7 Complications of Labor and Delivery
Veena Choubey
Erika F. Werner
UTERINE DEHISCENCE OR RUPTURE
Dehiscence is defined as lower uterine scar separation that does not breach the serosa; it rarely causes significant bleeding.
Rupture is defined as complete separation of the uterine wall and may lead to fetal distress and significant maternal hemorrhage.Incidence
• Uterine rupture occurs in 0.2% to 1.8% of patients with one or more previous low-segment transverse cesarean sections and in 4% to 9% of patients with a prior uterine active segment incision (classical cesarean or T-incision). One third of prior classical cesarean scar rupture occurs before the onset of labor.
Etiology
• Significant risk factors include:
• Cesarean section
• Prior uterine perforation
• Previous resection of cornual ectopic pregnancy
• Prostaglandin induction of labor with history of prior cesarean
• Other situations that may increase the risk of uterine rupture but not as significantly include:
• Collagen disorders
• Abdominal myomectomies in which the endometrial cavity was invaded
Diagnosis and Management
• Fetal bradycardia is clinically manifested in 33% to 70% of cases. Fetal distress may be the initial presentation in catastrophic uterine rupture. In more subtle cases, the
P.105 initial presentation may be a simple rise in fetal station or change in the position for fetal heart monitor placement. Maternal signs and symptoms include hypotension, uterine tenderness, a change in uterine shape, or constant abdominal pain.
• When uterine rupture is suspected, it is important to proceed emergently to laparotomy with delivery of the infant and repair of the uterine rupture. Rates of recurrent rupture in subsequent pregnancies carried to term approach 22%. Recommendations are for early delivery via cesarean section by 36 weeks.
UMBILICAL CORD PROLAPSE
• Umbilical cord prolapse occurs when the umbilical cord slips beyond the presenting fetal part and passes through the open cervical os (overt) or descends alongside the presenting part (occult).
The fetal blood supply is effectively compromised when the cord is compressed. The overall incidence is 1 to 6 per 1,000 births. The incidence in breech deliveries is slightly higher than 1 %, and in footling breech or rupture of membranes with transverse lie may be as high as 10% to 15%.Etiology
• Risk factors include ruptured membranes, unengaged fetal presenting part (including disengagement), malpresentation (breech, transverse, oblique), prematurity, multiple gestation (second twin), multiparity, and polyhydramnios.
Diagnosis
• Cord prolapse usually causes severe prolonged fetal bradycardia or persistent moderate to severe variable decelerations. Vaginal exam may confirm overt prolapse; the cord will be palpable.
Management
• If the cord is felt on vaginal examination, elevate the presenting part to relieve pressure on the cord, call for help, and move to the operating room for emergent cesarean section.
• Appropriate anesthesia should be administered in the operating room and the viability of the fetus confirmed before proceeding with cesarean section.
• Placing the patient in Trendelenburg or knee-chest position may relieve cord compression with prolapse, but the vaginal hand should continue to elevate the presenting part. This should not delay transportation to the operating room.
• The interval between cord prolapse and delivery is the major predictor of newborn status. If delivered expeditiously, the neonatal outcomes are generally favorable. A cord gas should be obtained at the delivery to assess the degree of hypoxia.
AMNIOTIC FLUID EMBOLISM
Amniotic fluid embolism (AFE) is a rare complication. Fetal fluid, tissue, or debris enters the maternal circulation via the placental bed and triggers acute anaphylaxis.
Incidence
• Approximately 1 in 20,000 singleton pregnancies is complicated by AFE.
• Mortality is around 25% in the United States, much lower than the typically reported 60% to 80%. AFE accounts for 10% of maternal deaths in the United
P.106 States.
Severe neurologic deficits occur in a high percentage of survivors. Neonatal survival is reported at 70%.Etiology and Diagnosis
• The term embolism is a misnomer because the clinical findings are probably a result of anaphylactic shock rather than pulmonary embolism. Amniotic fluid has been shown to cause vasospasm of the pulmonary vasculature in animal models.
• Risk factors include induced labor, advanced maternal age, multiparity, uterine rupture, abdominal trauma, placental abruption, diabetes, cervical lacerations, and operative delivery.
• AFE is primarily a clinical diagnosis of exclusion, made when a woman acutely presents with profound hypoxia, shock, and cardiovascular collapse during or immediately after labor. Cyanosis, hemorrhage, coma, and disseminated intravascular coagulation rapidly ensue.
• The differential diagnosis includes other acute events such as pulmonary embolism, hemorrhage, drug reaction, anaphylaxis, sepsis, and myocardial infarction.
• Useful laboratory data include arterial blood gas, serum electrolytes, calcium and magnesium levels, coagulation profile, and complete blood count.
• Definitive diagnosis is made only at autopsy, when amniotic fluid debris (e.g., fetal squamous cells or hair) are found in the maternal pulmonary vasculature. This debris may be present in the maternal circulation of women without AFE, however, so this finding is not pathognomonic.
Management
• Approximately 65% of AFE occurs before delivery. Emergent delivery is required for both fetal and maternal benefits.
• The patient should be intubated and aggressively resuscitated.
• Administer intravenous (IV) fluids, inotropic agents, and pressors to maintain adequate blood pressure. Packed red blood cells (PRBC) and fresh frozen plasma (FFP) should be available, as there is a high risk for disseminated intravascular coagulation (DIC). Factor VII has been used in cases of severe DIC. Despite all efforts, significant maternal morbidity and mortality remain high.
POSTPARTUM HEMORRHAGE
Postpartum hemorrhage (PPH) is defined as:
• Estimated blood loss (EBL) >500 mL for a vaginal delivery or >1,000 mL for a cesarean delivery; or
• Ten percent drop in hematocrit between admission and the postpartum period; or
• Any bleeding sufficient to cause symptoms or require erythrocyte transfusion (Table 7-1).
Incidence
• PPH is the leading cause of maternal death, accounting for at least 25% of maternal deaths worldwide. It is the second leading cause of pregnancy-related death in the United States, accounting for 17% of maternal mortality.
Etiology and Management
• Patients often tolerate loss of up to 20% of blood volume before symptoms of hypovolemia develop (see Chapter 3). Prompt, even anticipatory, action is crucial.
P.107 Blood flow to the gravid uterus is 600 to 900 mL/min; patients can become unstable rapidly.
TABLE 7-1 Etiology of Postpartum Hemorrhage

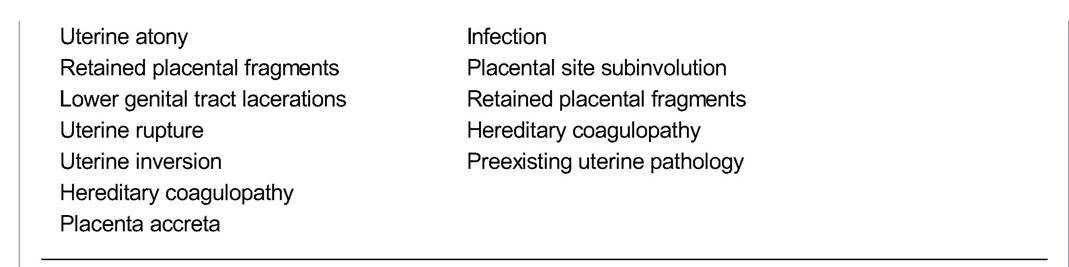
Adapted from American College of Obstetricians and Gynecologists. Practice bulletin no. 76: postpartum hemorrhage. Obstet Gynecol 2006;108:1039-1047, with permission.
• Establish large-bore IV access. Initiate IV fluid resuscitation. Administer supplemental oxygen and order crossmatched blood. After these initial steps, examine the patient to determine the underlying cause and address the problem expeditiously.
• Blood transfusion should be considered after 1 to 2 L EBL and may be initiated earlier if bleeding is expected to continue or the patient is symptomatic.
• Coagulation factors (FFP and cryoprecipitate) and platelets should be repleted with massive blood loss. Historically, one unit of FFP was given for every 4 to 6 units of PRBC to reduce dilutional and citrate coagulopathy as every 500 mL red cells is expected to dilute coagulation factors by 10%.
Additionally, platelets were transfused when the platelet count dropped below 50,000/mL or after 6 to 10 units of red cell transfusion. More recent evidence suggests better outcomes with a protocol of 1:1:1 repletion of PRBC, FFP, and platelets when bleeding is ongoing or massive transfusion (>8 units of PRBC) is needed. In the operative setting, direct manual aortic compression can decrease pulse pressure and slow active bleeding to allow hemodynamic stabilization before proceeding with definitive management.• Factor VII infusion may be considered in extreme cases of hemorrhage with DIC.
Uterine Atony
• Uterine atony (postpartum uterine contraction inadequate for hemostasis) is the most common cause of PPH.
• Normally, uterine contraction after delivery compresses uterine vessels, thereby reducing blood loss. Atony permits continuous brisk bleeding.
• Risk factors include uterine overdistention (as with fetal macrosomia, polyhydramnios, or multiple gestation); prolonged, augmented, or precipitous labor; chorioamnionitis; grand multiparity; and use of tocolytic agents.
• Initial management is bimanual massage of the uterus to stimulate contraction and evacuation of clot from the lower uterine segment to remove a distending mass. Along with oxytocin administration, this is sufficient in most cases.
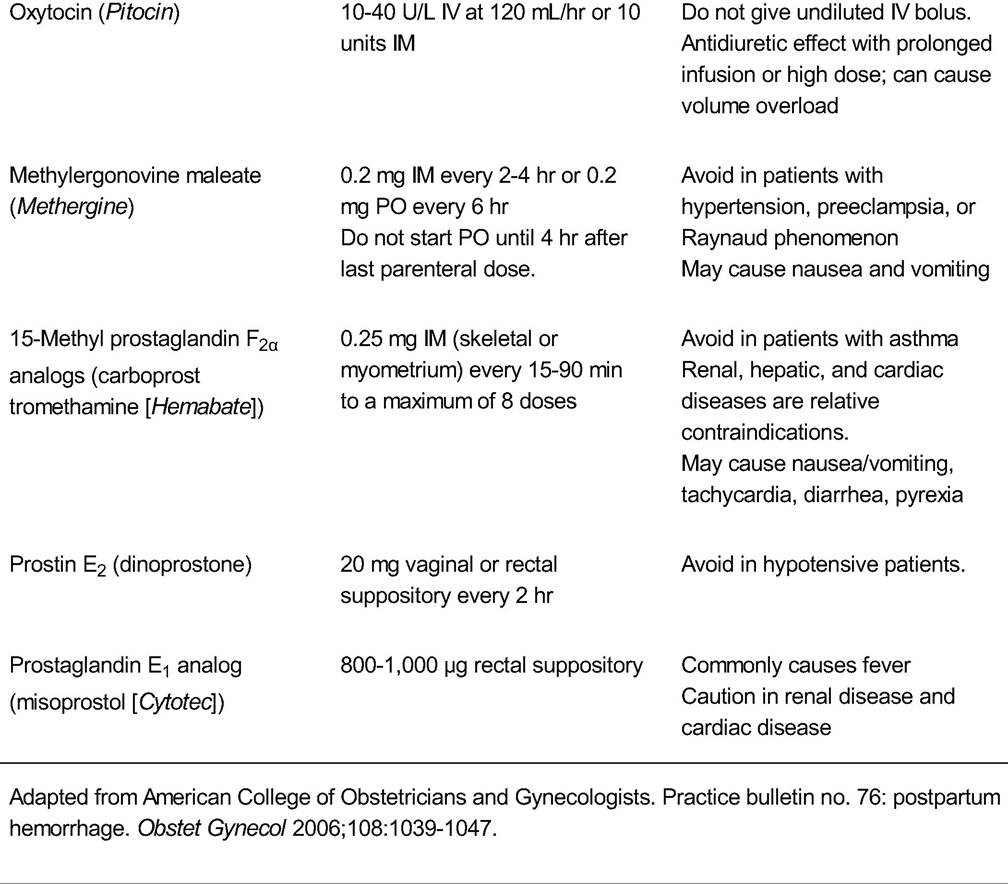
• Procontractile agents can be administered if atony persists (Table 7-2). Oxytocin, methylergonovine, and prostaglandins are appropriate. Rectal misoprostol (800 to 1,000 μg) is often used to stimulate sustained uterine contraction.
P.108
TABLE 7-2 Medical Management of Postpartum Hemorrhage with Uterotonic Agents
Agent
Dose
Comments and
Contraindications
P.109
• Selective uterine arterial embolization may also be considered for continued postpartum atony if the patient is stable for transport to a fluoroscopy suite.
• When these more conservative interventions are unsuccessful, surgical exploration through a vertical midline incision should be considered.
Depending on the patient's desire for future childbearing, the extent of hemorrhage, and the experience of the surgeon, several approaches may be used:• Uterine compressive sutures can be effective for uterine atony. The B-Lynch suture was the original technique described (Fig. 7-1). Since then, multiple compressive sutures have been proposed including combinations of vertical and horizontal sutures to transfix the anterior and posterior uterine walls. All have similar efficacy in achieving hemostasis.
• O'Leary bilateral uterine artery ligation effectively reduces blood loss (Fig. 7-2). After identifying the ureter, ascending branches of the uterine arteries are ligated at the level of the vesicouterine peritoneal reflection. The suture is placed through the lateral lower uterine segment, close to the cervix and then passed through an avascular area of the broad ligament lateral to the uterine vessels. Utero-ovarian vessels (near the cornua) and infundibulopelvic vessels may also be ligated if needed.
• Internal iliac artery ligation (anterior division of the internal iliac/hypogastric artery) significantly decreases uterine pulse pressure, promoting hemostasis. The artery is carefully isolated and ligated with permanent suture such as silk approximately 2 cm distal to the origin of the posterior branch; this placement prevents gluteal ischemia and improves hemostasis by limiting collateral flow to the uterus.
P.110 Care should be taken to avoid injuring the fragile hypogastric vein, ligating the nearby external iliac artery or damaging the ureter. This procedure is not always successful (increased mortality. Intensive care monitoring may be required after peripartum hysterectomy due to massive blood loss, large postoperative fluid shifts, and
potential need for ventilatory support.
Lacerations and Hematomas
• Uterine, vaginal, or cervical laceration should be suspected if the uterine fundus is well contracted but bleeding persists, particularly if operative delivery or episiotomy was performed. Adequate visualization (light and exposure) is mandatory to investigate a laceration. Adequate analgesia is also valuable.
• The cervix, entire vagina, and perineum should be evaluated systematically. Moving to the operating room often facilitates this process with adequate exposure and instrumentation.
• Occult bleeding in vulvar and vaginal hematomas is identified mainly by hypotension and pelvic pain. Stable hematomas may be managed conservatively, but expanding hematomas should be evacuated by performing a generous incision, copiously irrigating, and ligating the bleeding vessels. Layered closure is recommended to assist hemostasis and eliminate dead space. Vaginal packing (for 12 to 18 hours) may be helpful. Broad-spectrum antibiotics should be administered. Arterial embolization may be helpful if unable to be managed surgically.
• Retroperitoneal hematoma is potentially life-threatening due to the volume of blood that can develop in that space. Definitive diagnosis is made via computed tomography (CT) with IV contrast. It may present as hypotension, cardiovascular shock, or flank pain. Stable retroperitoneal bleeding can be managed conservatively.
P.111 The pressure from the expanding hematoma will tamponade vessels and stop blood loss. Continued expansion necessitates surgical exploration or interventional radiology embolization.
Retained Products of Conception
• Retained products of conception can cause PPH.
• Risk factors include accessory placental lobes, abnormal placentation, placenta accreta, chorioamnionitis, and very preterm delivery.
• If retained products are suspected, blunt curettage may be performed. Using large “banjo” curettes with a broad tip under ultrasound guidance may reduce the risk of uterine perforation.
In placenta accreta, the normal plane of separation between uterus and placenta is absent (see Chapter 10). If the third stage of labor lasts longer than 30 minutes, abnormal placentation should be considered. Manual extraction and uterine exploration are performed. Blunt curettage may be required. It may be impossible to remove the entire placenta without damaging the uterus. If bleeding is controlled with uterotonic agents, conservative management may be sufficient.
• Balloon catheter (Bakri balloon) can be placed in the uterus and inflated to tamponade bleeding from abnormal placentation. It may provide complete hemostasis or simply give time to stabilize the patient and arrange additional care, such as uterine artery embolization. The balloon catheter may be left in place for 12 to 24 hours.
• Laparotomy and peripartum hysterectomy are the definitive procedures for bleeding due to placenta accreta.
Coagulopathy
• Coagulopathy can cause or contribute to PPH.
• Risk factors include severe preeclampsia, abruptio placentae, idiopathic/autoimmune thrombocytopenia, AFE, DIC, intrauterine fetal demise, and hereditary coagulopathies (e.g., von Willebrand disease).
• If bleeding is due to coagulopathy, surgical treatment will only increase the hemorrhage. Replete coagulation factors and platelets as needed.
UTERINE INVERSION
In uterine inversion, the uterus is turned inside out, with the fundus protruding through the cervical os into or out of the vagina. It is classified as incomplete if the corpus travels partially through the cervix, complete if the corpus travels entirely through the cervix, and prolapsed if the corpus travels beyond the vaginal introitus.
Incidence
• Occurs in approximately 1 in 2,500 deliveries, usually with a fundal placenta
Etiology and Management
• Risk factors include multiparity, long labor, short umbilical cord, abnormal placentation (i.e., accreta), connective tissue disorders, and excessive traction on the cord.
• Establishment of additional IV access with aggressive fluid resuscitation, anticipating massive PPH. Uterotonics including oxytocin should be discontinued.
• An attempt to replace the uterus manually should be made.
• In the Johnson maneuver, the inverted fundus is grasped and replaced cephalad through the cervix into the normal position. Leaving the placenta in place may
P.112 reduce blood loss; it can be removed manually after normal anatomy is restored. However, if the placenta prevents replacement of the uterus, it should be removed quickly before attempting to push the fundus into place.
• If the maneuver is unsuccessful or a contracted ring of uterine tissue prevents access, uterine-relaxing agents can be administered. The preferred agent is nitroglycerin (up to three doses of 50 to 100 mg IV or sublingual spray); it has a rapid onset of about 30 seconds and a short half-life. Other uterine relaxants such as terbutaline sulfate or halogenated general anesthetics (e.g., halothane, isoflurane) can also be used.
• Uterotonics should be implemented as soon as normal uterine anatomy is restored.
• Laparotomy is indicated if manual restoration fails. Vaginal elevation, upward traction on the round ligaments, or a posterior vertical incision on the lower uterine segment and cervical ring can all facilitate replacement of the fundus.
Chorioamnionitis
Chorioamnionitis is infection/inflammation of the placenta, chorion, and amnion.
Incidence
• Occurs in 1 % to 2% of term and 5% to 10% of preterm deliveries
Etiology and Diagnosis
• Risk factors include nulliparity, prolonged labor, prolonged ruptured membranes, use of internal monitors, maternal bacterial vaginosis, untreated infection, and multiple vaginal examinations.
• Chorioamnionitis is an ascending polymicrobial infection. The most common pathogens are Ureaplasma urealyticum, Mycoplasma hominis, Bacteroides bivius, Gardnerella vaginalis, group B streptococci, and Escherichia coli.
• The diagnosis is clinical. Signs and symptoms include maternal fever 38.0°C or higher without other obvious infection, maternal or fetal tachycardia, uterine tenderness, foul-smelling amniotic fluid or frankly purulent discharge, and leukocytosis (typically >15,000 with a left shift).
• If the diagnosis is uncertain and the clinical situation warrants, amniocentesis may be performed. Positive amniotic fluid culture gives definitive diagnosis. An amniotic fluid white blood cell count >30 cells/pL, glucose level as the neonate may be affected.
• The placenta should be sent to pathology for histologic examination. Membrane culture can be obtained by carefully peeling the amnion and chorion apart and swabbing between the layers. Cord blood may also be sent for culture.
• Unless the patient remains febrile, maternal antibiotics are not indicated beyond one dose after vaginal delivery.
• After cesarean section with chorioamnionitis, broad coverage should be continued for at least one additional dose of antibiotics (8 hours). It may be reasonable to continue antibiotics for as long as 48 hours after the last recorded temperature of 38.0°C or higher. Gentamicin and clindamycin is the typical regimen, but ampicillin can be added to achieve broader coverage (especially for enterococcus).
POSTPARTUM ENDOMYOMETRITIS
Postpartum endomyometritis is infection of the endometrium, myometrium, and parametrial tissues.
Incidence
• About 5% of vaginal deliveries and 10% of cesarean deliveries are affected by postpartum uterine infection. Rates are significantly higher in women of lower socioeconomic status.
Etiology and Diagnosis
• Risk factors include cesarean section, maternal diabetes mellitus, manual removal of the placenta, and all of the risks for chorioamnionitis.
• Endomyometritis, like chorioamnionitis, is an ascending polymicrobial infection often caused by normal vaginal flora.
• May develop immediately to several days after delivery
• Diagnosis is clinical: fever 38.0°C or greater on two separate occasions >2 to 4 hours apart or single temperature >39.0°C, uterine tenderness, tachycardia, purulent vaginal discharge, and associated findings such as dynamic ileus, pelvic peritonitis, pelvic abscess, and bowel obstruction.
• Endometrial cultures are unnecessary; they are typically contaminated by normal flora and yield results much later than clinically required. Blood culture is indicated only for the most severe cases with concern for sepsis.
Management
• Acceptable broad-spectrum antibiotic regimens include:
• Therapy with gentamicin and clindamycin +/- ampicillin until 24 to 48 hours afebrile.
P.114
• Alternate single-agent therapies include ertapenem, ceftriaxone, cefotetan, Unasyn, Zosyn, or Timentin. The aim is broad polymicrobial coverage.
• Gentamicin is administered every 8 hours before delivery. For postpartum treatment, however, several studies show 5 to 7 mg/kg daily dosing is safe, efficacious, and cost-effective. Drug levels are not monitored for daily dosing.
• Endomyometritis typically resolves with 48 hours of antibiotic treatment. Oral antibiotics are not required after completion of IV course.
• If fever persists or patient develops sepsis, additional workup should be considered. This may include urine and blood cultures; chest and abdominal radiographs; pelvic examination; and pelvic/abdominal ultrasound, CT, or magnetic resonance imaging (MRI).
• Infections with clostridia, group A streptococci, and staphylococci should be suspected in patients presenting with sepsis. Group A streptococcal septicemia is the leading cause of peripartum sepsis worldwide but relatively rare in the United States. Toxic shock syndrome may be suspected when there is high fever, desquamation, diffuse macular rash, and multisystem organ failure. In rare cases, postpartum hysterectomy has been reported for uterine myonecrosis.
SEPTIC PELVIC THROMBOPHLEBITIS
Septic pelvic thrombophlebitis (SPT) exists in two forms: ovarian vein thrombosis/thrombophlebitis and deep pelvic septic thrombophlebitis. SPT occurs in 1 in 2,000 to 1 in 3,000 deliveries, most commonly after cesarean section.
Diagnosis and Etiology
• SPT should be considered in patients with persistent spiking fevers despite 3 days of antibiotic treatment for endometritis. The patient usually appears well between febrile episodes, and pain is minimal. Thrombi form in the deep pelvic veins as a result of pregnancy-induced hypercoagulability and venous congestion. These may become infected, releasing septic emboli which travel to the lungs. Less than 2% of cases have pulmonary emboli by imaging. When other causes of postpartum fever have been excluded, pelvic ultrasound and pelvic/abdominal CT or MRI help diagnose abscess or large thrombus. A negative result, however, does not rule out SPT, which is largely a diagnosis of exclusion. Blood cultures are typically negative.
Management
• As SPT is often a diagnosis of exclusion in patients with persistent fever, most are already being treated with broad-spectrum antibiotics, which also cover the typical pathogens of endomyometritis. Once the diagnosis is suspected, anticoagulation with heparin or enoxaparin is initiated.
• Heparin theoretically terminates embolic showers that may cause the spiking fever. Therapeutic IV heparin infusion may be initiated with a 5,000-unit heparin bolus, then a continuous infusion (usually 16 to 18 mm/kg/hr) with an activated partial thromboplastin time ratio (aPTT r) goal of 1.5 to 2.0 times normal. Low molecular weight heparin at a dose of 1 mg/kg every 12 hours is also acceptable.
• Antibiotics may be continued until the patient is 24 to 48 hours afebrile. The duration of anticoagulation is somewhat controversial, with recommendations ranging from 24 hours to 2 weeks after the last fever. If imaging clearly detects a deep vein
P.115 or pulmonary thrombus, 6 months of anticoagulation with warfarin or enoxaparin are indicated.
MECONIUM ASPIRATION
Meconium staining of the amniotic fluid complicates 7% to 20% of all live births. It increases the risk of neonatal respiratory disorders. Of infants born through meconium-stained fluid, 2% to 10% are subsequently diagnosed with meconium aspiration syndrome, with a mortality rate of up to 12%.
Etiology and Complications
• Fetal acidosis, fetal heart rate abnormalities, and low Apgar scores are associated with meconium- stained fluid. Fetal stress and hypoxia stimulate meconium passage. The majority of pregnancies complicated by meconium-stained amniotic fluid, however, result in normal healthy newborns.
• Aspiration has three major pulmonary effects: (a) airway obstruction, (b) surfactant dysfunction, and (c) chemical pneumonitis.
• Risk factors for meconium aspiration syndrome include moderate or thick meconium, nonreassuring fetal heart rate tracing, meconium below the cords, and low Apgar scores.
Management
• Amnioinfusion is no longer used for all cases of meconium. A large multicenter trial showed that amnioinfusion for thick meconium did not reduce the risk of moderate or severe meconium aspiration syndrome, perinatal death, or other major neonatal complications.
• The most recent Neonatal Resuscitation Program guidelines advise against routine intrapartum suctioning for infants with meconium-stained fluid. A large multicenter trial showed that deep suctioning before delivery of the shoulders did not reduce the rate of intubation, meconium aspiration syndrome, the need for mechanical ventilation, or overall mortality. After delivery, the infant should be passed to the pediatric team with minimal stimulation, with endotracheal suctioning performed for nonvigorous infants.
SUGGESTED READINGS
Conde-Agudelo A, Romero R. Amniotic fluid embolism: an evidence-based review. Am J Obstet Gynecol 2009;201:445.e1-e13.
French LM, Smaill FM. Antibiotic regimens for endometritis after delivery. Cochrane Database Syst Rev 2004;(4):CD001067.
Mousa HA, Alfirevic Z. Treatment for primary postpartum haemorrhage. Cochrane Database Syst Rev2007; (1):CD003249.
Tomacruz RS, Bristow RE, Montz FJ. Management of pelvic hemorrhage. Surg Clin North Am 2001;81(4):925-948.
Vain NE, Szyld EG, Prudent LM, et al. What (not) to do at and after delivery? Prevention and management of meconium aspiration syndrome. Early Hum Dev 2009;85:621-626.
Xu H, Hofmeyr J, Roy C, et al. Intrapartum amnioinfusion for meconium-stained amniotic fluid: a systematic review of randomised controlled trials. BJOG 2007;114:383-390.
You WB, Zahn CM. Postpartum hemorrhage: abnormally adherent placenta, uterine inversion, and puerperal hematomas. Clin Obstet Gynecol 2006;49:184-197.