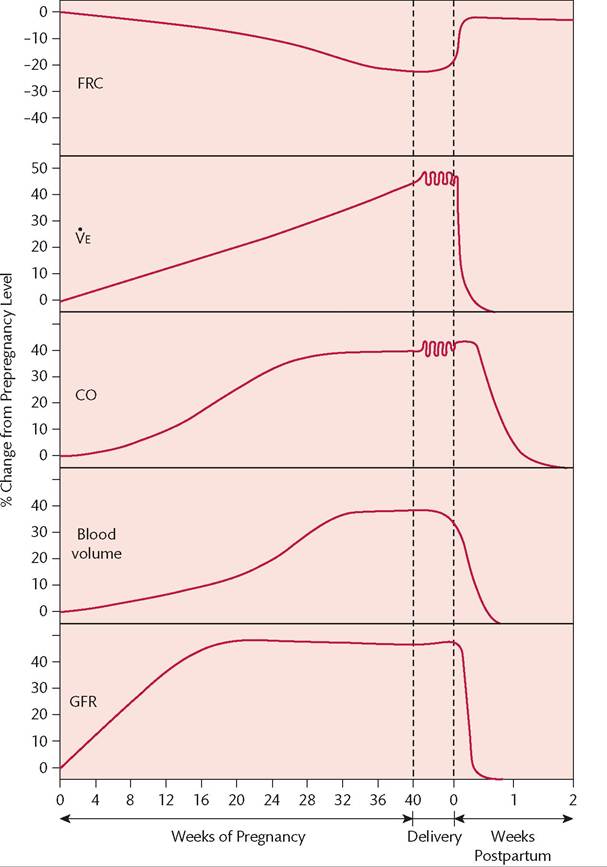
Figure 25.1 Physiological changes occurring during pregnancy and the postpartum period. CO, cardiac output; FRC, functional residual capacity; GFR, glomerular filtration rate; Ve, minute ventilation.
Reproduced with permission from the American Thoracic Society. Copyright © 2016 American Thoracic Society. Lapinsky SE et al, 1995; AmJ Respir Crit Care Med 152:427-455.
incidence is probably not higher than that in the general population. Pneumonia in pregnancy is due to the usual bacterial pathogens such as Streptococcus pneumoniae, Haemophilus influenzae, and Mycoplasma pneumoniae but the pregnant woman is at increased risk of complications such as respiratory failure and empyema (10). Due to alterations in cell-mediated immunity in pregnancy, pregnant women are at increased risk of developing severe respiratory disease related to some viral infections, particularly influenza and varicella infection. Critical illness and mortality from influenza in pregnant women is more common than in the general population (11). Varicella infection is more severe in adults than children, likely even more so during pregnancy. Coccidioidomycosis may produce more severe disease than in non-pregnant patients, related to impairment of cell-mediated immunity and to a stimulatory effect of progesterone and 17-β (β)-oestradiols on fungal proliferation (12).
Pneumocystis jirovecii pneumonia may be seen in HIV-positive patients, and has a more aggressive course during pregnancy (13). Pregnancy does not affect the course or incidence of reactivation of tuberculosis.
Postpartum pneumonia occurs in the first 6 weeks after delivery and is more common after caesarean section (14).Pneumonia increases the risk of preterm labour, as well as the incidence of small-for-gestational age infants and intrauterine and neonatal death rates (8). Chronic illness in the mother is a predictor of adverse outcome in both fetus and mother. Although pneumonia is associated with an increased risk of maternal mortality, this may be attributable to the presence of predisposing underlying diseases rather than to the pneumonia itself.
The diagnosis of pneumonia is often delayed because of reluctance on the part of physicians or patients to obtain a chest radiograph. The radiation risk to the fetus of a posteroanterior radiograph performed with abdominal screening is negligible, exposing the fetus to less than 1 mrad (0.01 mGy) (15). A lateral chest radiograph produces greater exposure but is usually not required. The risk to both fetus and mother of delaying the diagnosis exceeds any risk of this very small radiation dose.
Treatment of pneumonia in pregnancy is not very different to the non-pregnant patient. Community-acquired pneumonia may be treated with a β-lactam antibiotic (e.g. amoxicillin, ceftriaxone) with or without coverage for atypical pneumonias (e.g. clarithromycin, azithromycin). Tetracyclines (including doxycycline) are usually avoided in pregnancy as are quinolones (ciprofloxacin, moxifloxacin), although the risk for the latter is relatively low. Pregnant women should receive the inactivated influenza vaccine and if disease occurs, treatment with oseltamivir, zanamivir, or amantadine are acceptable during pregnancy. Varicella pneumonitis should be treated with aciclovir, which has not been associated with fetal anomalies, and decreases mortality (16). Susceptible pregnant women exposed to varicella should be evaluated for use of varicella zoster immune globulin in the same way as the general population. Disseminated coccidioidomycosis is associated with a very high mortality rate, and should be treated with amphotericin (17). P. jirovecii pneumonia is treated with trimethoprim-s ulfamethoxazole with folate supplementation (5 mg daily) (17). Folic acid antagonists and sulpha drugs carry some risks for the fetus, but the alternative, pentamidine, is associated with higher risks for both mother and fetus. Active tuberculosis is treated with isoniazid and rifampin, which have a low risk of adverse fetal effects. Ethambutol is also used initially until sensitivities are available, and pyrazinamide is recommended by some authorities. Contact tracing is important and the baby should receive immunization with bacillus Calmette-Guerin. Treatment of latent tuberculosis (‘prophylaxis') can usually be deferred until after the pregnancy, except in the case of documented skin test conversion and recent exposure.