11 Perinatal Infections
Stephen Martin
Andrew J. Satin
Perinatal infections encompass a range of viruses, parasites, and bacteria that can be transmitted during pregnancy from mother to embryo or fetus.
Infection can occur antepartum or intrapartum by transplacental or transcervical transmission, respectively. The acronym TORCH was originally used to characterize perinatal infections including toxoplasmosis, “other,” rubella, cytomegalovirus, and herpes simplex virus. The expansive “other” has grown to include, but is not limited to, parvovirus, syphilis, group B Streptococcus, hepatitis, and influenza.Asymptomatic or undiagnosed maternal disease can result in significant fetal and neonatal morbidity and mortality. For this reason, it is important to understand the clinical manifestations, diagnostic criteria, and management of these perinatal infections.
P.147
VIRUSES
Cytomegalovirus
Epidemiology
• Cytomegalovirus (CMV) is the most common congenital viral infection, with intrauterine infection occurring in 0.2% to 2.5% of live births. CMV is a ubiquitous DNA herpes virus, with approximately 50% of the US population having antibodies to CMV. Transmission occurs through direct contact with infected saliva, semen, cervical and vaginal secretions, urine, breast milk, or blood products. Vertical transmission can occur transplacentally, during delivery, or postpartum. An estimated 40,000 infants are born with CMV infection in the United States annually.
Clinical Manifestations
• Maternal infection: In immunocompetent adults, CMV infection is typically silent. Symptoms, however, can be flu-like, including fever, malaise, swollen glands, and rarely hepatitis. After the primary infection, the virus becomes dormant, with periodic episodes of reactivation and viral shedding.
• Congenital (fetal) infection: Most fetal infections are due to recurrent maternal infection and lead to congenital abnormalities in approximately 1.4% of cases.
Previously acquired maternal immunity confers protection from clinically apparent disease by maternal antibodies. Mothers determined to be seronegative for CMV before conception or early in gestation have a 1 % to 4% risk of acquiring the infection during pregnancy and 30% rate of fetal transmission after seroconversion.• Approximately 90% of infants with congenital CMV infection will be asymptomatic at birth. Ten percent to 15% of these may later develop symptoms including developmental delay, hearing loss, and visual and dental defects.
• Unlike recurrent infection, primary maternal infection during pregnancy can often lead to serious neonatal sequelae with neonatal mortality of approximately 5% but as high as 30% in some investigations. Approximately 5% to 20% of newborns of mothers with primary CMV infection are overtly symptomatic at
birth. Infection in the first trimester leads to higher risk of sequelae than in the third trimester.
• The most common clinical findings at birth include the presence of petechiae, hepatosplenomegaly or jaundice, and chorioretinitis. These symptoms constitute fulminant cytomegalic inclusion disease. Infants show signs of respiratory distress, lethargy, and seizures. Long-term sequelae include mental retardation, motor disabilities, and hearing and visual loss.
Diagnosis
• Maternal CMV screening is not routine. Women at high risk, such as day care workers and health care providers, should be offered testing with both immunoglobulin G and M (IgG and IgM). Screening may also be indicated as part of the workup for mononucleosis-like symptoms. Presence of CMV IgM is not helpful for timing the onset of infection because it is present in only 75% to 90% of women with acute infection, can remain positive following acute infection, and may represent reactivation or reinfection with a different strain. High anti-CMV IgG avidity suggests that the primary infection occurred more than 6 months in the past, while low avidity suggest the primary infection was more recent.
• Fetal ultrasound may demonstrate microcephaly, ventriculomegaly, intracranial calcifications, oligohydramnios, and intrauterine growth restriction. Amniocentesis
P.148 and cordocentesis for polymerase chain reaction (PCR) DNA testing have also been used to diagnose intrauterine infection.
Management
• There is no effective in utero therapy for CMV. Because it is difficult to predict the severity of sequelae, counseling patients appropriately about pregnancy termination is problematic. Limited studies have suggested a role for hyperimmunoglobulin therapy, while use is limited to a case-by-case base until further research confirm that benefits outweigh risks. Use of antiviral drugs in immunocompetent individuals is not indicated. The majority of infected fetuses do not suffer serious sequelae. The benefits of breast-feeding outweigh the risk of infection transmission by breastfeeding and may be encouraged.
Prevention
• CMV transmission requires close personal contact or contact with contaminated bodily fluids. Preventive measures include transfusing only CMV-negative blood products, safe sex practices, and frequent hand washing.
Varicella Zoster Virus
Epidemiology
• Primary varicella infection is estimated to affect only 1 to 5 of every 10,000 pregnancies. Less than 2% of cases occur in adults, but this group represents 25% of mortality from varicella zoster virus (VZV). Herpes zoster is also uncommon in women of childbearing age.
• The major mode of transmission is respiratory, although direct contact with vesicular or pustular lesions may also result in disease. In the past, nearly all persons were infected before adulthood, 90% before age 14 years. Since the advent of varicella vaccine, most people in the United States have vaccine-induced immunity.
• Varicella outbreaks occur most frequently during the winter and spring. The incubation period is 10 to 21 days. Infectivity is greatest 24 to 48 hours before the onset of rash and lasts 3 to 4 days into the rash.
The virus is rarely isolated after the lesions have crusted over.Clinical Manifestations
• Maternal: The characteristic pruritic rash starts as macules, evolves into papules, and then vesicles. Primary varicella infection tends to be more severe in adults than in children and can be especially severe in pregnancy. A particularly morbid complication of VZV in pregnancy is varicella pneumonia. Maternal mortality with varicella pneumonia may reach 40% in the absence of antiviral therapy (3% to 14% with antiviral therapy). In contrast, herpes zoster infection (reactivation of varicella) is more common in older and immunocompromised patients and poses little risk to the fetus.
• Congenital: Fetal infection with varicella zoster can occur in utero, intrapartum, or postpartum. Intrauterine infection infrequently causes congenital abnormalities including cutaneous scars, limb reduction anomalies, malformed digits, muscle atrophy, growth restriction, cataracts, chorioretinitis, microphthalmia, cortical atrophy, microcephaly, and psychomotor retardation.
• The risk of congenital malformation after fetal exposure to primary maternal varicella before 20 weeks' gestation is estimated to be cause significant infant morbidity and neonatal mortality rates as high as 25%. Sufficient transplacental antibody transfer to confer fetal immunity requires at least 5 days after the onset of the maternal rash. Women who develop chickenpox, especially near term, should be observed. Delay in delivery may offer the fetus the benefit of passive immunity. Neonatal therapy with immunoglobulin is also important when a mother develops signs of chickenpox within 3 days postpartum. Herpes zoster infection during pregnancy is not associated with fetal sequelae due to maternal antibody transfer.
Diagnosis
• Clinical: The diagnosis of acute varicella zoster in the mother usually can be established by the characteristic cutaneous manifestations described as chickenpox. The generalized vesicular rash usually appears on the head and ears and then spreads to the face, trunk, and extremities.
Mucous membrane involvement is common. Vesicles and pustules evolve into crusted lesions, which then heal and may scar. Herpes zoster, or shingles, demonstrates a unilateral vesicular eruption in a dermatomal distribution.• Laboratory: Confirmation of the diagnosis may be obtained by examining scrapings of vesicular lesions that will reveal multinucleated giant cells. For rapid diagnosis, varicella zoster antigen may be demonstrated in exfoliated cells from lesions by immunofluorescent antibody staining.
• Ultrasonography: Detailed ultrasonographic examination is the best means for assessing a fetus for major limb abnormalities or growth disturbances associated with varicella infection. Ultrasound findings in combination with PCR testing of amniotic fluid can estimate the risk of intrauterine infection and the congenital syndrome.
Management
• Varicella exposure during pregnancy: An IgG titer should be obtained within 24 to 48 hours of exposure to a person with noncrusted lesions. The presence of IgG reflects prior immunity, whereas absence of varicella IgG indicates susceptibility.
• Varicella zoster immune globulin (VZIG) may be administered to susceptible women (i.e., women without detectable varicella IgG) within 72 hours of exposure to reduce the severity of maternal infection. VZIG is administered intramuscularly (IM) at a dose of 125 U/10 kg to a maximum of 625 U. Maternal administration of VZIG, however, does not ameliorate or prevent fetal infection.
• Usually, the disease course is similar in pregnant and nonpregnant patients. Supportive care with fluids and analgesics should be administered. In addition, oral acyclovir, when started within 72 hours of symptom onset, has been shown to be associated with faster healing of lesions, shorter fever times, and less progression to pneumonia. It has low rates of teratogenicity, and its use is recommended by the American College of Obstetricians and Gynecologists (ACOG).
• Varicella pneumonia is a medical emergency with significant risk for mortality.
Patients should be admitted to the hospital for treatment with intravenous (IV) acyclovir. Acyclovir administered to pregnant women with varicella pneumonia during the second or third trimester decreases maternal morbidity and mortality. The dosage of acyclovir is 10 to 15 mg/kg IV every 8 hours for 7 days, or 800 mg by mouth (PO) five times per day. Tocolytics are generally avoided in women with varicella pneumonia. Delivery should be performed for obstetric indications.P.150
Prevention
• Preconception counseling plays an important role in prevention of VZV. An attenuated live vaccine was approved by the U.S. Food and Drug Administration (FDA) in 1995. One dose is recommended for all children between ages 1 and 12 years. Two doses, given 4 to 8 weeks apart, are recommended for adolescents and adults without history of varicella infection. The seroconversion rate after vaccination is approximately 82% in adults and 91% for children. Use of the vaccine during pregnancy is not recommended, but it is appropriate for breastfeeding mothers.
Parvovirus B19
Epidemiology
• Parvovirus B19 is a single-stranded DNA virus passed primarily by respiratory secretions. Also known as erythema infectiosum or fifth disease, it commonly occurs in school-aged children. By adulthood, 30% to 60% of women have acquired immunity (IgG) to the virus. Outbreaks usually occur in the midwinter to spring months. Prevalence in pregnancy is approximately 3.3% and is highest among teachers, day care workers, and homemakers.
Clinical Manifestations
• Maternal: Adults may present with typical clinical features: a red, macular rash and facial erythroderma, which gives a characteristic “slapped cheek” appearance. The rash may also cover the trunk and extremities. Infected adults often have acute joint swelling, usually with symmetric involvement of peripheral joints. The arthritis may be severe and chronic. Cases may also present with constitutional symptoms of fever, malaise, myalgia, and headaches. Some adults have a completely asymptomatic infection. Parvovirus B19 preferentially affects rapidly dividing cells and is cytotoxic to erythroid progenitor cells. It may cause aplastic crisis in patients with chronic anemia (e.g., sickle cell disease or thalassemia).
• Congenital: Approximately one third of maternal infections are associated with fetal infection via transplacental transfer of the virus. Infection of fetal red blood cell precursors can result in fetal anemia, which, if severe, leads to nonimmune hydrops fetalis. Hydrops can lead to rapid fetal death or can resolve spontaneously. In cases of mild to moderate hydrops, approximately one third resolves; this number decreases in cases of severe hydrops. The likelihood of severe fetal disease is increased if maternal infection occurs during the first 18 weeks of pregnancy, but the risk of hydrops fetalis persists even when infection occurs in the late third trimester. Fetal IgM production after 18 weeks' gestation probably contributes to the resolution of infection in fetuses who survive. The overall risk of fetal death after maternal infection before 20 weeks is 6% to 11% and after 20 weeks' gestation is Conscientious hand washing and avoiding known infected contacts are advised.
Rubella Virus
Epidemiology
• Despite widespread immunization programs in the United States, the Centers for Disease Control and Prevention (CDC) reports 10% to 20% of adults remain susceptible to rubella. The annual number of reported cases in the United States, however, remains extremely low, with fewer than 10 cases of congenital rubella occurring annually. The disease remains endemic in many areas of the world, and positive rubella antibodies in individuals from these areas can represent active infection.
Clinical Manifestations
The disease is communicable for 1 week before and for 4 days after the onset of the rash, with the most contagious period occurring a few days before the onset of the maculopapular rash. The incubation period ranges from 14 to 21 days. T ransmission results from direct contact with the nasopharyngeal secretions of an infected person.
• Maternal: Rubella usually presents as a maculopapular rash that persists for 3 days; generalized lymphadenopathy (especially postauricular and occipital), which may precede the rash; transient arthritis; malaise; and headache. Rubella typically follows the same mild course in pregnancy and may be asymptomatic. The majority of women with affected infants report no history of a rash during their pregnancies.
P.152
• Congenital: Maternal viremia leads to fetal infection in 25% to 90% of cases. Fetal sequelae are dependent on gestational age, with 90% of first-trimester exposures resulting in clinical signs, 54% at 13 to 14 weeks, and 25% by the end of the second trimester. Congenital rubella syndrome involves multiple organs. The most common manifestations are sensorineural hearing loss, developmental delay, growth retardation, and cardiac and ophthalmic defects.
• As many as one third of asymptomatic exposed infants may develop late manifestations, including diabetes mellitus, thyroid disorders, and precocious puberty. The extended rubella syndrome (progressive panencephalitis and type 1 diabetes mellitus) may develop as late as the second or third decade of life.
Diagnosis
• Infection is confirmed by serology. Specimens should be obtained as soon as possible after exposure, 2 weeks later, and, if necessary, 4 weeks after exposure. Serum specimens from both acute and convalescent phases should be tested; a fourfold or greater increase in titer or seroconversion indicates acute infection. If the patient is IgG-seropositive on the first titer, no risk to the fetus is apparent. Primary rubella confers lifelong immunity. Reinfection with rubella is usually subclinical, rarely associated with viremia, and infrequently results in a congenitally infected infant.
• Prenatal diagnosis is made by identification of rubella-specific IgM antibody in fetal blood samples obtained at 22 weeks' gestation or later. IgM does not cross the placenta, and therefore, its presence indicates fetal infection.
Management
• If a pregnant woman is exposed to rubella, serologic evaluation is recommended. If primary rubella is diagnosed, the mother should be informed about the implications of the infection for the fetus including the high rate of fetal infection and the option for termination discussed. Women electing to continue the pregnancy may be given immune globulin, which may modify clinical rubella in the mother. Immune globulin, however, does not prevent infection or viremia and affords no protection to the fetus.
Prevention
• Pregnant women should undergo rubella serum evaluation as part of routine prenatal care. A clinical history of rubella is unreliable. If the patient is nonimmune, she should receive rubella vaccine after delivery. The rubella vaccine is a live attenuated virus, so it should be avoided in pregnancy due to the theoretic risk of teratogenicity. The CDC maintains a registry to monitor fetal effects of vaccination, and there have been no reported cases of congenital rubella syndrome after vaccination. Nonetheless, the CDC recommends contraception for 28 days after vaccination.
Influenza
Epidemiology
In recent years, the number of cases of influenza has increased in the general population. The pattern of outbreaks is determined by the changing antigenic properties of the virus and their effect on the transmissibility and infectivity of the virus. During pregnancy, physiologic changes make women more likely to become infected with
P.153 influenza and more likely to have severe infection with significant morbidity and mortality.
Clinical Manifestations
• Maternal: Clinical manifestations of influenza in pregnancy are similar to the general population. The symptoms include fever, cough, rhinorrhea, sore throat, myalgia, and headaches. During the pandemics of 1918, 1957, and 2009, pregnant women were noted to have a disproportionate risk of mortality compared to the general population.
• Fetal: There is some evidence that pandemic influenza infection may increase the risk of spontaneous abortion, preterm delivery, and low-birth-weight fetuses. However, this is not well studied.
Management/Prevention
Antiviral therapies have not been well studied but can be used for postexposure chemoprophylaxis and treatment of influenza. Oseltamivir 75 mg daily for 10 days and zanamivir 10 mg daily are currently used. The CDC maintains a website with up-to-date treatment recommendations: http://www.cdc.gov/flu/antivirals/index.htm. Treatment is otherwise supportive with antipyretics and fluids. The CDC and ACOG recommend use of the trivalent inactivated influenza vaccine at any point during pregnancy.
Hepatitis A Virus
Epidemiology
• An estimated 200,000 cases of hepatitis A virus (HAV) infection occur annually in the United States, and HAV affects approximately 1 in 1,000 pregnancies. HAV is transmitted primarily through fecal-oral contamination and typically is not excreted in urine or other bodily fluids. Obstetric patients at highest risk of developing HAV infection are those who have emigrated from or traveled to countries where the virus is endemic (e.g., Southeast Asia, Africa, Central America, Mexico, and the Middle East).
Clinical Manifestations
• Maternal: Symptoms of HAV infection include malaise, fatigue, anorexia, nausea, and abdominal pain, typically right upper quadrant or epigastric. Physical findings include jaundice, upper abdominal tenderness, and hepatomegaly.
• Congenital: Perinatal transmission of HAV has not been documented.
Diagnosis
• A complete travel history suggests the diagnosis in a jaundiced patient. Laboratory studies may reveal transaminitis (elevated alanine aminotransferase [ALT] and aspartate aminotransferase [AST]) and hyperbilirubinemia. Abnormal coagulation studies and hyperammonemia may suggest more significant liver injury. The presence of IgM antibody to HAV confirms the diagnosis. IgG antibody will persist in patients with a history of exposure.
Management
• Individuals with close personal or sexual contact with an affected individual may receive HAV immune globulin in a single IM dose.
P.154
• T reatment of HAV is supportive. There is no antiviral therapy. Activity level should be decreased, and upper abdominal trauma should be avoided. Patients with hepatitis-induced encephalopathy or coagulopathy and debilitated patients should be hospitalized.
Prevention
• The HAV vaccine, an inactivated vaccine, may be used in pregnancy. The vaccine is recommended for individuals traveling to endemic areas and is administered in two injections 4 to 6 months apart.
Hepatitis B Virus
Epidemiology
• In North America, hepatitis B virus (HBV) transmission occurs most commonly via parenteral exposure or sexual contact. Approximately 43,000 persons in the United States are newly diagnosed each year, with an estimated 2.2 million chronic carriers. Acute HBV occurs in 1 to 2 per 1,000 pregnancies and chronic HBV in 5 to 15 per 1,000. Mother-to-child transmission (MTCT) is an important cause of chronic HBV infection worldwide. Transmission can occur prenatally, during delivery, or postpartum and is highest in women who are HBV envelope antigen (HBeAg)-positive. The vertical transmission rate in these women is as high as 90% in the puerperium if prophylaxis is not given to their neonates.
• Natural history: HBV contains three principal antigens: HBV surface antigen (HBsAg), HBV core antigen (HBcAg), and HBeAg. HBsAg is detectable in serum during acute and chronic infection. HBcAg compromises the central nucleocapsid of the virus; it is found only in hepatocytes during active viral replication and is not detected in serum. HBeAg is a secretory product that is processed from the precore protein; it is a marker of active HBV replication and increased infectivity. The presence of HBeAg is usually associated with high levels of HBV DNA in serum and higher rates of HBV transmission. Circulating antibodies against these viral antigens develop in response to infection.
Clinical Manifestations
• Maternal: The clinical manifestations of HBV during pregnancy are similar to those for the nonpregnant patient. HBV infection presents with nonhepatic prodromal symptoms, including rash, arthralgia, myalgia, and occasionally frank arthritis. Jaundice occurs in a minority of patients. In adults, between 95% and 99% of acute infections resolve completely, and the patient develops protective levels of antibody. The remaining 1% to 5% of patients become chronically infected. These patients are clinically asymptomatic and usually have normal liver function tests. They nonetheless have detectable levels of HBsAg. The incidence of cirrhosis in a chronic HBV carrier is 8% to 20% over 5 years. Acute hepatitis B carries a 1 % risk of maternal mortality. Physiologic changes in immunity, metabolism, and hemodynamics during pregnancy may unmask underlying liver disease in otherwise asymptomatic patients.
• Fetal infection: Maternal-fetal transmission can occur at any time during pregnancy but most commonly occurs at the time of delivery. In women who are seropositive for both HBsAg and HBeAg (indicating active replication), the vertical transmission rate approaches 90%. However, in a woman who is HBsAg-positive and anti-HBV surface antibody-positive with an undetectable hepatitis B viral
P.155 load (carrier state), the risk of transmission drops to 10% to 30%. The frequency of vertical transmission is also affected by the timing of maternal infection. When maternal infection occurs in the first trimester, 10% of neonates are seropositive; when it occurs in the third trimester, 80% to 90% of neonates are infected. Whether infection occurs in utero or intrapartum, the presence of HBeAg in the neonates carries an 85% to 90% likelihood of progression to chronic HBV infection and the associated hepatic sequelae. Prophylactic administration of hepatitis B immunoglobulin to infants after birth reduces transmission from 5% to 10%. Fetal malformation, intrauterine growth restriction, spontaneous abortion, or stillbirth is not associated with HBV infection.
Diagnosis
• Diagnosis is confirmed by serology.
• HBsAg appears in the serum 1 to 10 weeks after an acute exposure prior to the onset of clinical symptoms then becomes undetectable after 4 to 6 months in patients who eventually recover. Persistence of HBsAg for >6 months implies chronic infection.
• The disappearance of HBsAg is followed by the appearance of anti-HBs. In most patients, anti-HBs persist for life, conferring long-term immunity.
• HBeAg is detected during active viral replication. The disappearance of HBeAg and the appearance of anti-HBeAg IgG signal a decrease in infectivity. The presence of anti-HBsAg IgG indicates immunity or recovery.
• If a patient is tested during the period in which results for HBsAg are negative, HBV can be identified by the presence of anti-HBsAg IgM.
Management
• Patients with acute hepatitis B infection may require hospitalization and supportive care. The disease is generally self-limited, and symptoms resolve within 1 to 2 weeks. Therapeutic options for HBV include antiviral nucleoside analogues and pegylated interferon. These therapies have the theoretical risk of teratogenicity but have been shown to be safe.
• Current CDC recommendations include universal screening of all pregnant women for HBV at the first prenatal visit. Serum transaminase levels should be measured in seropositive patients to assess active chronic hepatitis.
• Women exposed to HBV should receive passive immunization with HBV immune globulin (HBIG) and receive recombinant HBV vaccine, preferably in the contralateral arm. HBIG is 75% effective in preventing maternal HBV infection.
• HBIG should be administered to the neonate of an infected mother within the first 12 hours of life. HBIG is followed immediately by the standard three-dose HBV immunization series. The combination of HBIG and HBV vaccine prevents vertical transmission in 85% to 90% of cases.
• Invasive intrapartum fetal monitoring (fetal scalp electrodes or fetal scalp blood sampling) should be avoided if maternal infection is known to help minimize vertical transmission risk.
Prevention
• Vaccination for hepatitis B is recommended for all women of reproductive age, preferably during preconception or routine gynecologic care but is also safe to use during pregnancy.
P.156
Hepatitis C Virus
Epidemiology
• T ransmission of the hepatitis C virus (HCV) is similar to that of HBV but occurs via percutaneous blood contamination and rarely through sexual contact. An increased incidence of HCV is noted among IV drug abusers and recipients of blood products. Mass screening of the blood supply for HCV has markedly decreased the risk of HCV infection to (HSV) is responsible for most nongenital herpetic infections and up to 50% of genital lesions. Type 2 HSV is usually recovered from the genital tract. Approximately 1 in 7,500 live-born infants contract HSV perinatally. Whether pregnancy alters the rate of recurrence or frequency of cervical
P.157 shedding of virus is debated. The incidence of asymptomatic shedding in pregnancy is 10% after a first episode and 0.5% after a recurrent episode.
TABLE 11-1 Interpretation of Hepatitis Serology Results
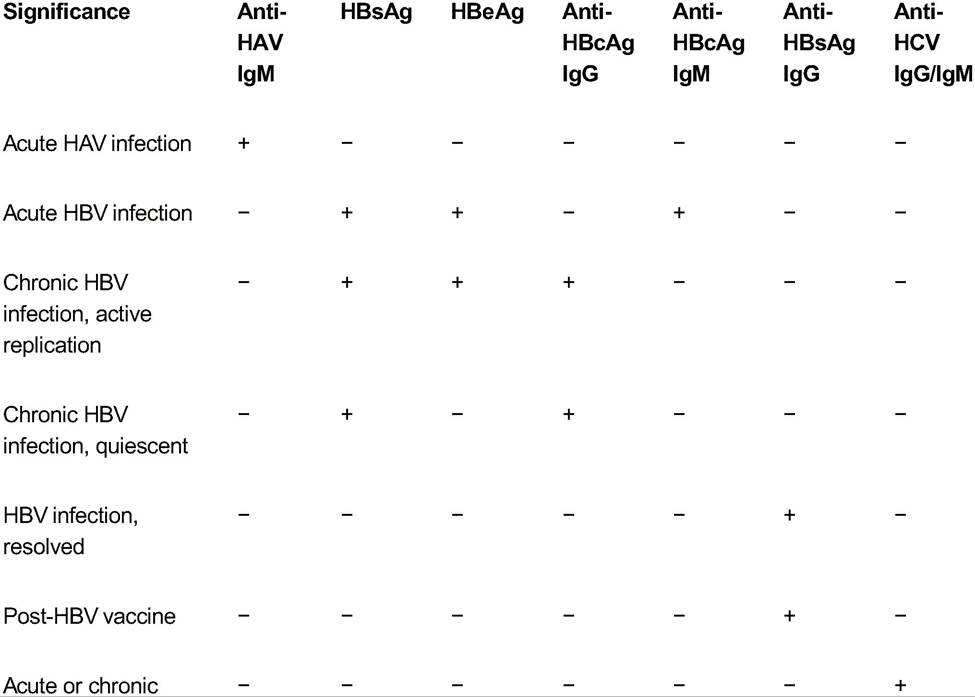
HCV infection
+, present; -, absent; HAV, hepatitis A virus; IgM, immunoglobulin M; HBsAg, hepatitis B surface antigen; HBeAg, hepatitis B envelope antigen; HBcAg, hepatitis B core antigen; IgG, immunoglobulin G; HCV, hepatitis C virus; HBV, hepatitis B virus.
• Primary maternal infection with HSV results from direct contact with mucous membranes or skin infected with the virus, commonly through sexual contact.
• Fetal infection with HSV can occur transplacentally, as an ascending infection from the cervix, or most commonly through direct contact with infectious maternal genital lesions during delivery.
Clinical Manifestations
• Maternal: Primary infections range from mild or asymptomatic to severe. Vesicles appear on the cervix, vagina, or vulva from 2 to 10 days after exposure. Swelling, erythema, pain, and regional lymphadenopathy are common. The lesions persist for 1 to 3 weeks with concomitant viral shedding. Reactivation occurs in 50% of patients within 6 months of the initial outbreak and subsequently at irregular intervals. Symptoms of recurrent outbreaks are generally milder, with viral shedding lasting less than a week. In pregnancy, primary outbreaks are not associated with spontaneous abortion but may increase the incidence of preterm labor in the latter half of pregnancy.
P.158
• Fetal infection is usually the result of primary maternal infection. T ransmission from a recurrent maternal infection is rare, accounting for If amniotic fluid PCR results for Toxoplasma are negative, spiramycin is used as a single agent; if results are positive, pyrimethamine and sulfadiazine should be added. Spiramycin dosing is 500 mg PO five times daily, or 3 g/day in divided doses.
• Pyrimethamine and sulfadiazine: Patients with documented Tgondii infection of the fetus may be offered treatment with pyrimethamine 25 mg PO daily and sulfadiazine PO 1 g four times daily for 28 days. Folinic acid, 6 mg IM or PO, is administered three times per week to prevent toxicity. During the first trimester, pyrimethamine is not recommended due to teratogenic risk. Sulfadiazine is omitted from the regimen at term.
Prevention
• Pregnant women should eat only fully cooked meats, wash their hands after preparing meat for cooking, wash fruits and vegetables well, and avoid contact with cat litter boxes.
BACTERIA
Group B Streptococcus
Epidemiology
• Group B Streptococcus (GBS) (Streptococcus agalactiae), a Gram-positive bacteria, can be isolated from the vagina and/or rectum in 5% to 40% of pregnant women in the United States. Neonatal colonization may occur as a result of ascending infection from the maternal genital tract or during passage of the fetus through the birth canal during a vaginal delivery. The vertical transmission rate may be as high as 72%, but invasive disease in term neonates is rare. In preterm infants, however, invasive disease is more common and is accompanied by significant morbidity and mortality.
Clinical Manifestations
• Maternal: GBS is a common urinary pathogen in pregnant women. GBS is isolated in 5% to 29% of cases of asymptomatic bacteriuria and in 1 % to 5% of cases of acute cystitis during pregnancy. When inadequately treated, both asymptomatic bacteriuria and acute cystitis can progress to pyelonephritis, necessitating hospitalization. Maternal GBS infection has also been associated with premature rupture of membranes, preterm labor, chorioamnionitis, bacteremia, puerperal endometritis, and postoperative wound infections after cesarean section.
• Congenital: Neonatal colonization with GBS results from contamination from the mother's genital tract in 75% of cases. One percent to 2% of colonized infants will develop early-onset GBS infection (infection occurring within the first 7 days of life), with a case fatality of 11 % to 50%. Preterm and/or low-birth-weight
P.161 infants are at higher risk than term neonates. Maternal risk factors that predispose a neonate to early-onset GBS infection include preterm delivery, prolonged rupture of membranes (>18 hours), intrapartum temperature of at least 38°C or 100.4°F, or a prior infant who had GBS infection.
• Late-onset GBS infection, which occurs 7 days or more after birth, affects 0.5 to 1.8 per 1,000 live births. It may result from maternal-neonatal transmission, nosocomial, or community contacts. Mortality for late-onset disease is approximately 10%.
• Meningitis occurs in 85% of all colonized neonates, but infants may also present with bacteremia without localizing symptoms. Other clinical syndromes include pneumonia, osteomyelitis, cellulitis, and sepsis. Neurologic sequelae develop in 15% to 30% of meningitis survivors.
Diagnosis
• GBS colonization can be detected by culture or rapid DNA-based testing. Anorectovaginal culture remains the gold standard and can be performed in a single swab of the areas. Samples must be inoculated immediately into Todd-Hewitt broth or onto selective blood agar to inhibit the growth of competing organisms. The predominant limitation of culture is time. Results are not available for 24 to 48 hours, making management difficult if delivery is imminent. Rapid diagnostic tests are available that detect specific polysaccharide antigens. They are easy to perform, generally less expensive than a culture, and produce results within a short period of time (usually 1 hour). The tests are highly sensitive in patients who are heavily colonized with GBS; however, their lower sensitivity and higher false-negative rate compared with those of cultures prevent their widespread clinical application in obstetrics. Rapid DNA-based testing is also available with excellent sensitivity.
Management
• Treatment of uncomplicated GBS lower urinary tract infection is with amoxicillin or penicillin. Hospitalization is required for cases of pyelonephritis, and patients should be treated with an appropriate regimen until afebrile and asymptomatic for 24 to 48 hours. She may then be discharged to complete a total of 10 days of antibiotics.
• ACOG recommends universal screening for GBS at 35 to 37 weeks' gestation with a swab of the lower vagina and rectum. Women with a positive screen, a previous infant with GBS infection, urine colonization (>10,000 colony-forming units (CFUs)ZmL) or infection with GBS during the current pregnancy, labor before 37 weeks with unknown GBS status, rupture of membranes >18 hours at term with unknown GBS status, or signs of chorioamnionitis should receive intrapartum antibiotics. T reatment is typically with penicillin 5-million-U IV loading dose followed by 2.5 million U IV every 4 hours. Prophylaxis is most effective if started at least 4 hours before delivery. For patients with a penicillin allergy, cephalosporins can be used if the allergy is mild as with a rash but should be avoided for more severe allergies that may lead to anaphylaxis. Genital culture results should be evaluated for sensitivity to clindamycin and erythromycin, where resistance to either precludes effectiveness of clindamycin. If culture results demonstrate resistance or sensitivities are unknown and the patient has a severe penicillin allergy, vancomycin should be administered.
SEQUELAE OF PERINATAL INFECTIONS
Table 11-3 summarizes the sequelae of the perinatal infections discussed earlier.
P.162 P.163
TABLE 11-3 Maternal and Fetal Manifestations of Perinatal Infections
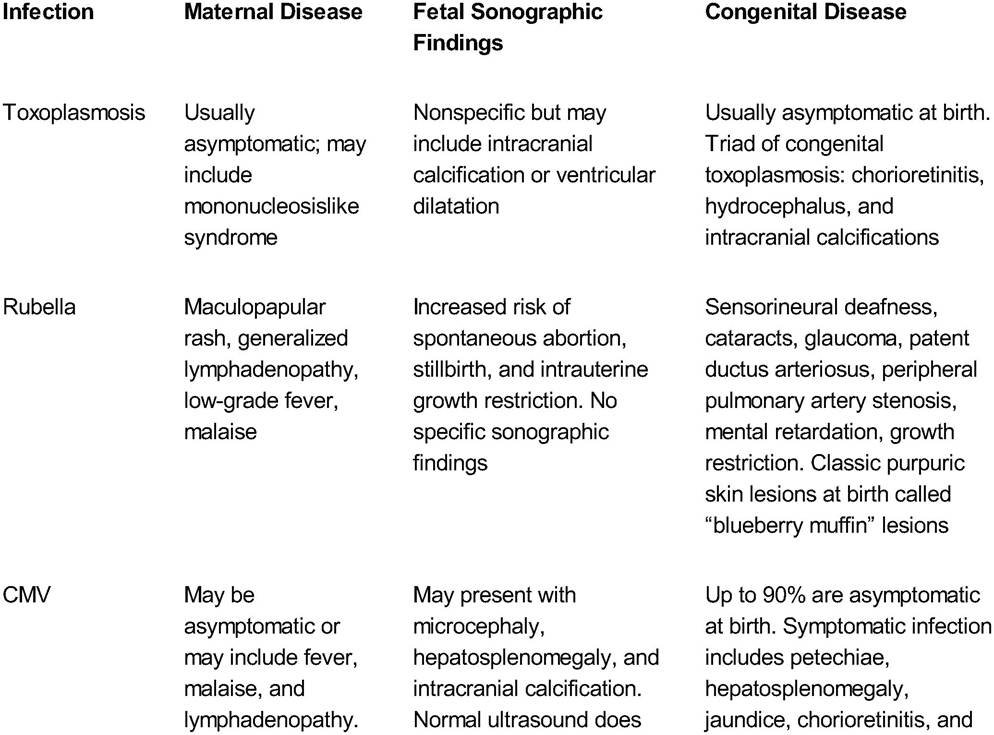
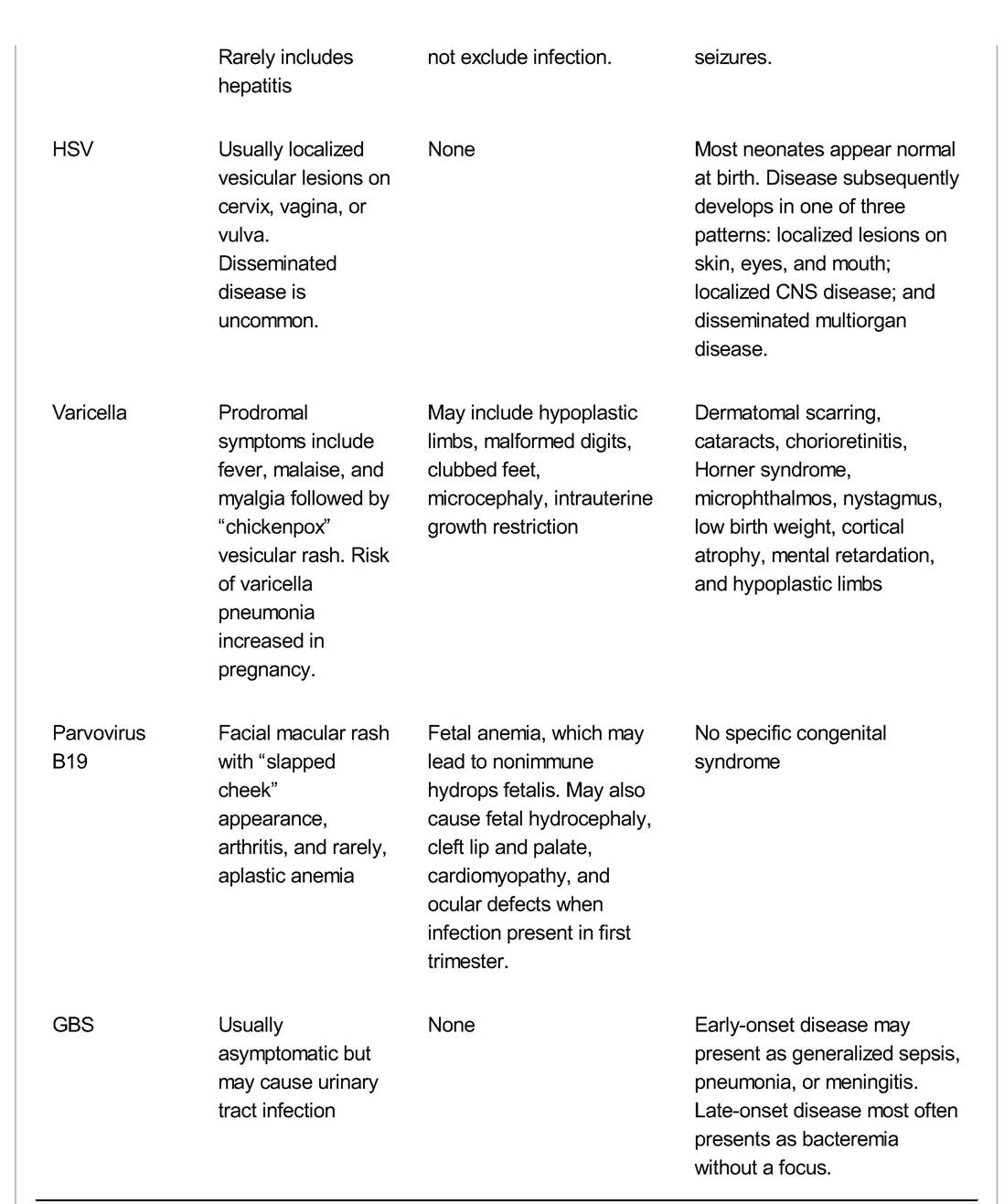
CMV, cytomegalovirus; HSV, herpes simplex virus; CNS, central nervous system; GBS, group B Streptococcus
SUGGESTED READINGS
American College of Obstetricians and Gynecologists. ACOG practice bulletin. Perinatal viral and parasitic infections. Number 20, September 2000. (Replaces educational bulletin number 177, February 1993). Int J
Gynaecol Obstet 2002;76(1 ):95-107.
Centers for Disease Control and Prevention. Perinatal group B streptococcal disease after universal screening recommendations—United States, 2003-2005. MMWR Morb Mortal Wkly Rep 2007;56(28):701- 705.
Corey L, Wald A. Maternal and neonatal herpes simplex virus infections. N Engl J Med 2009;361(14):1376- 1385.
Lin K, Vickery J. Screening for hepatitis B virus infection in pregnant women: evidence for the U.S.
Preventive Services Task Force reaffirmation recommendation statement. Ann Intern Med 2009;150(12):874- 876.
Malm G, Engman ML. Congenital cytomegalovirus infections. Semin Fetal Neonatal Med 2007; 12(3):154- 159.
Sharma D, Spearman P. The impact of cesarean delivery on transmission of infectious agents to the neonate. Clin Perinatol 2008;35(2):407-420.
Winn HN. Group B streptococcus infection in pregnancy. Clin Perinatol 2007;34(3):387-392.