6 Fetal Assessment
Sarahn M. Wheeler
Edith Gurewitsch Allen
Antenatal fetal surveillance is performed using various modalities that allow care providers to closely monitor fetuses at risk for uteroplacental insufficiency.
Its purpose is to detect signs of fetal compromise related to poor uteroplacental perfusion in order to circumvent fetal hypoxemia, acidemia, and death. Performed serially at regular intervals, antenatal fetal testing is used to assess ongoing fetal well-being, guide antenatal management, and determine possible need for imminent delivery or other acute obstetric management. It is therefore important that providers of obstetric care be well versed in the different modalities of fetal testing, including their limitations and implications.METHODS OF FETAL ASSESSMENT
There are numerous methods to assess fetal well-being, and no single test is superior to another method. Each test has its own individual merits (as well as limitations) and often are used in combination to create an overall picture of the fetal state and help identify fetal compromise (Table 6-1).
Fetal Movement
• Maternal assessment of fetal movement (kick counts)
• Least expensive and least invasive fetal assessment test
• Requires neither equipment nor hospital setting
P.96
TABLE 6-1 Comparison of Antenatal Fetal Tests
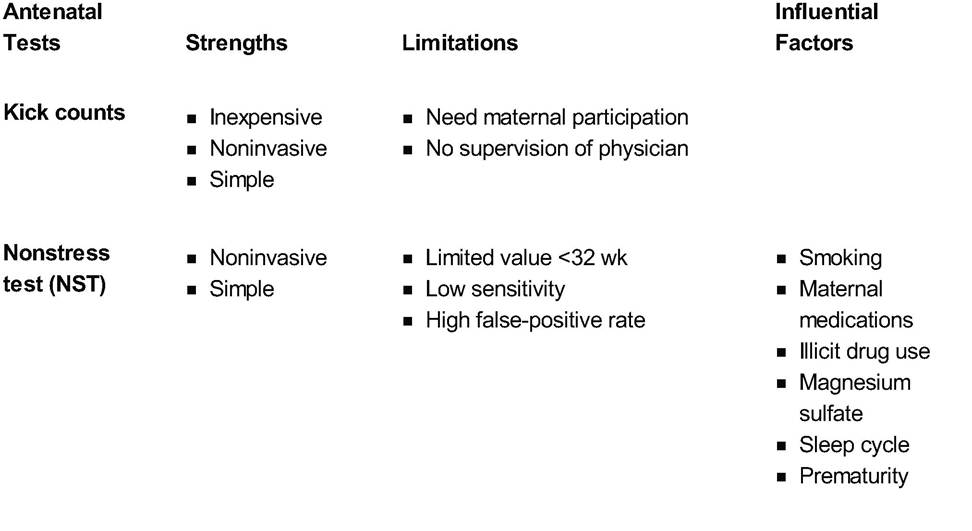
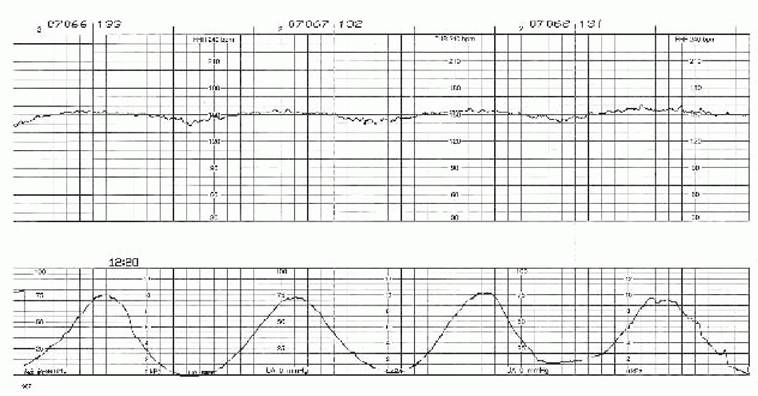
| Vibroacoustic stimulation (VAS) | ■ Noninvasive ■ Prevents some false-positive results from NST | ■ Limited value 90%. The positive predictive value is only 50% to 70%. Therefore, the NST is better suited to rule out rather than predict fetal compromise. Given the high false-positive rate, a nonreactive NST should be followed by more extensive testing such as biophysical profile, vibroacoustic stimulation, or contraction stress test. • Contraction stress test (CST) or oxytocin challenge test (OCT) • Purpose: The CST is designed to assess fetal response to the stress of induced uterine contractions causing transient uteroplacental insufficiency. • Method of testing: The mother is placed in the left lateral tilt position, and external monitors are applied. If three contractions of 40 seconds duration or greater are noted, a “spontaneous” CST can be performed without stimulation. In the absence of spontaneous contractions, uterine activity can be induced either by nipple stimulation or with a dilute solution of oxytocin until three contractions occur in a 10-minute time period. • Criteria for test results: A “positive” CST demonstrates late decelerations with more than 50% of contractions (Fig. 6-2). Late decelerations reach their nadir after the peak of the contraction. A “negative” CST demonstrates no late decelerations. A CST with intermittent late decelerations is considered equivocal, and further evaluation of the pregnancy is warranted. An “inadequate” or “unsatisfactory” CST is one in which adequate contractions are not achieved. P.99 If hyperstimulation occurs, an abnormal fetal response may be the result of the testing technique alone and should be repeated or another form of testing should be done.
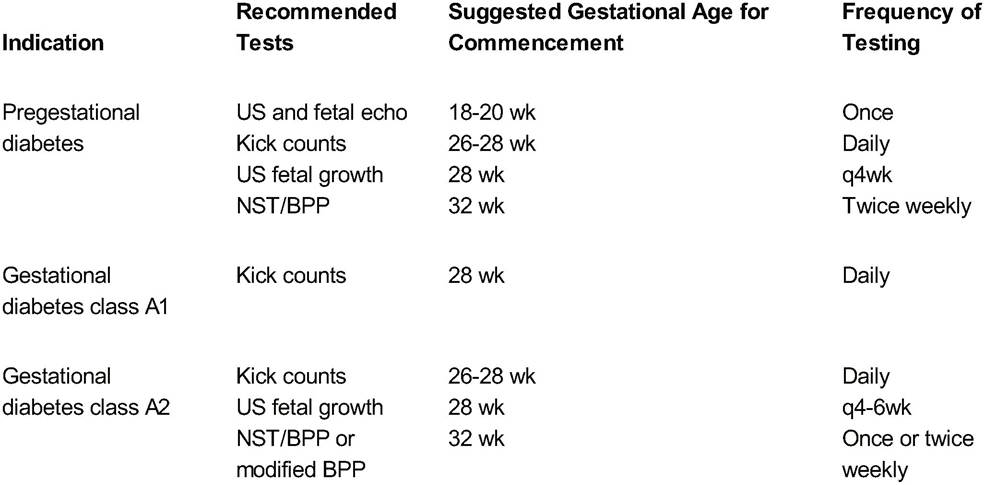
Figure 6-2. Fetal heart tracing with late decelerations. Following each contraction (bottom tracing) is a slight depression of the fetal heart rate (top tracing), suggesting uteroplacental insufficiency. (Original fetal monitor strip from Dr. Janice Henderson, Johns Hopkins Hospital, Department of Gynecology and Obstetrics, Division of Maternal Fetal Medicine.) • Strengths and limitations: CST is one of the most labor-intensive methods of fetal surveillance but has the highest specificity for detecting the compromised fetus. It has a negative predictive value of >99%. Relative contraindications to CST include preterm labor, preterm premature rupture of membranes (PPROM), placenta previa, and high risk for uterine rupture. Previous low transverse cesarean section is not a contraindication.• Vibroacoustic stimulation test (VAS) • Purpose: VAS is a useful adjunct to a nonreactive NST. This test will decrease false-positive results of nonreactive NST if the cause of the abnormal test is fetal sleep and potentially decrease testing. • Method of testing: VAS is performed by placing a vibrating auditory source, such as an artificial larynx, on the maternal abdomen. The sound device is placed halfway between the pubic symphysis and umbilicus, and it delivers a short burst of sound to the fetus for 5 seconds. The procedure stimulates the fetus to move and shortens the time necessary to produce fetal heart rate accelerations. It is important to avoid stimulating the fetus when it is experiencing stress from a contraction because this may cause the fetus to have a drop in heart rate. • Criteria for test results: The VAS is used in conjunction with the NST and is interpreted similarly to the NST as discussed earlier. Fetal Heart Monitoring with Ultrasonography • Biophysical profile (BPP) • Purpose: The BPP uses ultrasound observations in conjunction with the NST to help predict acute and chronic tissue hypoxia. It has excellent negative predictive value for fetal mortality in the 72 to 96 hours after the test. It has been shown to reduce perinatal morbidity and mortality. • Method of testing: The BPP has five components: fetal breathing, fetal movement, fetal tone, and amniotic fluid assessment determined by ultrasound along with the NST. Two points are awarded for each observed parameter. No points are awarded for a nonreactive NST or the absence of any parameter. Therefore, only even number scores are possible, with a maximum score of 10. The specific criteria of these components are listed in Table 6-2. All of the sonographic criteria must be observed within a 30-minute period. • Criteria for test results: A score of 8 or 10 is reassuring, and routine surveillance and expectant obstetric management may continue. A score of 6 raises concern, and the BPP should be repeated in 6 to 24 hours, especially in fetuses over 32 weeks' gestation. If the score does not improve, delivery should be considered, depending on gestational age and individual circumstances. Scores of 4 or below are worrisome, and delivery should be considered, again depending on gestational age and clinical context. It is important to consider that fetal breathing can be reduced in preterm fetuses well-being.P.102 Glucocorticosteroids given for the purpose of maturing premature fetal lungs have been shown to influence BPP scores by decreasing the AFI, decreasing fetal movement, and decreasing breathing motion. Magnesium sulfate can decrease the fetal heart rate variability. Other medications such as narcotics, sedatives, and betablockers have been shown to decrease fetal heart rate variability and reactivity. • Maternal smoking and illicit drugs: The maternal use of illicit drugs and smoking results in a transient decrease in fetal heart rate variability. • Maternal hypoglycemia: Maternal hypoglycemia may reduce fetal heart rate variability as well as fetal movement and breathing. INDICATIONS FOR FETAL TESTING • Maternal conditions and complications of pregnancy: There are numerous maternal medical conditions, complications of pregnancy, and fetal conditions that confer increased risk of adverse fetal outcomes. Therefore, antenatal fetal surveillance is recommended in these high-risk pregnancies in an attempt to decrease fetal morbidity and mortality. Tables 6-3 and 6-4 outline some of the maternal and fetal indications for antenatal fetal surveillance, the methods of testing to be employed for fetal assessment, the gestational age to begin testing, and the frequency of monitoring. Other indications for fetal testing are chronic hypertension, preeclampsia, maternal renal disease, lupus, maternal hemoglobinopathies, antiphospholipid syndrome, chronic abruption, and monoamnionic monochorionic twins. • Commencement and frequency of testing: Each maternal and fetal indication for fetal surveillance has its own recommendations for the commencement and frequency of testing based on the underlying etiology of disease and the perceived risk to the fetus. TABLE 6-3 Recommendations for Antenatal Fetal Assessment: Diabetes
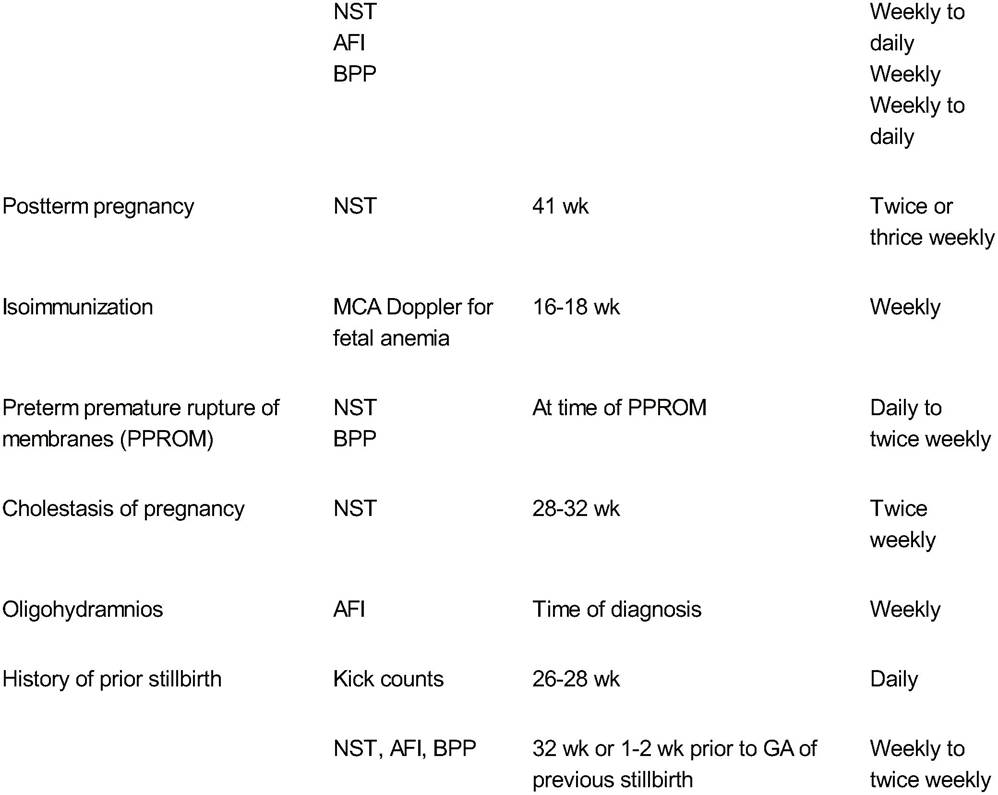
US, ultrasound; NST, nonstress test; BPP, biophysical profile. P.103 TABLE 6-4 Recommendations for Antenatal Fetal Testing: Fetal Conditions
NST, nonstress test; AFI, amniotic fluid index; BPP, biophysical profile; MCA, middle cerebral artery; GA, gestational age. P.104 SUGGESTED READINGS American College of Obstetricians and Gynecologists. Practice bulletin no. 9: antepartum fetal surveillance. Int J Gynaecol Obstet 2000;68(2):175-185. Devoe LD. Antenatal fetal assessment: contraction stress test, nonstress test, vibroacoustic stimulation, amniotic fluid volume, biophysical profile, and modified biophysical profile—an overview. Semin Perinatol 2008;32:247-252. Nageotte M. Antenatal testing: diabetes mellitus. Semin Perinatol 2008;32:269-270. Turan S, Miller J, Baschat A. Integrated testing and management in fetal growth restriction. Semin Perinatol 2008;32:194-200.
More medical literature on Medic.Studio
More on the topic 6 Fetal Assessment:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|