4 Preconception Counseling and Prenatal Care
William Fletcher
Melissa L. Russo
PRECONCEPTION CARE AND COUNSELING
Preconception care and counseling are important to identify any medical, pharmacologic, behavioral, or social risks to a woman's health and initiate an intervention prior to pregnancy in an effort to reduce the risk of maternal-fetal morbidity and mortality.
The preconception evaluation offers a unique opportunity to inform women of potential infertility or pregnancy issues. Preconception care is especially useful for women who have underlying medical conditions (e.g., diabetes mellitus, phenylketonurics, renal disease), exposure to potential teratogens (e.g., warfarin, isotretinoin), or high-risk behaviors (e.g., smoking or cocaine use). Preconception counseling should emphasize healthy preconception habits and confirm that vaccines are up-to-date. This should be incorporated into routine health care visits for women of childbearing age because approximately half of pregnancies in the United States are unplanned. The following sections will highlight the main areas to address during a preconception evaluation. P.59
Medical Assessment
• Preconception care (Table 4-1) should include a thorough assessment of an individual's medical problems. This is becoming increasingly important as the incidence of obesity-related comorbidities, such as diabetes mellitus and hypertension, increases. These conditions should be as well-controlled as possible prior to conception because they can have significant adverse effects on the developing fetus and adverse effects in the mother. For example, the risk of birth defects increases with hemoglobin A1C level in diabetic patients, with an A1C greater than 10.6% conferring eight times the risk of having a birth defect compared to women with an A1C of less than 8%.
• With maternal medical issues, it is important to discuss the impact on the fetus and the potential for the pregnancy to exacerbate the underlying medical condition.
• With any complex medical condition, expertise from a maternal-fetal medicine specialist is advised and ongoing collaboration with other specialists may be indicated.
Gynecologic and Reproductive History
• The gynecologic and obstetric history may reveal potential factors contributing to infertility or complications in a future pregnancy.
• Discussion of menstrual and contraceptive history provides an educational opportunity for conception counseling and to discuss optimal timing of a pregnancy in a medically complex patient.
• Past history of sexually transmitted infections is important to note because these women may be at increased risk of these infections in a future pregnancy. These infections include Neisseria gonorrhea, Chlamydia trachomatis, Treponema pallidum, genital herpes simplex virus (HSV), and HIV.
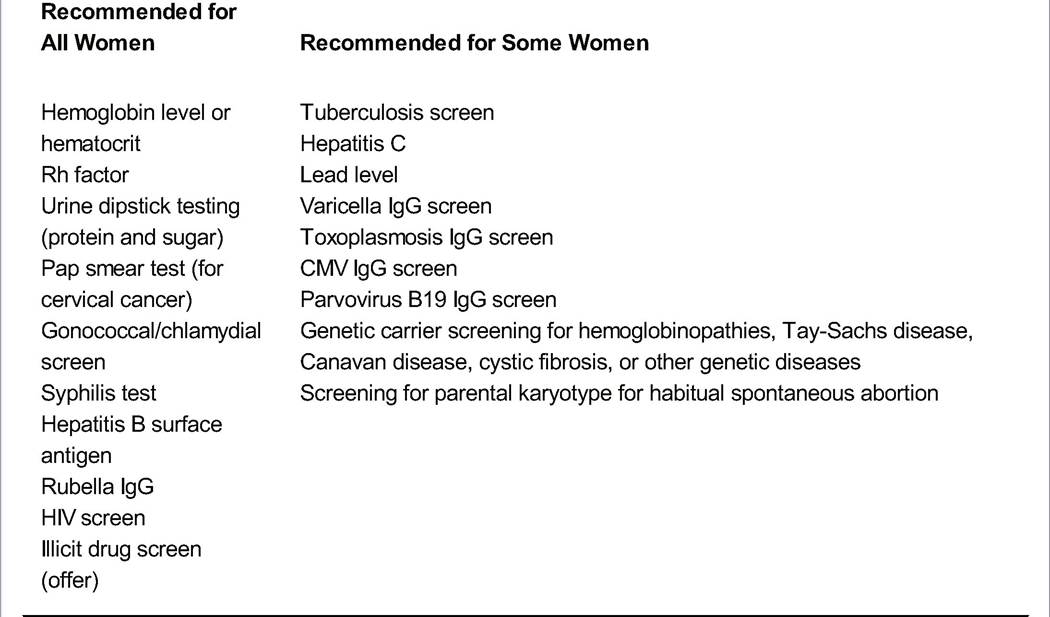
TABLE 4-1 Preconception Risk Assessment: Laboratory Testing
![]()
IgG, immunoglobulin G; CMV, cytomegalovirus. Adapted from U.S. Department of Health and Human Services. Caring for our Future: The Content of Prenatal Care. A Report of the PHS Export Panel. Washington, DC: U.S. Department of Health and Human Services, 1989, with permission.
P.60 With prior poor pregnancy outcomes, the recurrence risk of an adverse outcome should be discussed. In some cases, there are interventions to reduce these risks in a future pregnancy.
Known congenital uterine malformations are important to identify because these conditions can be associated with recurrent pregnancy loss, malpresentation, or preterm birth.
Age
• Advanced maternal age (older than 35 years at time of delivery) is associated with increased risks that include infertility, fetal aneuploidy, gestational diabetes, preeclampsia, and stillbirth.
• Prior to pregnancy, it is important to educate women about these risks and discuss aneuploidy screening and diagnostic tests that are available, as well as management options, if available.
Family History
• A patient's family history can identify genetic risks to a future pregnancy.
• A preconception history includes evaluation for family history of congenital anomalies; chromosomal abnormalities (e.g., Down syndrome); mental retardation/developmental delay; inherited diseases such as hemoglobinopathies, cystic fibrosis, and hemophilia; recurrent pregnancy loss/stillbirth/early infant death in the family; ethnicity; and consanguinity.
• Carrier screening for hereditary disease is traditionally based on ethnic background of the couple and allows counseling before the first potentially affected pregnancy. Early recognition of carrier status informs patients of their risks outside of the emotional context of pregnancy and facilitates educated decisions about reproductive goals and testing during or after pregnancy. Expanded carrier screening is an option for patients, in which over 100 diseases are screened in a single test. Family history can identify those at increased risks for specific diseases, such as muscular dystrophy, fragile X syndrome, or Down syndrome, for which genetic counseling should be offered. Information about diagnostic tests, such as chorionic villus sampling (CVS) or amniocentesis, can be explained. In some instances, genetic counseling may result in a decision to forgo pregnancy or to use assisted reproductive technologies that can decrease this risk.
Medications
Both over-the-counter and prescription drugs, herbs, and supplements should be reviewed. In general, U.S. Food and Drug Administration (FDA) pregnancy categories X and D medications should be avoided or discontinued. For other medications, maternal and fetal risk-benefit should be assessed, with appreciation that in cases maternal risk of not using a specific medicine may outweigh fetal risks of administration. Assistance in answering questions about reproductive toxicology is available through the online database REPROTOX (http://www.reprotox.org). The Reproductive Toxicology Center at Columbia Hospital for Women Medical Center, one of the sponsors of REPROTOX, also offers a clinical inquiry program.
Many states have teratogen hotlines or state-funded programs; the Organization of Teratology Information Specialists (OTIS) is a good source for information about these programs and offers other resources (http://www.otispregnancy.org). • Isotretinoin (Accutane): An oral treatment for severe cystic acne, it is highly teratogenic, causing craniofacial defects (microtia, anotia). It should be discontinued prior to pregnancy.
P.61
• Warfarin (Coumadin) and vitamin K antagonists: Such anticoagulants have been associated with warfarin embryopathy. Because heparins (both unfractionated and low-molecular-weight) do not cross the placenta, women requiring anticoagulation should be encouraged to switch to heparin therapy prior to conception, except in rare cases.
• Antiepileptic drugs (AED): Children born to mothers treated with certain AEDs are at increased risk for congenital malformations, particularly when these drugs are used in the first trimester. Valproic acid is associated with neural tube defects (NTDs); adverse neurocognitive effects; and craniofacial, limb, and cardiac abnormalities. Carbamazepine exposure has been associated with facial dysmorphism and fingernail hypoplasia. Data on newer AEDs are still limited. For women with seizure disorders, it is important to have them on AED regimens with less teratogenicity. Notably, a patient with an unintended pregnancy using an AED should not abruptly discontinue her medication but rather be switched to another medication where possible, due to risk of seizure recurrence. A detailed fetal anatomy sonogram, maternal serum alphafetoprotein (MSAFP), and fetal echocardiogram may provide useful information for these patients.
• Lithium has been associated with increased incidence of heart defects and should only be continued based on the severity and frequency of illness. Fetal echocardiogram is recommended for women taking lithium in the first trimester. Lamotrigine is a mood stabilizer with a significantly better reproductive safety profile than lithium.
It should be considered as an alternative in women with bipolar disorder. • Selective serotonin reuptake inhibitors (SSRIs) are considered safe; however, paroxetine early in pregnancy has been associated with increased risk of heart defects, and an FDA advisory notes an association between late-term SSRI use and persistent pulmonary hypertension in the newborn. SSRI use in pregnancy should be individualized, balancing the risks of maternal depression and potential fetal effects.
Nutritional Assessment
• Folic acid supplementation reduces the risk of NTDs. The U.S. Public Health Service recommends daily supplementation with 0.4 mg of folic acid for all women capable of becoming pregnant. Unless contraindicated by the presence of pernicious anemia, women who have previously had a fetus with an NTD should take 4.0 mg of folic acid daily.
• The body mass index (BMI), defined as (weight in kilograms/[height in meters]2), is the preferred indicator of nutritional status. Very overweight (BMI above 30) and very underweight women (BMI placentae. Cocaine is teratogenic, and its use has been associated with cases of in utero fetal cerebral infarction, microcephaly, and limb reduction defects. Genitourinary malformations have been reported with first-trimester cocaine use. Infants born to women who use cocaine are at risk for neurobehavioral abnormalities and impairment in orientation and motor function.
• Opiates: Opiate use is associated with increased rates of stillbirth, fetal growth restriction, prematurity, and neonatal mortality, perhaps due to risky behaviors in opiate substance abusers. Methadone treatment is associated with improved pregnancy outcomes. Neonates born to narcotic addicts are at risk for a severe, potentially fatal, narcotic withdrawal syndrome. Although the incidence of clinically significant withdrawal is slightly lower among methadone-treated addicts, its course can be just as severe. Neonatal withdrawal is characterized by a high-pitched cry, poor feeding, hypertonicity, tremors, irritability, sneezing, sweating, vomiting, diarrhea, and, occasionally, seizures.
Frequent sharing of needles has resulted in high rates of HIV infection (>50%) and hepatitis among intravenous narcotic addicts. • Amphetamines: Crystal methamphetamine, a potent stimulant that is inhaled, injected, or snorted, has been associated with decreased fetal head circumference and increased risk of abruptio placentae, IUGR, and fetal death in utero. However, no proven teratogenicity exists.
• Hallucinogens: No evidence proves that lysergic acid diethylamide (LSD) or other hallucinogens cause chromosomal damage, as was once reported. Few studies exist on the possible deleterious effects of maternal hallucinogen use during pregnancy. No proven teratogenicity to LSD exists.
Social History
A social and lifestyle history should be obtained to identify risky behaviors and exposures that may compromise reproductive outcome. Social, financial, and psychological issues that could affect pregnancy planning can also be identified.
• Domestic violence: Women are more likely to be abused during pregnancy than at other times. Approximately 37% of abused women are assaulted during their pregnancy, resulting in possible abruptio placentae, antepartum hemorrhage, fetal
P.64 fractures, rupture of the internal organs, and preterm labor. Information about community, social, and legal resources should be made available to women who are abused and a plan devised for dealing with the abusive partner. See Chapter 33.
• Insurance coverage and financial difficulties: Many women and couples do not know the eligibility requirements or amount of maternity coverage provided by their insurance carriers or may lack medical insurance coverage altogether. Referral for medical assistance programs should be part of preconception planning as needed.
GENETIC COUNSELING AND TESTING
Genetic Counseling
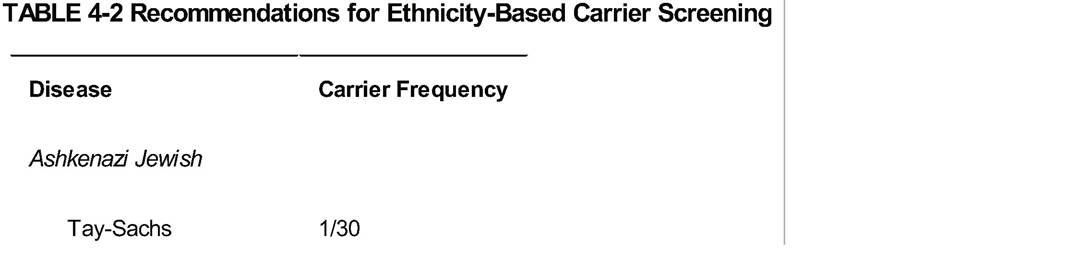
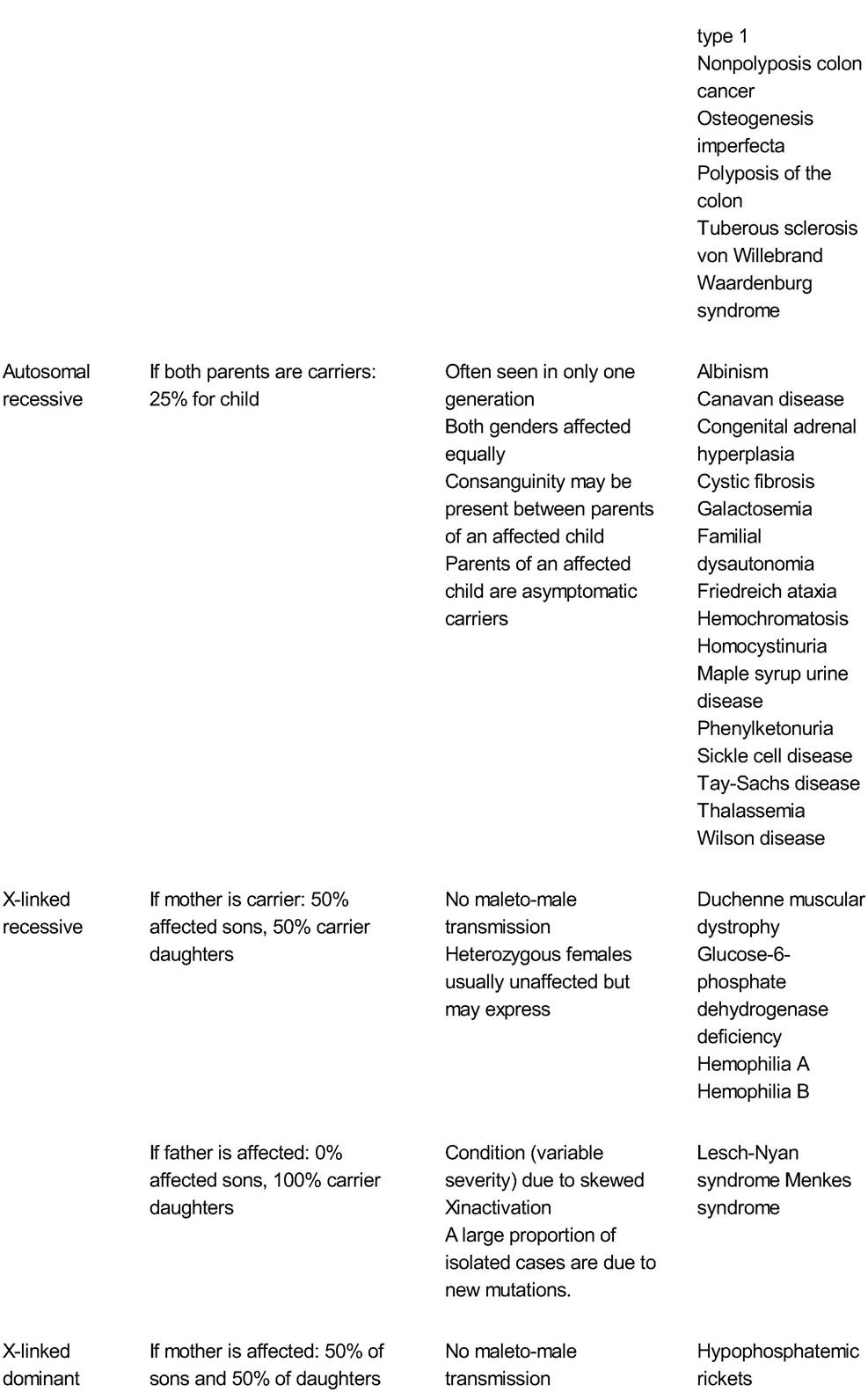
Genetic counseling, risk assessment, and intervention are based on the family history of the biologic mother and father, maternal age, ethnicity, drug or environmental exposures, and medical and obstetric history (Tables 4-2 and 4-3). Information on hereditary birth defects is best assessed with a three-generation pedigree. Table 4-4 describes major modes of inheritance.
• Assisted reproductive technologies, such as donor egg and sperm, sperm sorting, and preimplantation genetic diagnosis (PGD), may obviate the risk in specific cases. Adoption and avoidance of pregnancy represent other choices. CVS and amniocentesis permit early diagnosis, facilitate preparation for the care of an affected child, and give the option for pregnancy termination.
![]()
![]()
TABLE 4-3 Indications for Genetic Counseling
Mother 35 years or older at her estimated date of delivery
Fetal anomalies detected via ultrasonography
Abnormal first-trimester serum/nuchal translucency screening
Abnormal triple/quad screening or abnormal alpha-fetoprotein test results
Parental exposure to teratogens
Drugs
Radiation
Infection
Family history of genetic disease (includes chromosome, single gene, and multifactorial disorders)
Birth defects
Mental retardation
Cancer, heart disease, hypertension, diabetes, and other common conditions (especially when onset occurs at an early age)
Membership in ethnic group in which certain genetic disorders are frequent when appropriate screening for or prenatal diagnosis of the disease is available (e.g., sickle cell anemia, Tay-Sachs disease, Canavan disease, thalassemia)
Consanguinity
Reproductive failure
Infertility
Repeated spontaneous abortions
Stillbirths and neonatal deaths
Infant, child, or adult with the following:
Dysmorphic features
Developmental and/or growth delay
Ambiguous genitalia or abnormal sexual development
• In general, prenatal screening involves three groups: the general pregnant population, patients with a specific ethnic background or positive family history for a genetic disorder, and patients with a fetal anomaly. The National Society of Genetic Counselors (NSGC) urges caution regarding prenatal testing for adult-onset conditions unless there are treatments or preventive measures that can be initiated during pregnancy or in early childhood.
Prenatal Genetic Screening
Aneuploidy refers to any condition in which there are an abnormal number of chromosomes. Normally, 46 chromosomes (23 pairs) are found in every somatic cell of the body. Regardless of the maternal age, aneuploidy screening (Table 4-5) should be offered to all women before 20 weeks' gestation. Women who do not seek prenatal care until the second trimester should be offered quadruple screening and ultrasound assessment. Women seen in the first trimester should be offered first-trimester serum and nuchal translucency screening or an integrated approach combining first- and second-trimester screening.
P.66
P.67
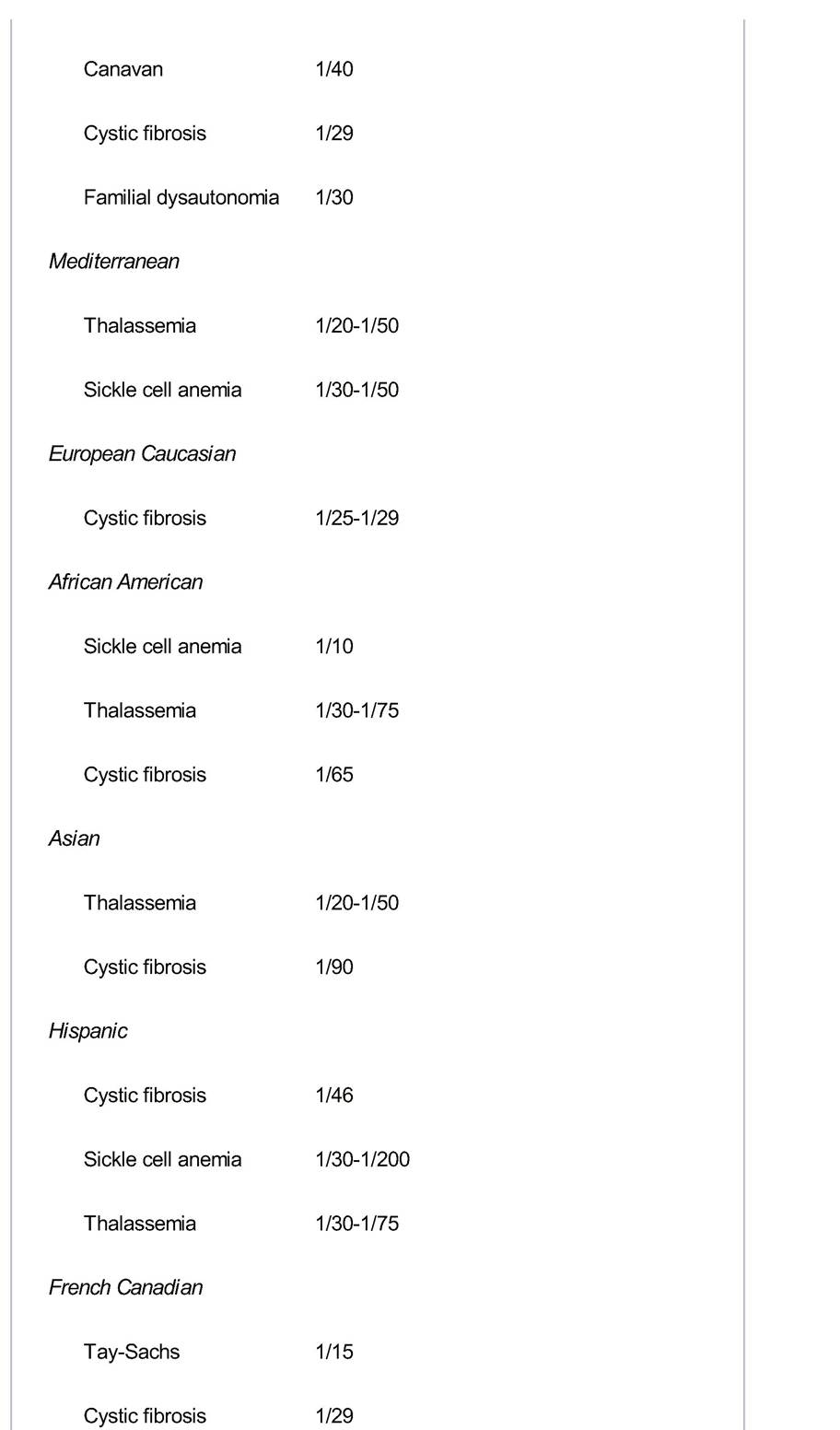
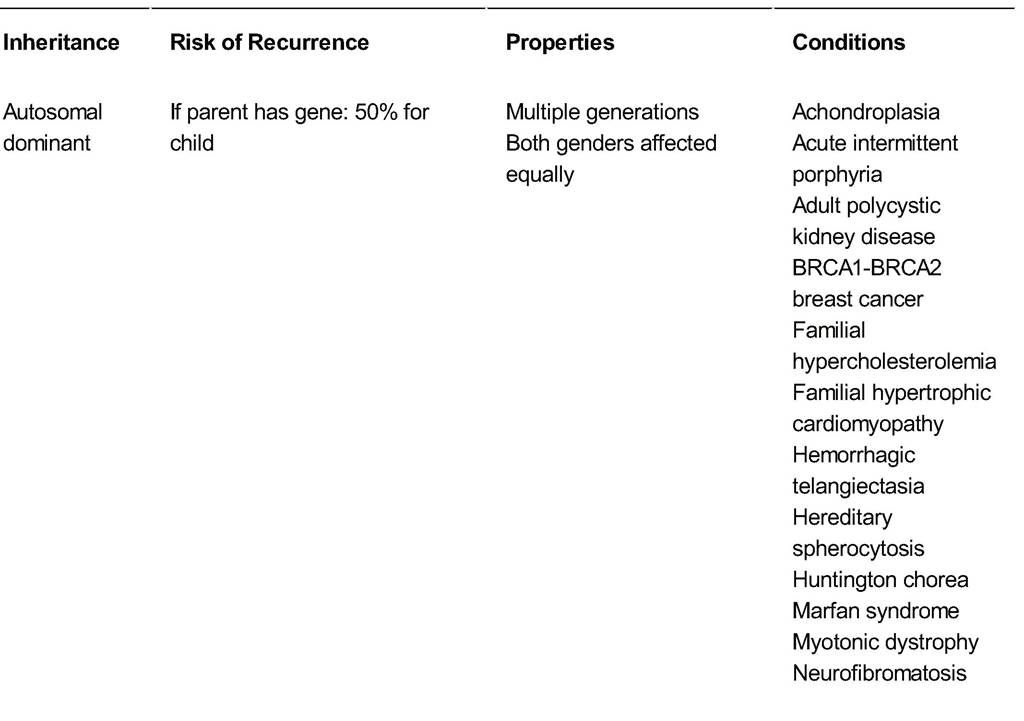
TABLE 4-4 Major Modes of Inheritance
![]()
![]()
![]()
BRCA1, breast cancer 1 gene; BRCA2, breast cancer 2 gene; MELAS, mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke syndrome.
P.68
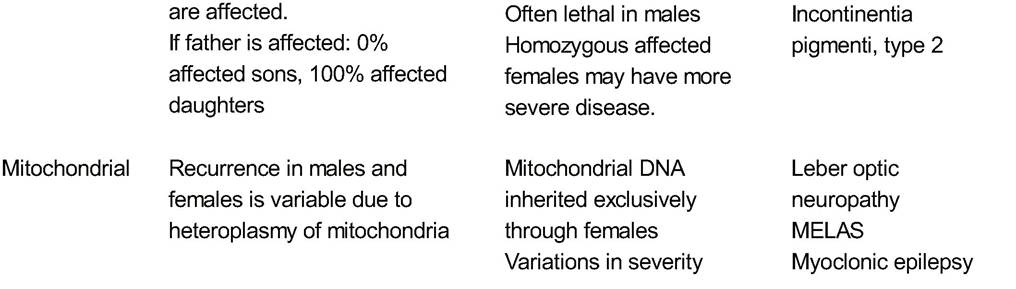
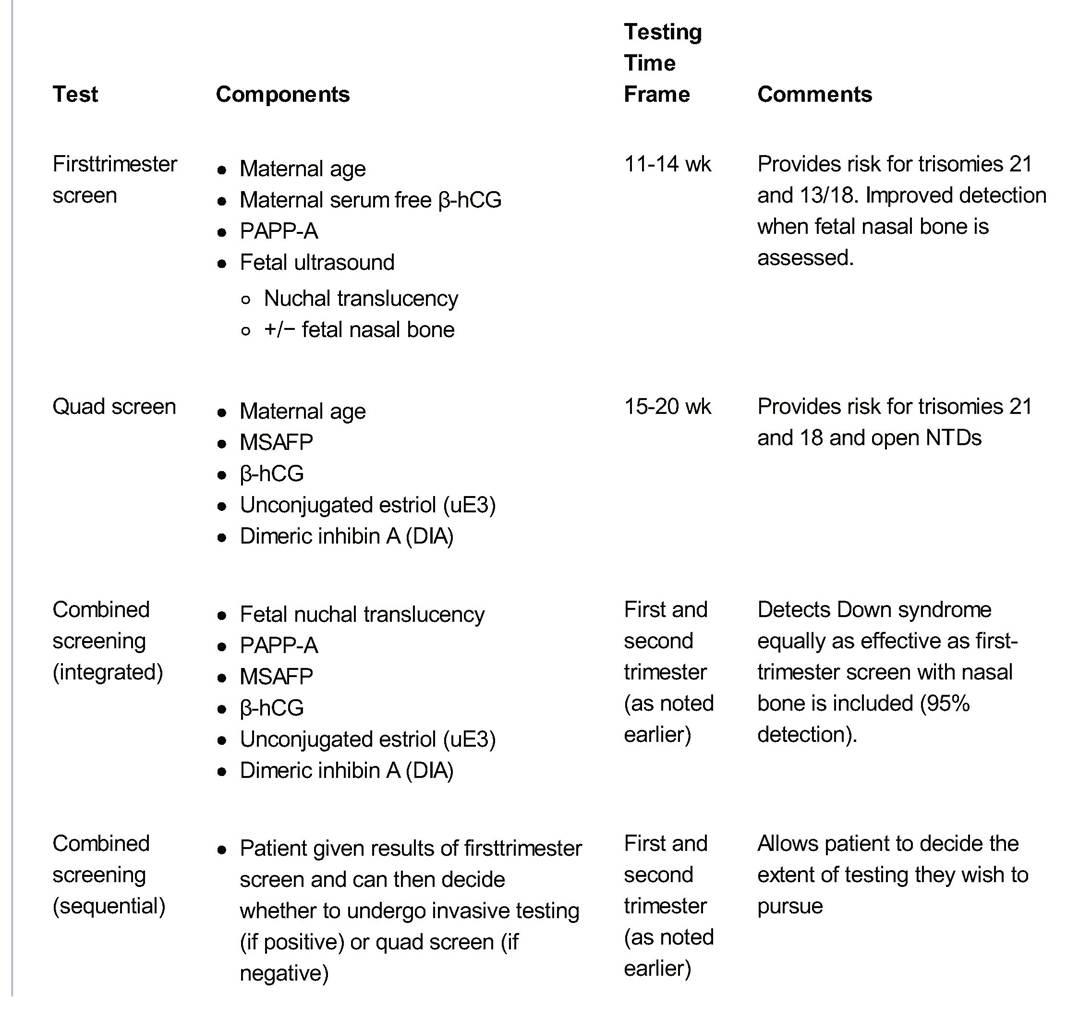
TABLE 4-5 Summary of Prenatal Genetic Screening Tests
![]()
| MSAFP | • Maternal serum alpha-fetoprotein | Second trimester | Provides risk for open neural tube defects |
| Cell-free fetal DNA analysis | • Maternal blood draw with analysis of fetal DNA | 10-20 wk | Only recommended for patients at high risk of aneuploidy |
β-hCG, beta-human chorionic gonadotropin; PAPP-A, pregnancy-associated plasma protein-A; MSAFP, maternal serum alpha-fetoprotein; NTD, neural tube defect.
P.69
• Trisomy 21 (Down syndrome), the most common aneuploid condition in live borns, is the result of an extra chromosome 21. T risomy 21 most often results from meiotic nondisjunction during maternal chromosomal replication and division. It is characterized by mental retardation, cardiac defects, hypotonia, and characteristic facial features. Although its incidence increases with maternal age (Table 4-6), 70% of cases occur in women younger than 35 years because most pregnancies occur in these younger women.
TABLE 4-6 Chromosomal Abnormalities in Livebornsa border=0>
| Maternal Age | Risk of Down Syndrome | Total Risk of Chromosomal Abnormalitiesa |
| 20 | 1:1,667 | 1:526 |
| 21 | 1:1,667 | 1:526 |
| 22 | 1:1,429 | 1:500 |
| 23 | 1:1,429 | 1:500 |
| 24 | 1:1,250 | 1:476 |
| 25 | 1:1,250 | 1:476 |
| 26 | 1:1,176 | 1:476 |
| 27 | 1:1,111 | 1:455 |
| 28 | 1:1,053 | 1:435 |
| 29 | 1:1,000 | 1:417 |
| 30 | 1:952 | 1:385 |
| 31 | 1:909 | 1:385 |
| 32 | 1:769 | 1:322 |
| 33 | 1:602 | 1:286 |
| 34 | 1:485 | 1:238 |
| 35 | 1:378 | 1:192 |
| 36 | 1:289 | 1:156 |
| 37 | 1:224 | 1:127 |
| 38 | 1:173 | 1:102 |
| 39 | 1:136 | 1:83 |
| 40 | 1:106 | 1:66 |
| 41 | 1:82 | 1:53 |
| 42 | 1:63 | 1:42 |
| 43 | 1:49 | 1:33 |
| 44 | 1:38 | 1:26 |
| 45 | 1:30 | 1:21 |
| 46 | 1:23 | 1:16 |
| 47 | 1:18 | 1:13 |
| 48 | 1:14 | 1:10 |
| 49 | 1:11 | 1:8 |
aKaryotype 47, XXX was excluded for ages 20 to 32 years (data not available).
Adapted from Hook EB, Cross PK, Schreinemachers DM. Chromosomal abnormality rates at amniocentesis and in live-born infants. JAMA 1983;249:2034-2038, with permission; Hook EB. Rates of chromosomal abnormalities at different maternal ages. Obstet Gynecol 1981 ;58:282-285, with permission.
• Trisomy 13 (Patau syndrome) and 18 (Edward syndrome) are more severe disorders that cause profound mental retardation and severe multiorgan birth defects. Few babies with trisomy 13 or 18 survive more than a few months. The risk of trisomy recurrence for a Chromosomally normal couple is often cited to be 1%.
First-Trimester Screening
• First-trimester screening, performed between 11 and 14 weeks, includes maternal age, nuchal translucency, maternal serum free beta-human chorionic gonadotropin (free β-hCG), and pregnancy- associated plasma protein-A (PAPP-A).
• The detection rate for Down syndrome and trisomy 18 is about 89% and 95%, respectively, with a 5% falsepositive rate.
• First-trimester screening with ultrasound assessment of the nasal bone (absent in about 70% of trisomy 21 fetuses) improves the detection rate for Down syndrome to approximately 95% with a 5% false-positive rate.
• First-trimester screening does not screen for open NTDs.
Second-Trimester Screening
• Second-trimester quad screening is performed between 15 and 20 weeks and estimates risk for Down syndrome, open NTDs, and trisomy 18. It uses MSAFP, β-hCG, unconjugated estriol (uE3), and dimeric inhibin A (DIA), combined with maternal age.
• The detection rate for trisomy 21 is approximately 75% for women younger than 35 years old and 90% for those older than 35 years. Additionally, abnormal values on this screening (elevated alpha-fetoprotein [AFP] and/or hCG) correlate with an increased risk of perinatal complications.
Combined Screening
Combined screening uses combined first- and second-trimester screening to adjust a woman's age-related risk for a fetus with Down syndrome.
• Integrated screening uses nuchal translucency and PAPP-A from the first-trimester screening and MSAFP, estriol, hCG, and inhibin A from the second-trimester screening. Results are reported only after both screening tests are completed. The detection rate for this method is 94% to 96% with 5% false positives; this is equivalent to first-trimester screening when nasal bone is included in the risk assessment.
• Sequential screening is where the patient is given the first-trimester results. If at high risk, patients are given the option for invasive testing, whereas those at low risk can still undergo second-trimester screening to achieve a higher detection rate.
Cell-Free Fetal DNA Screening
• Cell-free fetal DNA can be found in maternal circulation in increasing quantity as pregnancy progresses.
• Clinical testing of this DNA has recently become available and is currently only recommended for patients at increased risk of aneuploidy and should not be considered routine screening.
• Screening can be performed for trisomies 21, 13, and 18 as early as 10 weeks' gestation by determining the relative amount of fetal DNA from various fetal chromosomes.
• This form of screening has been found to detect over 98% of trisomies 21 and 18 pregnancies with a very low false-positive rate of less than 0.5%.
• High-risk patients include women with advanced maternal age, sonographic findings suggesting increased risk of aneuploidy, history of trisomy in a prior pregnancy, and a prior screening test suggesting an increased risk of aneuploidy.
P.71
• As with the other forms of prenatal genetic screening, patients with a result indicating an increased risk of aneuploidy should be offered diagnostic testing because results are not considered diagnostic due to screening imperfections.
Screening for Neural Tube Defects
• NTDs result from a failure of the neural tube to close or attain its normal musculoskeletal coverings in early embryogenesis. Among the most common major congenital malformations with an incidence of 1 to 2 in 1,000 live births, NTDs include the fatal condition of anencephaly as well as spina bifida (meningomyelocele and meningocele); most have the potential for surgical correction.
• Family history of NTD increases risk. If one partner has an NTD, the recurrence risk is 2% to 3%. In a couple with a previously affected child, the risk of recurrence is also 2% to 3%. Ninety percent of NTDs, however, occur in families without such histories. All pregnant women should be offered NTD screening.
• MSAFP is a fetal glycoprotein synthesized sequentially in the embryonic yolk sac, gastrointestinal (GI) tract, and liver. Normally, AFP crosses the placenta to appear in the mother's blood. In addition, a small amount of AFP enters the amniotic fluid via fetal urination, GI secretions, and transudation from exposed blood vessels. The concentration of AFP in amniotic fluid (amniotic fluid alpha-fetoprotein [AFAFP]) is highest at the end of the first trimester and slowly declines during the remainder of pregnancy. MSAFP concentrations, on the other hand, rise until approximately 30 weeks' gestation.
• With an open fetal NTD or an abdominal wall defect, increased AFP more than 2.5 multiples of the median (MoM) will be detected in amniotic fluid in over 95% of cases and in the mother's blood in about 80% of cases.
• Elevated MSAFP levels can also occur with incorrect pregnancy dating, multiple pregnancies, congenital hereditary nephrosis, Turner syndrome with cystic hygroma, fetal bowel obstruction, teratomas, IUGR, and fetal death.
• Women who elected to undergo first-trimester screening or have a normal result from CVS should still be offered NTD screening with an MSAFP in the second trimester.
• Diagnostic ultrasonography should be performed on patients with elevated MSAFP screening results to confirm gestational age, as well as to visualize the placenta, detect multiple pregnancies, and detect any fetal anomalies.
• Assignment of incorrect gestational age may lead to incorrect interpretation of AFP levels because both MSAFP and AFAFP levels change in relation to gestational age. Maternal smoking is also associated with false-positive elevations in MSAFP.
Prenatal Diagnostic Testing
• In the United States, it is standard to offer CVS or amniocentesis to women who will be 35 years or older when they give birth, due to inherent age-associated risks.
• CVS uses either a catheter (transcervically) or a needle (transabdominally) to biopsy placental tissue derived from the same fertilized egg as the fetus.
• CVS is usually performed at 10 to 13 weeks' gestation but transabdominal CVS may be performed throughout the second or third trimester.
• CVS offers the psychological and medical advantages of early diagnosis and possibility for first-trimester termination.
• When adjusted for confounding factors, such as gestational age and early spontaneous miscarriage rate, the CVS-related miscarriage rate is not statistically different from that for second-trimester amniocentesis.
P.72
• Unsensitized Rh-negative women should be given Rh immunoglobin after CVS.
• Cytogenetically ambiguous results caused by maternal cell contamination or mosaicism are reported more often after CVS than after amniocentesis. In such instances, follow-up amniocentesis may be required to clarify results, which increases both the total cost of testing and the risk of miscarriage.
• Reports of infants born with limb defects after CVS were first published in 1991. This outcome is associated with gestational age, and therefore, CVS is not generally recommended before 9 weeks' gestation.
• Amniocentesis aspirates a small amount of amniotic fluid, containing cells that are shed from the fetal bladder, skin, GI tract, and amnion, and these cells can be used for karyotyping or other genetic testing.
• Amniocentesis is most commonly performed at 15 to 18 weeks' gestation.
• Patients with an obstetric history of NTD should be counseled about their 2% to 3% risk of recurrence and offered second-trimester amniocentesis for AFP testing as well as detailed ultrasonographic evaluation of fetal anatomy at 18 to 20 weeks' gestation.
• The amniocentesis site should be selected carefully, avoiding the placenta if possible, as contamination with fetal blood will falsely elevate the AFAFP. Falsepositive results due to contamination with fetal blood can be identified by acetylcholinesterase testing (absent in pregnancies for which the elevated AFAFP can be explained by contamination with fetal blood).
• The miscarriage rate from midtrimester (16 to 20 weeks) amniocentesis is estimated to be 1 in 200 to 500. Other complications such as vaginal spotting or amniotic fluid leakage occur infrequently; most are transient.
• Unsensitized Rh-negative women should be given Rh-immune globulin after amniocentesis.
• Midtrimester ultrasonographic evaluation at 18 to 22 weeks' gestation should include a systematic fetal anatomy survey and growth assessment.
• Ultrasound screening for Down syndrome, also called age-adjusted ultrasound risk assessment (AAURA), uses likelihood ratios associated with specific markers to adjust a woman's a priori risk.
• AAURA screening includes thickened nuchal fold, echogenicity of the fetal bowl, short humerus and femur lengths, dilated renal pyelectasis, and intracardiac echogenic focus.
• Although helpful, an ultrasound cannot diagnose Down syndrome with certainty.
• Ultrasonography is better at detecting aneuploidies other than Down syndrome, such as trisomy 18 or trisomy 13, which are associated with a higher incidence of major structural anomalies.
ROUTINE PRENATAL CARE
Establishment of Expected Date of Confinement The gestational dating of a pregnancy is very important to establish at the first prenatal visit because this can later play an important role in management of a pregnancy and can impact plans for delivery. The average duration of human pregnancy is 280 days from the first day of the last menstrual period (LMP) until delivery. The 40-week gestational period is based on menstrual weeks (not weeks since conception), assuming ovulation and conception on the 14th day of a 28-day cycle.
• Clinical dating using Naegele’s rule: The estimated date of delivery is calculated by subtracting 3 months from the first day of the LMP then adding 1 week.
P.73
TABLE 4-7 Accuracy of Pregnancy Dating by Ultrasonography According to Gestational Age
| Gestational Age (wk) | Ultrasonographic Measurements | Accuracy |
| 28 | BPD/HC/Fl/AC | ±3 wk |
CRL, crown-rump length; BPD, biparietal diameter; HC, head circumference; Fl, femur length. ; AC, abdominal circumference
• Doppler ultrasonography allows detection of fetal heart tones by 11 to 12 weeks' gestation.
• Ultrasonographic dating is most accurate from 7 to 11-6/7 weeks of gestation. If LMP dating is consistent with ultrasonographic dating within the established range of accuracy for ultrasonography (Table 4-7), the estimated date of delivery is based on LMP.
• A fetoscope can enable detection of heart tones at 19 to 20 weeks' gestation. Quickening (maternal detection of fetal movement) is noted at approximately 19 weeks in the first pregnancy; in subsequent pregnancies, it is usually noted approximately 2 weeks earlier.
Nutrition and Weight Gain
• Pregnant women require 15% more calories than nonpregnant women, usually 300 to 500 kcal more per day, depending on the patient's weight and activity.
• Dietary allowances for most vitamins and minerals increase with pregnancy and are adequately supplied in a well-balanced diet.
• Iron is needed for both the fetus and the mother. Consumption of iron-containing foods should be encouraged, and iron supplements may be prescribed. The 30-mg daily elemental ferrous iron supplement is contained in approximately 150 mg of ferrous sulfate, 300 mg of ferrous gluconate, or 100 mg of ferrous fumarate.
• Prenatal calcium requirement is 1,200 mg/day.
• The recommended weight gain for pregnancy is based on the prepregnancy BMI and has been established by the Institute of Medicine.
• The total weight gain recommended is 25 to 35 pounds for women with a normal BMI. Underweight women may gain 28 to 40 pounds, and overweight/obese women should limit weight gain to sleep.
• No treatment is necessary, and the patient should be reassured that they are a common and benign complaint in pregnancy.
Hemorrhoids
• Hemorrhoids are varicose veins of the rectum and may become swollen and painful during pregnancy.
• Patients with hemorrhoids should avoid constipation because straining during bowel movements can
aggravate hemorrhoids.
• Good hydration and increased fiber consumption may help soften the stool.
• Hemorrhoids often regress after delivery but usually do not resolve completely.
LAB ASSESSMENT/INFECTION SCREENING
• Table 4-8 lists the routine prenatal testing through a pregnancy.
• Women are screened for various infections during initial prenatal care laboratory assessment or if they have certain environmental exposures.
• Rubella: Screening for antirubella immunoglobulin G (IgG) identifies nonimmune women who should then be offered vaccination preconception or in the postpartum period.
• HBV: Screening of pregnant women for hepatitis B surface antigen is recommended. Women with risks for exposure to HBV (i.e., HIV and certain immunocompromised populations) should be counseled and offered vaccination.
• Tuberculosis (TB): Patients at risk for TB should be tested with subcutaneous purified protein derivative (PPD) challenge; if the patient has a history of bacillus Calmette-Guerin (BCG) vaccination, the PPD screen should still be used unless they have known positive skin testing. Preconception treatment for latent TB infection can be ordered as indicated.
• Cytomegalovirus (CMV): Screening should be offered to women who work in neonatal intensive care units, child care facilities, or dialysis units.
• Parvovirus B19: IgG testing may be offered preconceptually to school teachers and child care workers.
• Toxoplasmosis: Cat owners and women who eat or handle raw meat are at increased risk, but routine testing without risk factors is not recommended. Routine toxoplasmosis screening to determine antibody status before conception mainly provides reassurance to those who are already immune; patients' cats can also be tested.
P.77
TABLE 4-8 Routine Prenatal Testing
Timing Tests
Initial Blood type, Rh type, antibody screen, CBC, rubella, STS/RPR, HBsAg, HIV, Hgb obstetric electrophoresis, urine culture and sensitivity, urine toxicology, Pap smear, gonorrhea,
visit and chlamydia testing. Dating sonogram, if questionable dating criteria for firsttrimester
screening
11-14 First-trimester screening
weeks'
gestation
16-20 MSAFP/quad screen
weeks'
gestation
18-22 Anatomy ultrasound to rule out fetal anomalies
weeks'
gestation
24-28 Blood type, Rh type, antibody screen, CBC, STS/RPR, glucose screen. If high-risk
weeks' patient, repeat HBsAg, HIV, gonorrhea, and chlamydia testing
gestation
36 Group B streptococci culture
weeks'
gestation
CBC, complete blood count; STS, serologic test for syphilis; RPR, rapid plasma reagin; HBsAg, hepatitis B surface antigen; Hgb, hemoglobin; MSAFP, maternal serum alpha-fetoprotein.
• Varicella: Screening for IgG should be performed if a positive history cannot be obtained. The varicella zoster virus vaccine is now recommended for all nonimmune adults. It is a live virus vaccine that should be given prior to conception. Nonimmune individuals can be counseled regarding postexposure prophylaxis during pregnancy.
• HIV: Counseling and testing should be offered routinely to all women. The CDC recommends an “opt-out” strategy to increase screening compliance.
SUGGESTED READINGS
American College of Obstetricians and Gynecologists Committee on Genetics. Committee opinion no. 545: noninvasive prenatal testing for fetal aneuploidy. Obstet Gynecol 2012;120:1532-1534.
American College of Obstetricians and Gynecologists Committee on Practice Bulletins— Obstetrics. ACOG practice bulletin no. 92: clinical management guidelines for obstetriciangynecologists: use of psychiatric medications during pregnancy and lactation. Obstet Gynecol 2008;111(4):1001-1020.
American College of Obstetricians and Gynecologists Committee on Practice Bulletins. ACOG practice bulletin no. 77: screening for fetal chromosomal abnormalities. Obstet Gynecol 2007; 109(1):217-227.
Behnke M, VC Smith. Prenatal substance abuse: short- and long-term effects on the exposed fetus. Pediatrics 2013;131 (3):e1009-e1024.
Bennett RL, Motulsky AG, Bittles A, et al. Genetic counseling and screening of consanguineous couples and their offspring: recommendations of the National Society of Genetic Counselors. J Gen Couns 2002;11(2):97- 119.
Jack B, Atrash HK, eds. Preconception health and health care: the clinical content of preconception care. Am J Obstet Gynecol 2008;199(6)(suppl B):257-395.
Spencer K. Aneuploidy screening in the first trimester. Am J Med Genet C Semin Med Genet 2007;
145C:18-32.