5 Normal Labor and Delivery, Operative Delivery, and Malpresentations
John L. Wu
Betty Chou
Labor is defined as repetitive uterine contractions of sufficient frequency, intensity, and duration to cause progressive cervical effacement and dilation.
STAGES AND PHASES OF LABOR
• The first stage of labor begins with the onset of labor and ends with full cervical dilation. It is divided into latent and active phases (Table 5-1).
• The latent phase begins with regular contractions and ends when there is an increase in the rate of cervical dilation.
• The active phase is characterized by an increased rate of cervical dilation and descent of the presenting fetal part, which may not occur until after 6 cm of dilation. It ends with complete cervical dilation and is further subdivided into:
î Acceleration phase: A gradual increase in the rate of dilation initiates the active phase and marks a change to rapid dilation.
î Phase of maximum slope: the period of active labor with the greatest rate of cervical dilation
î Deceleration phase: the terminal portion of the active phase in which the rate of dilation may slow until full cervical dilation
• The second stage of labor is the interval between full cervical dilation and delivery of the neonate.
• The third stage of labor is the interval between delivery of the neonate and delivery of the placenta.
• The fourth stage of labor, or puerperium, follows delivery and concludes with resolution of the physiologic changes of pregnancy, usually by 6 weeks postpartum.
P.79
TABLE 5-1 Stages and Phases of Labor
| Parameter | Nulliparous | Multiparous |
| Latent phase of first-stage labor | ||
| Mean | 6 hr | 5 hr |
| Fifth percentile | 21 hr | 14 hr |
First stage of labor (total)
| Mean | 10 hr | 8 hr |
| Fifth percentile | 25 hr | 19 hr |
| Second stage of labor | ||
| Mean | ||
| Fifth percentile | 33 min | 9 min |
| Prolonged (without epidural) | 118 min | 47 min |
| Prolonged (with epidural) | 2 hr | 1 hr |
| Prolonged (with epidural) | 3 hr | 2 hr |
| Third stage of labor | ||
| 5 min | 5 min | |
| Prolonged | 30 min | 30 min |
| Rate of maximal dilation | ||
| Mean | 3.0 cm/hr | 5.7 cm/hr |
| Fifth percentile | 1.2 cm/hr | 1.5 cm/hr |
| Rate of descent | ||
| Mean | 3.3 cm/hr | 6.6 cm/hr |
| Fifth percentile | 1.0 cm/hr | 2.0 cm/hr |
Adapted from Liao JB, Buhimschi CS, Norwitz ER.
Normal labor: mechanism and duration. Obstet Gynecol Clin North Am 2005;32(2):145-164; American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Obstetrics. Practice bulletin no. 49: dystocia and augmentation of labor. Obstet Gynecol 2003; 102:1445-1454.During this time, the reproductive tract returns to its nonpregnant state, and ovulation may resume.
MECHANISM OF LABOR
The cardinal movements of labor refer to the changes in position of the fetal head during its descent through the birth canal in vertex presentation:
• Descent (lightening): movement of the fetal head through the pelvis toward the pelvic floor. The highest rate of descent occurs during the deceleration phase of the first stage and during the second stage of labor.
• Engagement: the descent of the widest diameter of the presenting fetal part below the plane of the pelvic inlet. The widest diameter in cephalic presentation is the biparietal diameter. In breech presentation, the bitrochanteric diameter determines the station.
• Flexion: a passive movement that permits the smallest diameter of the fetal head (suboccipitobregmatic diameter) to pass through the maternal pelvis
• Internal rotation: The fetal occiput rotates from its original position (usually transverse) toward the symphysis pubis (occiput anterior) or, less commonly, toward the hollow of the sacrum (occiput posterior).
P.80
• Extension: The fetal head is delivered by extension from the flexed position as it travels beneath the symphysis pubis.
• External rotation: The fetal head turns to realign with the long axis of the spine, allowing the shoulders to align in the anterior—posterior axis.
• Expulsion: The anterior shoulder descends to the level of the symphysis pubis. After the shoulder is delivered under the symphysis pubis, the remainder of the fetus is delivered.
MANAGEMENT OF NORMAL LABOR AND DELIVERY
Initial Assessment
History
• Age, parity (full-term deliveries [≥37 weeks], preterm deliveries [≥20 to is contraindicated (Table 5-2).
Consideration of fetal lung maturity is necessary before elective induction of labor prior to 39 weeks of gestation. Amniocentesis is not necessary if the induction is medically indicated and the risk of continuing the pregnancy is greater than the risk of delivering before lung maturity. The favorability of the cervix at the time of induction is related to the success of labor induction. When the Bishop score (Table 5-3) exceeds 8, theP.82 likelihood of vaginal delivery after induction is similar to that with spontaneous labor. Induction with a lower Bishop score has been associated with a higher rate of failure, prolonged labor, and cesarean delivery.
TABLE 5-2 Induction of Labor: Indications and Contraindications
| Indications | Contraindications |
| î Abruptio placentae, chorioamnionitis, gestational hypertension î Premature rupture of membranes, postterm pregnancy, preeclampsia, eclampsia î Maternal medical conditions (e.g., diabetes mellitus, renal disease, chronic pulmonary disease, chronic hypertension) î Fetal compromise (e.g., severe fetal growth restriction, isoimmunization) î Fetal demise î Elective inductions for gestational age >39 wk for logistical issues such as remote access to care, psychosocial reasons, and history of rapid deliveries. Typically only considered if cervix is favorable. | î Vasa previa or complete placenta previa î Transverse fetal lie î Infection—active HSV, high viral load HIV î Pelvic structural deformities î Umbilical cord prolapse î Advanced cervical cancer |
HSV, herpes simplex virus.
Adapted from American College of Obstetricians and Gynecologists—Obstetrics. ACOG practice bulletin no. 107: induction of labor. Obstet Gynecol 2009;114:386-397.
• Cervical ripening may be used to soften the cervix before induction if the Bishop score is low. Cervical ripening can be achieved using pharmacologic and mechanical methods.
TABLE 5-3 Components of the Bishop Score
Rating
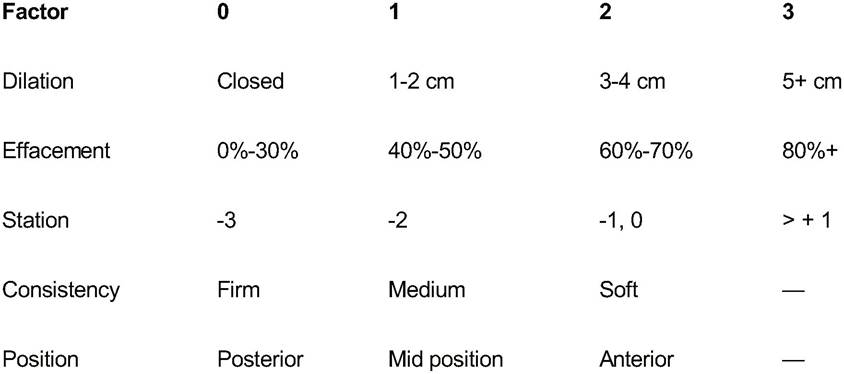
Adapted from Bishop EH. Pelvic scoring for elective induction. Obstet Gynecol 1964;24:267.
P.83 • Pharmacologic methods of induction of labor and cervical ripening
• Low-dose oxytocin may be used with or without mechanical dilators.
• Prostaglandin E2 is superior to placebo in promoting cervical effacement and dilation and may enhance sensitivity to oxytocin.
î Prepidil gel contains 0.5 mg of dinoprostone in a 2.5-mL syringe; the gel is injected into the cervical canal every 6 hours for up to 3 doses in a 24-hour period.
î Cervidil is a vaginal insert containing 10 mg of dinoprostone. It provides a lower rate of release (0.3 mg/hr) than the gel but has the advantage that it can be removed if uterine tachysystole occurs (>5 contractions in 10 minutes).
• Prostaglandin E1 is also effective in stimulating cervical ripening.
î Cytotec (misoprostol) is administered as 25 to 50 mg every 3 to 6 hours intravaginally. The use of misoprostol for cervical ripening is off-label.
• Side effects: Any pharmacologic induction method includes a risk of uterine tachysystole. If oxytocin is being used, it can be titrated down or turned off with quick effect due to its short half-life. If Cervidil is being used, the insert can be removed. If indicated, a beta-adrenergic agonist (e.g., terbutaline sulfate) can be administered. Maternal systemic effects of prostaglandins may include fever, vomiting, and diarrhea.
• Contraindications: A history of uterine scar or prior cesarean delivery, allergy to the medication, or active vaginal bleeding. Caution should be exercised when using prostaglandin E2 in patients with glaucoma or severe hepatic or renal impairment.
• Mechanical methods of labor induction and cervical ripening
• Membrane stripping
• Amniotomy (artificial rupture of membranes): The risk of umbilical cord prolapse can be reduced by performing the amniotomy while the fetal presenting part is well applied to the cervix.
• Balloon catheters placed transcervically: A single-balloon device such as a 24-French Foley catheter with 30-mL bulb inserted into the extra-amniotic space. Other options are to use larger volume bulb catheters or a double-balloon device.
• Hygroscopic dilators (laminaria)
OXYTOCIN ADMINISTRATION
• Indications: Oxytocin is used for both induction and augmentation of labor. Augmentation should be considered for protracted or arrest disorders of labor or the presence of a hypotonic uterine contraction pattern. A range of opinions regarding the dosage of oxytocin exist. A reasonable starting dosage is 0.5 to 4 mIU/min, with incremental increases of 1 to 2 mIU/min every 20 to 30 minutes. Cervical dilation of at least 1 cm/hr in the active phase indicates that oxytocin dosing is adequate. If an intrauterine pressure catheter is in place, 180 Montevideo units (MVU) per 10-minute period is considered adequate. However, some practitioners use a threshold of 250 to 275 MVU with increased success of induction and minimal adverse consequences.
• Complications: Adverse effects of oxytocin are primarily dose-related. The most common complication is uterine tachysystole, which may result in uteroplacental hypoperfusion and nonreassuring fetal heart tracing. Uterine tachysystole is usually reversible when oxytocin infusion is decreased or discontinued. If necessary, a beta-adrenergic agent may be administered. Rapid infusion of oxytocin can result in hypotension. Prolonged infusion can result in water intoxication and hyponatremia
P.84 because oxytocin structurally resembles antidiuretic hormone; it also increases the risk of postpartum uterine atony and hemorrhage.
Labor Progress Assessment
• Dr. Emanuel Friedman’s studies on normal labor resulted in widely used guidelines for normal labor progress (see Table 5-1, p. 79).
• Abnormal labor progression is identified when the patient falls below the fifth percentile of expected cervical change and fetal descent.
• Latent phase prolongation is somewhat controversial, as measurement of this phase is difficult and inexact. Generally speaking, without induction, this phase is considered prolonged if it exceeds 20 hours in a nulliparous patient and 14 hours in a multiparous patient.
• The active phase is considered protracted if the rate of cervical change is g or ≥4,500 g), epidural anesthesia, chorioamnionitis, a history of previous complications like perinatal death, and amniotic fluid abnormalities
• Risks for an abnormal second stage of labor: a prolonged first stage, occiput posterior position, epidural anesthesia, nulliparity, short maternal stature, increased birth weight, and high station at complete cervical dilation
Interventions for Abnormal Labor
• Amniotomy: Artificial rupture of membranes may enhance progress for a patient who is in active labor, although it may increase the risk of chorioamnionitis.
• Augmentation of labor via oxytocin: Oxytocin has been shown to decrease the time of active labor in nulliparous women. In addition, some studies have shown that it decreases the rate of cesarean section for failure to progress.
• Uterine contraction monitoring: Placement of an intrauterine pressure catheter provides information about the frequency and strength of contractions and may be useful for titrating oxytocin to maximize the chance for successful vaginal delivery.
P.85
FETAL HEART RATE EVALUATION
Guidelines for fetal heart rate (FHR) or fetal heart tracing (FHT) interpretation are given in Table 5-4.
• Baseline rate: lasts for at least 2 minutes during a 10-minute section rounded to the nearest 5 beats per minute (bpm)
• Normal rate: 110 to 160 bpm
• Bradycardia: A baseline FHR 160 bpm. The most common cause is maternal fever or infection. Other less common causes of fetal tachycardia include fetal arrhythmias or maternal administration of parasympatholytic or sympathomimetic drugs.
• Variability: Beat-to-beat fluctuations in the FHR. It is most reliable when measured with a fetal scalp electrode.
• Absent: absent variability
• Minimal: detectable variability of 25 bpm
• Accelerations: For gestational age (GA) >32 weeks, an acceleration is an increase in FHR of at least 15 bpm that lasts for at least 15 seconds. For GA 10 bpm for 10 seconds.
• FHT is reactive if it shows two accelerations within 10 minutes.
• A sinusoidal FHT is a persistent smooth undulating pattern with a frequency of 3 to 5 cycles/min. It is concerning and requires immediate evaluation. Fetal anemia; analgesic drugs such as morphine, meperidine, alphaprodine, and butorphanol; and chronic fetal distress should be considered.
• Decelerations: a decrease in FHR below the baseline. In some instances, the pattern of deceleration of the FHR can be used to identify the cause.
• Variable decelerations may start before, during, or after the uterine contraction starts (hence the designation “variable”). They usually show an abrupt onset to nadir in 15 bpm lasting >15 seconds but 30 seconds and gradual return, reach their nadir after the peak of the contraction, and do not return to the baseline until after the contraction is over. They may result from uteroplacental insufficiency and relative fetal hypoxia. Recurrent late decelerations can be an ominous sign.
• Prolonged deceleration: a deceleration that lasts longer than 2 minutes but 50% of uterine contractions in any 20-minute span
• Intermittent decelerations: occur with be performed to place internal monitors, unless these are contraindicated by the clinical situation.
• Fetal scalp electrode (FSE): Direct application of an FSE records the fetal electrocardiogram (fECG) waveform and may allow closer evaluation of the FHR. An FSE may be contraindicated in cases of fetal coagulopathy or maternal infections such as HIV, active herpes simplex virus, and hepatitis B or C.
• Intrauterine pressure catheter and amnioinfusion: A catheter is inserted into the chorioamnionic sac and attached to a pressure gauge. Pressure readings provide quantitative data on the strength and duration of contractions. Amnioinfusion of room temperature normal saline can be used to replace amniotic fluid volume to relieve recurrent variable decelerations in patients with oligohydramnios. Care should be used to avoid overdistention of the uterus.
• Tocolytic agents: Beta-adrenergic agonists (e.g., terbutaline, 0.25 mg subcutaneously or 0.125 to 0.25 mg IV) can be administered to decrease uterine activity in the presence of uterine tachysystole. Potential side effects of beta-adrenergic agonists include elevated serum glucose levels and increased maternal and fetal heart rates.
• Management of maternal hypotension: Maternal hypotension, as a complication of the sympathetic blockade associated with epidural anesthesia or from
P.88 compression of the vena cava, can lead to decreased placental perfusion and FHR decelerations. IV fluid bolus, left uterine displacement, and ephedrine or phenylephrine administration may be appropriate.
• Fetal scalp blood pH: Determination of fetal scalp blood pH can clarify the acid-base state of the fetus. A pH value of 7.25 or higher is normal. A pH range of 7.20 to 7.24 is a preacidotic. A pH of A pediatrician should be notified. If available, an anesthesiologist should also be informed.
• The time should be marked when the dystocia is called and the total time until delivery recorded in the notes. Once the shoulder dystocia is identified, no significant pressure should be applied to the head until the shoulders are delivered. Fundal pressure should never be applied as it only exacerbates the shoulder impaction.
• McRoberts maneuver is performed by hyperflexion and abduction of the maternal hips, flattening the lumbar spine, and rotating the pelvis to increase the anterior-posterior outlet diameter.
• Suprapubic pressure is applied in a vector chosen to anteriorly rotate the anterior fetal shoulder and dislodge the shoulder from the symphysis.
• Other measures in combination are chosen for the specific clinical situation based on clinician experience. There is no “right order” in which the maneuvers described in the following text should be performed, and maneuvers can and should be used more than once, as needed.
• Delivery of the posterior arm: By grabbing the posterior hand, the posterior arm can be flexed and swept across the fetal chest, delivered first, thereby creating more room for the anterior shoulder.
• Episiotomy: Incision of the perineum provides additional room and should be considered if it might facilitate delivery or additional maneuvering.
• Rubin maneuver: The anterior fetal shoulder is rotated obliquely with a vaginal hand. This maneuver may
also be performed in a posterior manner.
• Wood corkscrew: The posterior shoulder is rotated over 180 degrees with a vaginal hand to assist delivery of the shoulders.
• Gaskin maneuver: Facilitated in the unanesthetized patient, she is turned over on “all fours,” inverting the anterior and posterior shoulders.
• Delivery that does not occur following the aforementioned maneuvers may require some of the more invasive and traumatic procedures noted in the following text for the sake of fetal viability.
• Neonatal clavicular fracture: Palpate the clavicles and apply outward pressure with the thumb to avoid lung or subclavian artery injury.
• In extreme cases, the Zavanelli maneuver (in which the fetal head is flexed and pushed back up into the uterus as preparations for emergent cesarean section are made) or symphysiotomy (performed by laterally displacing the urethra using the index and middle fingers placed against the posterior aspect of the symphysis and incising the cartilaginous portion of the symphysis) could be performed.
CESAREAN SECTION
• Fetal indications for cesarean delivery include:
• Nonreassuring FHT
• Nonvertex presentation (malpresentation)
• Fetal anomalies, such as hydrocephalus, that would make successful vaginal delivery unlikely
P.91
• Umbilical cord prolapse
• Conjoined twins
• Maternal indications for cesarean delivery include:
• Obstruction of the lower genital tract (e.g., large condyloma)
• Previous cesarean section (if vaginal birth after cesarean [VBAC] is declined or not appropriate)
• Previous uterine surgery involving the contractile portion of the uterus (i.e., classical cesarean, transmural myomectomy)
• History of severe pelvic floor injury from a prior vaginal delivery
• Abdominal cerclage
• Maternal and fetal indications include:
• Abruptio placentae
• Active maternal herpes simplex virus infection
• Labor dystocia or cephalopelvic disproportion
• Placenta previa or known vasa previa (absolute indication)
• The patient should be counseled regarding standard risks of surgery, such as pain, bleeding that may require transfusion, infection, damage to nearby organs, and a small but increased risk of death when compared to vaginal delivery.
VAGINAL BIRTH AFTER CESAREAN SECTION
• Provided there are no contraindications to vaginal delivery, a patient may be counseled and offered a trial of labor after previous cesarean delivery (TOLAC). Success rates of VBAC are higher for patients with nonrecurring conditions, such as malpresentation or fetal intolerance of labor (60% to 85%), than for those with a prior diagnosis of dystocia (15% to 30%). Patients should be counseled regarding the risk of uterine rupture (0.9% to 3.7%), failed trial of labor, and need for cesarean delivery. Someone with a history of two prior C-sections may consider a TOLAC, depending on prior indications, although some providers may choose not to offer it.
• Contraindications include previous classical or inverted T-shaped uterine incision, transfundal uterine surgery, history of uterine rupture, contracted pelvis, and medical or obstetric contraindications to vaginal delivery.
• Epidural anesthesia and oxytocin may be used with VBAC. The delivery hospital must have facilities and staffing for emergency cesarean delivery. Blood products should be readily available. The most common sign of uterine rupture is a nonreassuring FHR pattern with variable decelerations evolving into late decelerations, bradycardia, and undetectable FHR. Other findings include uterine or abdominal pain, loss of station of the presenting part, vaginal bleeding, and hypovolemia.
Malpresentations
Normal presentation is defined by longitudinal lie, cephalic presentation, and flexion of the fetal neck. All other presentations are malpresentations. Occurring in approximately 5% of all deliveries, malpresentations may lead to abnormalities of labor and increased risk for mother or fetus.
• Risk factors for malpresentation are conditions that decrease the polarity of the uterus, increase or decrease fetal mobility, or block the presenting part from the pelvis.
• Maternal factors include grand multiparity, pelvic tumors, uterine fibroids, pelvic contracture, and uterine malformations.
P.92
• Fetal factors include prematurity, multiple gestation, polyhydramnios or oligohydramnios, macrosomia, placenta previa, hydrocephaly, trisomy, anencephaly, and myotonic dystrophy.
• Breech presentation occurs when the cephalic pole is in the uterine fundus. Major congenital anomalies occur in 6.3% of term breech presentation infants compared to 2.4% of vertex presentation infants.
• The incidence of breech presentation is 25% of pregnancies at Beckmann CR, Ling FW, Herbert WN, et al. Obstetrics and Gynecology, 2nd ed. Baltimore, MD: Lippincott Williams & Wilkins, 1995:194, with permission.)
P.93
• A pediatrician is available.
• An obstetrician is available who is experienced with vaginal breech delivery.
• In breech presentation, the fetus usually emerges in the sacrum transverse or oblique position. As crowning occurs (the bitrochanteric diameter passes under the symphysis), an episiotomy can be considered.
• When the umbilicus appears, place fingers medial to each thigh and press out laterally to deliver the legs (Pinard maneuver). The fetus should then be rotated to the anterior sacrum position, and the trunk can be wrapped in a towel for traction.
• When the infant's scapulas appear, the arms can be delivered. The shoulders can be grasped posteriorly, the humerus followed down, and each arm rotated across the chest and out (Lovsett maneuver). To deliver the right arm, the fetus is turned in a counterclockwise direction; to deliver the left arm, the fetus is turned in a clockwise direction.
If the head does not deliver spontaneously, the head may be flexed by placing downward traction and pressure on the maxillary ridge (Mauriceau-Smellie-Veit maneuver). Direct vertical suprapubic pressure may
also be applied. Piper forceps may be used to assist in delivery of the head.
• For delivery of a breech second twin, ultrasonography should be available in the delivery room. The operator reaches into the uterus and grasps both feet, trying to keep the membranes intact. The feet are brought down to the introitus, then amniotomy is performed. The body is delivered to the scapula by applying gentle traction on the feet. The remainder of the delivery is the same as that described earlier for a singleton breech.
• Head entrapment during breech vaginal delivery may be managed by one or more of the following procedures:
• Duhrssen incisions are made in the cervix at the 2, 6, and 10 o'clock positions. Up to three incisions may be needed to facilitate delivery of the fetal head through the cervix. The 3 and 9 o'clock positions should be avoided due to the risk of dividing the cervical vessels with resultant hemorrhage.
• Relaxation agents (nitric oxide or nitroglycerine) may release the entrapped head, enabling proper head flexion and vaginal delivery.
• Cephalocentesis can be performed if the fetus is not viable. The procedure is performed by perforating the base of the skull and suctioning the cranial contents.
• External cephalic version
• Indication is persistent breech presentation at term. The version is performed to avoid breech presentation in labor.
• Risks include compromised umbilical blood flow, placental separation, fetal distress, fetal injury, premature rupture of membranes, and fetomaternal bleeding (overall incidence is 0% to 1.4%). The most common “risk” is failed version.
• Success rate for external cephalic version ranges from 35% to 86%, but in 2% of cases, the fetus reverts back to breech presentation.
• Technique: A GA of at least 36 weeks, reactive nonstress test, and informed consent must be obtained. Version is generally accomplished by applying a liberal amount of lubrication then transabdominally grasping the fetal head and fetal breech and manipulating the fetus through a forward or backward roll. Ultrasonographic guidance is an important adjunct to confirm position and monitor FHR. Tocolysis and spinal or epidural anesthesia may improve success rates. After the procedure, the patient should be monitored continuously until the FHR is reactive, no decelerations are present, and no evidence of regular contractions exists. Rh-negative patients should receive Rho (D) immunoglobulin (RhoGAM) after the procedure because of the potential for fetomaternal bleeding.
P.94
• Factors associated with failure include obesity, oligohydramnios, deep engagement of the presenting part, a partial uterine septum, and fetal back posterior. Nulliparity and an anterior placenta may also reduce the likelihood of success.
• Contraindications to external cephalic version include conditions in which labor or vaginal delivery would be contraindicated. Version is not generally recommended in cases of ruptured membranes, third-trimester bleeding, oligohydramnios, multiple gestations, or after labor has begun.
• Abnormal lie
• Lie refers to the alignment of the fetal spine in relation to the maternal spine. Longitudinal lie is normal, whereas oblique and transverse lies are abnormal. Abnormal lie is associated with multiparity, prematurity, pelvic contraction, and disorders of the placenta.
• Incidence of abnormal lie is 1 in 300 term pregnancies. At 32 weeks' gestation, the incidence is J, Landy HJ, Branch DW, et al; Consortium on Safe Labor. Contemporary patterns of spontaneous labor with normal neonatal outcomes. Obstet Gynecol 2010;116(6):1281-1287.