8 Gestational Complications
Meghan E. Pratts
Janice Henderson
This chapter reviews several common antenatal complications:
• Amniotic fluid disorders (including oligohydramnios, polyhydramnios)
• Intrauterine growth restriction Cervical insufficiency
• Multiple gestation
• Postterm pregnancy
• Fetal demise in utero (FDIU)
AMNIOTIC FLUID DISORDERS
• Amniotic fluid volume (AFV) represents the balance between production and removal of fetal fluids.
• In early gestation, fluid is produced from the fetal surface of the placenta, from transfer across the amnion, and from embryonic surface secretions.
• In mid to late gestation, fluid is produced by fetal urination and alveolar transudate. By 16 weeks, there is about 250 mL of fluid, increasing to approximately 800 mL by 34 to 36 weeks' gestation.
• Fluid is removed by fetal swallowing and absorption at the amnion-chorion interface.
• The most accurate measurement of AFV is by dye dilution techniques or direct measurement at the time of hysterotomy. Ultrasound provides a standard noninvasive tool to estimate AFV (Table 8-1).
• Polyhydramnios is the pathologic accumulation of amniotic fluid defined as more than 2,000 mL at any gestational age, more than the 95th percentile for gestational age, or an amniotic fluid index (AFI) >25 cm at term.
• The incidence of polyhydramnios in the general population is about 1%.
• Implications: Mildly increased AFV is usually clinically insignificant. Markedly increased AFV is associated with increased perinatal morbidity due to preterm labor, cord prolapse upon membrane rupture, underlying comorbidities, and congenital malformations. Abruptio placentae is associated with polyhydramnios and rupture of membranes due to rapid decompression of the overdistended uterus. Increased maternal morbidity also results from postpartum hemorrhage due to uterine overdistention leading to atony.
If polyhydramnios is severe, uterine distention can cause venous and ureteral compression causing severe lower extremity edema and hydronephrosis.• The most common etiology of polyhydramnios is idiopathic (Fig. 8-1); however, in severe cases, a cause is more often apparent and likely to be associated with a detectable fetal anomaly. Specific causes include:
î Fetal structural malformations: In cases of acrania or anencephaly, polyhydramnios occurs from an impaired swallowing mechanism, low antidiuretic
P.117 hormone causing polyuria, and possibly transudation across the exposed fetal meninges. Gastrointestinal tract anomalies may also lead to polyhydramnios by either direct physical obstruction or decreased absorption. Ventral wall defects increase AFV from transudation across the peritoneal surface or bowel wall.
TABLE 8-1 Methods of Amniotic Fluid Assessment
| Diagnostic Method | Interpretation | Clinical Value |
| Maximum vertical pocket (MVP) | Oligo ≤2 cm Normal = 2.1-8 cm Poly ≥8 cm | ■ 94% concordant with dye-determined normal pregnancies ■ Less accurate for low AFV ■ Useful predictor of adverse events |
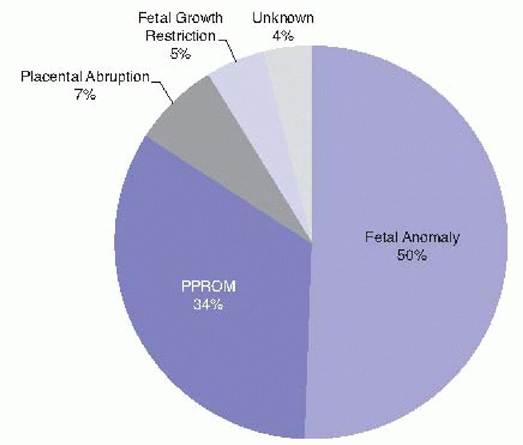
| Amniotic fluid index (AFI)— measurement and summation of deepest pocket in each of four quadrants | Oligo of cases. Cord compression leads to increased incidence of fetal heart rate decelerations in labor. • The etiology of oligohydramnios includes ruptured membranes, fetal urinary tract malformations, postterm pregnancy, placental insufficiency, and medications reducing fetal urine production. Rupture of membranes must be considered at any gestational age. Renal agenesis or urinary tract obstruction often becomes apparent during the second trimester of pregnancy, when fetal urine flow begins to contribute significantly to AFV. Placental insufficiency can cause both oligohydramnios and intrauterine growth restriction. The cause of oligohydramnios in postterm pregnancies may be deteriorating placental function (Fig. 8-2).• Ultrasound is used to diagnose oligohydramnios. Rupture of membranes should be evaluated, and in cases of preterm gestation with uncertain membrane status, a tampon dye test can be performed (see Chapter 9). • Treatment for oligohydramnios is limited. Maternal intravascular fluid status appears to be closely tied to that of the fetus; maternal hydration (intravenous or oral) may improve the AFV depending on the etiology of oligohydramnios. In cases of obstructive genitourinary defects, in utero surgical diversion has produced P.120 some promising results. For optimal benefit, urinary diversion must be performed before renal dysplasia develops and early enough in gestation to permit normal lung development. Until near term, oligohydramnios is managed with frequent fetal surveillance. Indications for induction of labor include term gestation or nonreassuring fetal testing after 34 weeks. Oligohydramnios is not a contraindication to labor. There is no consensus as to which of the measurements of AFV is most recommended when deciding if induction for oligohydramnios is indicated. MVP may be a superior option to AFI, as AFI measurement has a higher rate of false positives for oligohydramnios and thus increases induction and cesarean section rates without evidence of improvement in neonatal outcomes.
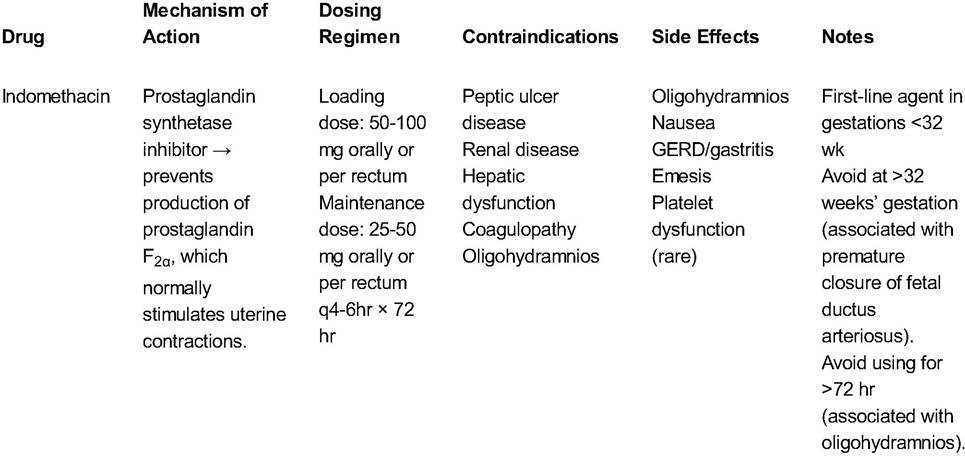
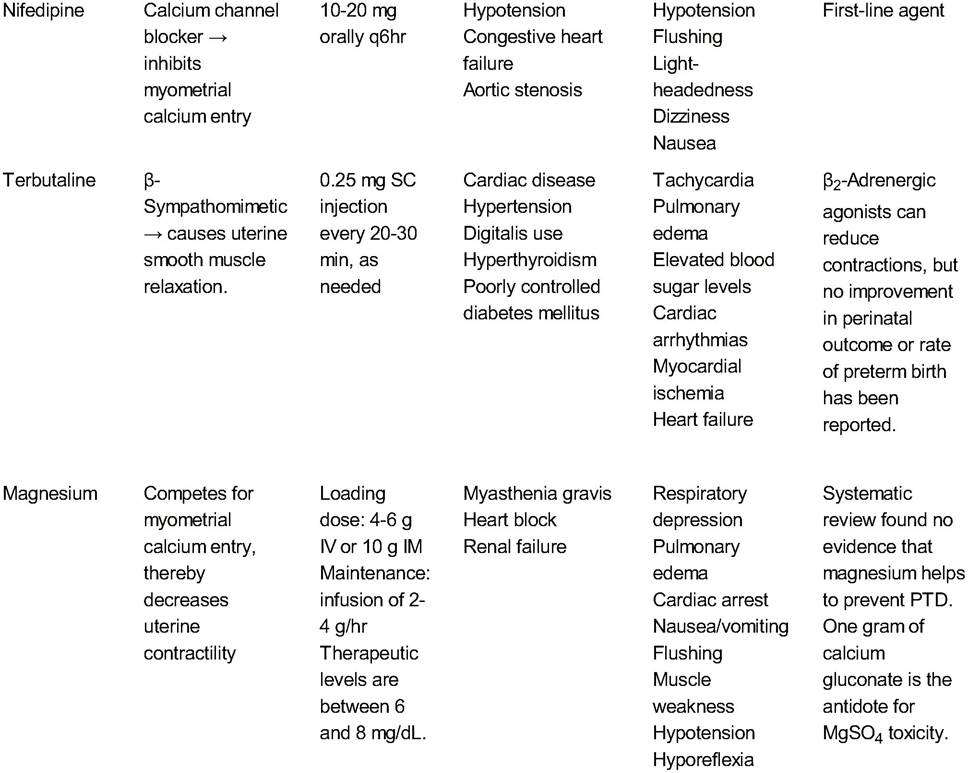
Figure 8-2. Causes of oligohydramnios. PPROM, preterm premature rupture of membranes. (Adapted from Shipp TD, Bromley B. Outcome of singleton pregnancies with severe oligohydramnios in the second and third trimesters. Ultrasound Obstet Gynecol 1996;7[2]:108-113.) INTRAUTERINE GROWTH RESTRICTION Intrauterine growth restriction (IUGR) is suggested when the estimated fetal weight falls below the 10th percentile for gestational age. Approximately 70% of socalled IUGR is merely constitutional, although underlying etiology may be difficult to elucidate. The incidence of pathologic IUGR is between 4% to 8% of gestations in developed countries and 6% to 30% in developing countries. Fetuses with IUGR have a two- to sixfold increase in perinatal morbidity and mortality. Asymmetric versus symmetric IUGR may suggest etiology. In symmetric IUGR, the fetus is proportionally small, whereas in asymmetric IUGR, abdominal growth lags behind head circumference. Symmetric growth restriction implies an early insult such as chemical exposure, infection, or aneuploidy. Asymmetric growth is more associated with a late pregnancy insult such as placental insufficiency.• The etiology of IUGR includes both maternal and fetal causes: • Constitutionally small mothers and inadequate weight gain: Women who weigh must be rigorously sought. Although prophylactic cervical cerclage has only been shown to be beneficial after three or more second-trimester pregnancy losses due to CI, patient concerns and provider judgment rarely tolerate waiting so long before proceeding with elective preventive treatment (i.e., cerclage). Cervical funneling on ultrasound is not adequate justification for cerclage placement, although serial cervical ultrasound of high-risk women starting at 16 to 20 weeks may identify those pregnancies requiring additional management (see Chapter 11). • Admittedly, diagnosis of CI and selection of patients for elective cervical cerclage are as much art as science. • Pelvic rest, pessary placement, and cervical cerclage have been suggested to prevent repeated pregnancy loss from CI, but the evidence for their effectiveness is mixed. A careful review of maternal history and prior pregnancy losses, complete counseling on the risks and benefits of cerclage (e.g., preterm premature rupture of membrane, chorioamnionitis, preterm birth, cervical laceration), and early screening for aneuploidy and congenital anomalies (see Chapter 12) should be offered before proceeding with cerclage placement. Ideally, cerclage placement should occur before the onset of cervical dilation. Once dilation occurs, a rescue cerclage may be placed.• McDonald or Shirodkar cerclages are placed vaginally, usually at 12 to 14 weeks' gestation; selection of technique depends on the available cervical length and surgeon experience/preference. Prophylactic antibiotics and postoperative tocolysis have not been shown to affect outcome but are often employed. The risk of iatrogenic pregnancy loss ranges from 1 % to nearly 20% for elective cases. Rescue cerclage for CI/bulging membranes is associated with >50% risk of complications. P.123 Abdominal cerclage is placed at laparotomy in rare instances for women who have minimal to no residual cervical length (often due to large cone biopsies or trachelectomy). Subsequent cesarean section is necessary. • Cerclage is removed when the patient begins to labor, when membranes rupture, if there is evidence of uterine infection, or if the patient reaches 36 weeks' gestation. MULTIPLE GESTATION Multiple gestation occurs in approximately 3% of all births in the United States and is increasing annually due to assisted reproductive technologies (ART). The incidence of monozygotic twins is constant at approximately 4 in 1,000 gestations. The incidence of dizygotic twins varies widely and is higher in some families; in individuals of African descent; with ovulation induction and in vitro fertilization; and with increasing maternal age, parity, weight, and height. In the absence of fertility drugs, triplet pregnancies occur in approximately 1 in 8,000 gestations. Higher order births are much rarer. Multiple gestation increases morbidity and mortality for both mother and fetus. Perinatal mortality rates in developed countries range from 50 to 100 per 1,000 births for twins and from 100 to 200 per 1,000 births for triplets. • Diagnosis is confirmed by sonogram most accurately in the first trimester when separate gestational sacs are easily seen to determine chorionicity. In later gestations, sonogram can detect the “twin-peak” sign also known as the “lambda sign” for dichorionic twins and the Tsign for monochorionic diamnionic twins. Multiple gestation is suspected if uterine size is greater than expected for gestational age, multiple fetal heart rates are detected, multiple fetal parts are felt, the human chorionic gonadotropin (hCG) and maternal serum alphafetoprotein levels are elevated for gestational age, or the pregnancy is a result of ART.• Zygosity, placentation, and mortality • Dizygotic dichorionic/diamnionic twins (70% to 80% of all twins) result from the fertilization of two ova. Each fetus has its own placenta and a complete and separate amnion-chorion membrane. • Monozygotic twins (20% to 30% of all twins) result from cleavage of a single, fertilized conceptus. The timing of cleavage determines the placentation. î Dichorionic/diamnionic monozygotic twins (8% of all twins) are produced by cleavage in the first 3 days after fertilization. They will have separate amnions and chorions, just like dizygotic twins. They have the lowest perinatal mortality rate (uterine growth between 20 and 30 weeks' gestation from polyhydramnios of the recipient twin is common. TTTS can be diagnosed when sonography suggests a single chorion, discordant fetal growth, polyhydramnios around the larger twin, and oligohydramnios around the smaller fetus (“stuck twin” sign or “poly-oli” syndrome). The severity and timing of growth discrepancy depend on the degree of arteriovenous shunting. Fetal hydrops is an ominous sign. P.125 î If extreme prematurity prevents immediate delivery, management includes serial amnioreduction for the recipient twin, intrauterine blood transfusion for the donor twin, selective fetal reduction, or fetoscopic laser ablation of placental anastomoses. • Antenatal management of multiple gestations includes adequate nutrition (300 additional calories per day per fetus), more frequent prenatal visits, periodic ultrasound assessment of fetal growth and well-being, and prompt hospital admission for preterm labor or obstetric complications. No evidence supports bed rest or prophylactic tocolytics in multiple gestations. In addition, neither prophylactic cerclage or progesterone therapy have been shown to reduce preterm birth rates in multiples and cerclage specifically may worsen outcomes. • Ultrasonographic assessments should be conducted every 3 to 4 weeks from 23 weeks' gestation to monitor fetal growth and detect discordance. Monochorionic placentation may warrant ultrasonography every 2 weeks to evaluate for evidence of TTTS. • Fetal surveillance with nonstress testing (NST) is not indicated for dizygotic twins unless clinical or ultrasonographic data suggest IUGR or discordance. When NSTs are discordant, additional testing may be necessary. The use of contraction stress testing is controversial and rarely used as it might precipitate preterm delivery. • Amniocentesis should be performed for both fetuses, if indicated, for prenatal diagnosis of genetic disorders or alloimmunization. One to 5 mL of indigo carmine is injected into the first sac following fluid aspiration to ensure that both sacs are sampled. To establish lung maturity, amniotic fluid evaluation from one fetal sac is adequate. For discordant twins, amniotic fluid should be obtained from the larger twin, which usually reaches pulmonary maturity later. • Multifetal pregnancy reduction may be offered to reduce risk in higher order pregnancies. Because the presence of three or more fetuses is associated with such increased maternal and perinatal mortality and morbidity, fetal reduction may be appropriately offered. The risk of subsequent pregnancy loss is 5% to 10%. Selective termination refers specifically to the termination of one or more specific fetuses with structural or chromosomal anomalies. • Management of fetal demise is based on gestational age and the condition of the surviving fetus. Until the surviving twin develops lung maturity, weekly fetal surveillance and maternal coagulation profile testing should be performed. Consider delivery when fetal lung maturity is demonstrated, if fetal status deteriorates, or if disseminated intravascular coagulation (DIC) develops in the mother. In TTTS, one fetal demise should prompt consideration for delivery, particularly after 28 weeks. • The optimal route of delivery for twins remains controversial and should be assessed on a case-by-case basis. Decisions about delivery must consider the presentations, gestational age, maternal or fetal complications, the experience of the obstetrician, and the availability of anesthesia and neonatal intensive care support. • VertexZvertex (43%) presentation can have a successful vaginal delivery in 70% to 80% of cases. Surveillance of twin B between deliveries is advised. • VertexZnonvertex (38%) presentation can have a vaginal delivery if estimated fetal weights are concordant. External cephalic version or internal podalic version and breech extraction of twin B may be attempted. Vaginal delivery of twin B in nonvertex presentation may be considered for infants with an estimated weight P.126 between 1,500 and 3,500 g. Success rates are more than 96%. There is insufficient data to advocate a specific route of delivery for a second twin weighing occur before 32 weeks' gestation, 20% occur between 36 and 40 weeks' gestation, and approximately 10% occur beyond 41 weeks' gestation. • FDIU is suspected with any maternal report of more than a few hours of absent fetal movement. Definitive diagnosis is by absent fetal cardiac activity on real-time ultrasonography. • Fetal deaths can be categorized by occurrence during the antepartum period or during labor (intrapartum stillbirth). The antepartum fetal death rate in an unmonitored population is approximately 8 in 1,000 and represents 86% of fetal deaths. • The etiology of antepartum fetal death can be divided into broad categories: chronic hypoxia of diverse origin (30%), congenital malformation or chromosomal anomaly (20%), complications of pregnancy such as Rh alloimmunization (suppositories (90 to 200 mg) every night at bedtime • Progesterone has been shown to prolong gestation for women with prior history of PTL. • Vaginal progesterone has been shown to prolong gestation for women with a short cervix weeks, indomethacin. (Table 9-1). • Use of multiple tocolytics concurrently should be avoided given the risk of pulmonary edema (excluding indomethacin). • GBS prophylaxis is continued until cervical exam is stable and risk for progression to PTD is lower. • Antibiotic prophylaxis is not indicated outside of concern for active labor. • Prolonged empiric antibiotics in the case of intact membranes may increase neonatal risk of sepsis. • Corticosteroids should considered between 24 and 34 weeks' gestation. • Give two doses of betamethasone (12 mg IM) 24 hours apart or four doses of dexamethasone (6 mg IM) 12 hours apart. î Benefit is optimized 24 hours after the second dose and remains up to 1 week after administration. • Corticosteroid administration reduces risk for neonatal respiratory depression, intraventricular hemorrhage, necrotizing enterocolitis, and neonatal death. P.134 P.135 TABLE 9-1 Common Tocolytic Agents for Preterm Labor
GERD, gastroesophageal reflux disease; SC, subcutaneous; IV, intravenous; IM, intramuscular; PTD, preterm delivery; MgSO4, magnesium sulfate. P.136 • A single rescue course of two doses of steroid administration at 28 to 34 weeks 7 or more days after earlier administration may be considered with little additional neonatal risk and potential benefit. î We often redose betamethasone once at least 2 weeks after initial dose if imminent delivery is again suspected. î Particularly if prior dose was given at 30 weeks or earlier • Serial courses or additional doses are not indicated and are associated with growth restriction and neonatal morbidity. • Corticosteroids increase maternal white blood cell count and serum glucose, so exercise caution in interpreting those lab values. î Glucose monitoring is required if given to diabetics or suspected diabetics due to risk for hyperglycemia and morbidity. î This effect peaks with approximately 50% increased insulin requirements at 2 to 3 days and lasts about 5 days. • Magnesium should be considered between 24 and 32 weeks of gestation for fetal neuroprotection. • Meta-analysis of studies evaluating intravenous magnesium have demonstrated that its administration can help decrease the combined outcome of neonatal death or cerebral palsy. î Studies included in the meta-analysis used different doses of magnesium infusions î 4 g bolus î 1g∕hr for 24 hours î 2 g/hr for 12 hours • It is generally accepted to use any of these proposed regimens for neonatal neuroprotective effects. We generally consider a 4 gram bolus followed by magnesium at 1g/hr for 24 hours or until delivery. At 24 hours, the patient is re-evaluated and the magnesium may be continued if delivery is felt to be imminent. Additionally, magnesium infusions that are discontinued are considered to be restarted if delivery is felt to be imminent in the future, prior to 32 weeks' gestation. • Fetal monitoring • No optimal schedule of fetal testing has been established. î Maintain external fetal monitoring/tocodynamometry until active PTL resolves (i.e., no cervical change and minimal contractions). î Once PTL resolves, there is no need for further continuous monitoring. On our inpatient unit, we check fetal doptones one to two times daily with vital signs and perform a fetal nonstress test one to three times per week. • Route of delivery varies by gestational age • If 800 g, Csection should be considered to minimize neonatal morbidity. î C-section for breech presentation is performed to minimize the risk of head entrapment and associated morbidity. P.137 • Criteria for discharge include acontractile, stable cervical exam (without advanced cervical dilation [>4 cm], bulging membranes, or significant effacement), no vaginal bleeding, no suspicion of ruptured membranes, reasonable hospital access with appropriate level of neonatology support, ability to comply with activity recommendations (modified bed rest and complete pelvic rest), and reassuring fetal status (we typically perform a nonstress test on the day of discharge). PRETERM PREMATURE RUPTURE OF MEMBRANES Preterm premature rupture of membranes (PPROM) can be defined as spontaneous rupture of the amnion and chorion membranes before the onset of labor (premature rupture of membranes [PROM]) or PROM before 37 weeks' gestation. The latency period is the time from PROM or PPROM to onset of labor. At term, latency is 1 to 12 hours on average. Incidence and Significance • Term PROM occurs in up to 19% of pregnancies. • PPROM occurs in approximately 30% of pregnancies and accounts for 30% of PTD. • Fifty percent of patients with PPROM before 26 weeks will labor within 1 week. • Fifty percent of patients with PPROM between 28 and 34 weeks will labor within 24 hours; 80% to 90% will labor within 1 week. Etiology • Risk factors include intrauterine infection, prior history of PPROM, trauma, amniocentesis, and polyhydramnios. Evaluation • Same as for PTL (see earlier discussion). Make careful note of the circumstances, character, and timing of rupture of membranes (ROM) and the consistency of the fluid. • Only an SSE should be performed. Avoid digital cervical exam unless delivery is imminent. Digital examination decreases the latency period and increases the risk of neonatal sepsis. • When clinical suspicion of PROM is high despite negative ferning, nitrazine, and pooling, retest after prolonged recumbency (several hours). • Consider amnioinfusion of indigo carmine (1 ml in 9-ml sterile normal saline) for a “tampon test.” A tampon or packing is placed in the vagina, and dye is injected into the amniotic fluid via the amniocentesis needle. After some time, the tampon is examined to see whether blue-stained fluid has leaked through the cervix. Management Management for PPROM and PTL is similar. • The goals are to screen for underlying chorioamnionitis or placental abruption and move toward delivery if these conditions are identified. Otherwise, prolonging the latent period is desired, depending on gestational age. •If the fetal vertex is not well applied to the cervix, bed rest should be maintained to avoid cord accident. • Before 34 weeks in the absence of chorioamnionitis, initiate latency antibiotics, which delay the onset of PTL. •The standard latency regimen is intravenous ampicillin 2 g and erythromycin 250 mg every 6 hours for 48 hours. P.138 • This is followed by oral amoxicillin 250 mg and erythromycin 330 mg every 8 hours (or 250 mg erythromycin every 6 hours) for 5 more days. • In cases of penicillin allergy, cephalosporins can replace amoxicillin if the allergic reaction is mild, or clindamycin and gentamycin can be considered if the allergic reaction is severe (e.g., angioedema). •The entire latency course is 7 days. • Tocolysis is generally contraindicated in PPROM except for extreme prematurity to allow corticosteroid administration. • If chorioamnionitis is suspected, tocolysis is contraindicated. • Once the patient and fetus are stable, fetal heart tones should be evaluated every 8 hours and daily fetal testing performed. • At vaginal or cervical lacerations and the amount of bleeding. Laboratory Tests • Complete blood cell count with hematocrit and platelets (150 mg/dL, hematocrit >25%, and platelets >60,000φL. • Once the mother is stabilized, proceed to urgent cesarean section, unless vaginal delivery is imminent. Preterm Gestation, Hemodynamically Stable • Eighty-two percent of patients with evidence of AP at transabdominal scan, especially if the placenta lies in the posterior portion of the lower uterine segment where it is poorly visualized. Having the patient empty her bladder may help in identifying anterior PP. Trendelenburg position may be useful in diagnosing posterior PP. If ultrasound findings are suspicious for accreta, magnetic resonance imaging (MRI) may be helpful in making the diagnosis, particularly with a posterior placenta. • If PP is present or suspected, digital examination is contraindicated. A gentle speculum exam can be used to evaluate the presence and quantity of vaginal bleeding, but in most cases, this can be assessed adequately by inspecting the perineum and thereby avoid exacerbating the hemorrhage. Laboratory Studies • Complete blood cell count • Type and crossmatch • Prothrombin time and activated thromboplastin time • Kleihauer-Betke test to assess for fetomaternal hemorrhage in Rh-negative unsensitized patients. Not useful for the diagnosis of PP. • Apt test (as described earlier for abruption) P.144 Management • In general, patients diagnosed with PP but without bleeding in the third trimester should have ultrasound confirmation of persistent previa. They should maintain strict pelvic rest (i.e., nothing in the vagina, including intercourse or pelvic exams) and avoid strenuous activity or exercise. They should receive advice about when to seek medical attention and be scheduled for fetal growth ultrasounds every 3 to 4 weeks. • In general, patients with PP who are bleeding should be hospitalized for hemodynamic stabilization and continuous maternal and fetal monitoring. Laboratory studies should be ordered as described. Steroids are administered to promote lung maturity for gestations between 24 and 34 weeks, and Rh D immunoglobulin should be administered to Rh-negative mothers. • Management of placenta accreta, or its variants, can be challenging. In patients with PP and a prior history of cesarean section, cesarean hysterectomy may be required. In cases where uterine preservation is highly desired and no bladder invasion has occurred, bleeding might be successfully controlled with selective arterial embolization or packing of the lower uterine segment, with removal of the pack through the vagina in 24 hours. The Bakri balloon catheter has also been used to help control bleeding from the placental bed. • Specific management of PP is based on gestational age and assessment of the maternal and fetal status. Term Gestation, Hemodynamically Stable • Patients with complete previa at term require cesarean section. • Patients with partial or marginal previa at term may deliver vaginally, with thorough consent regarding risks for blood loss and need for transfusion. The staff and facilities for immediate emergent cesarean section must be available. If maternal or fetal stability is compromised at any point in labor, urgent cesarean section is performed. Term Gestation, Hemodynamic Instability • Stabilize the mother with fluid resuscitation and blood products • Delivery via cesarean section is indicated for nonreassuring fetal heart monitoring, life-threatening maternal hemorrhage, or bleeding after 34 weeks with documented fetal lung maturity. If the mother is stable and intrauterine fetal loss occurs or the fetus is 48 hours, no other complications exist, and the following criteria are met: • The patient can maintain bed rest at home and is adherent to medical care. • There is a responsible adult present at all times who can assist in an emergency. • The patient lives near the hospital with dependable transportation. • For preterm gestations with PP and contractions, it can be difficult to diagnose labor. Cervical exams are contraindicated, and 20% of patients with PP show some uterine activity. If the patient and fetus are stable, tocolysis may be considered with magnesium sulfate. As with AP, terbutaline, nifedipine, and indomethacin should be avoided. Preterm Gestation, Hemodynamic Instability • Appropriate stabilization and resuscitation are initiated with rapid delivery by cesarean section. VASA PREVIA VP occurs when the umbilical cord inserts into the membranes instead of the central placental disc. When the vessels traverse the membranes near the internal os in advance of the fetal presenting part, they are at risk of rupture, causing fetal hemorrhage. VP can also occur when a velamentous cord insertion or vessels to an accessory lobe are located near the cervical os. Velamentous cord insertion is much more common in multiple gestations. Epidemiology • The incidence of VP is estimated to be approximately 1 in 5,000 pregnancies. • Fetal mortality may be as high as 60% with intact membranes and 75% when membranes rupture. Etiology • The cause of VP is unknown. Because of the association between velamentous cord insertion, multiple gestations, and VP, one theory suggests that it develops due to trophoblastic growth and placental migration toward the more vascular uterine fundus. The initial cord insertion at the center of the placenta becomes more peripheral as one portion of the placenta actively grows and another portion does not. In vitro fertilization (IVF) may also be a risk factor. Complications • Even small amounts of fetal hemorrhage can result in morbidity and possible death due to the small total fetal blood volume. • Rupture of the membranes can result in rapid exsanguination of the fetus. History • The patient usually presents with acute onset vaginal bleeding after rupture of membranes. P.146 • The bleeding is associated with an acute change in fetal heart pattern. Typically, fetal tachycardia occurs, followed by bradycardia with intermittent accelerations. Shortterm variability is often maintained. Occasionally, a sinusoidal pattern may be seen. Diagnosis • Transvaginal ultrasound, in combination with color Doppler ultrasonography, is the most effective tool in antenatal diagnosis. • In one study, there was a 97% survival rate in cases diagnosed antenatally compared to a 44% survival rate in those without prenatal diagnosis. Management • Third-trimester bleeding caused by VP is often accompanied by acute and severe fetal distress. Emergency cesarean section is indicated. • If VP is diagnosed antenatally, planned cesarean section should be scheduled at 36 to 38 weeks under controlled circumstances and before the onset of labor to reduce fetal mortality. Earlier delivery can be considered with documented fetal lung maturity. SUGGESTED READINGS Love CD, Wallace EM. Pregnancies complicated by placenta praevia: what is appropriate management? Br J Obstet Gynecol 1996;103(9):864-867. Magann EF, Cummings JE, Niederhauser A, et al. Antepartum bleeding of unknown origin in the second half of pregnancy: a review. Obstet Gynecol Surv2005;60(11):741-745. McCormack RA, Doherty DA, Magann EF, et al. Antepartum bleeding of unknown origin in the second half of pregnancy and pregnancy outcomes. BJOG 2008;115(11):1451-1457. Oyelese Y, Smulian JC. Placenta previa, placenta accreta, and vasa previa. Obstet Gynecol 2006; 107(4):927-941.
More medical literature on Medic.Studio
More on the topic 8 Gestational Complications:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|