Prepregnancy counselling
The major cardiac causes of maternal mortality and morbidity
Congenital cardiovascular malformation is the single commonest group of congenital abnormalities seen in newborn children, occurring about 0.8-1% (7).
Before the introduction of open heart surgery in the 1960s (requiring the development of heart-lung bypass technology, and the use of hypothermia), about two-thirds of affected babies died in the first year of life (8). Accordingly, the majority of women with cardiac disease becoming pregnant before the 1960s had acquired disorders, mostly secondary to rheumatic fever. Mitral stenosis (caused by autoimmune damage to the valve associated with the immune response to rheumatic fever caused by streptococcal infections) was the commonest lesion, and in 1957 the maternal mortality due to acquired heart disease was approximately 5 per 100,000 maternities. However the widespread use of penicillin greatly reduced the incidence of rheumatic fever, and by 1990 the maternal mortality rate due to acquired disease had fallen to only 0.38 per 100,000 maternities. In contrast, by the 1990s two- thirds of women with congenital heart disease were surviving into their 20s and were therefore eligible to become parents themselves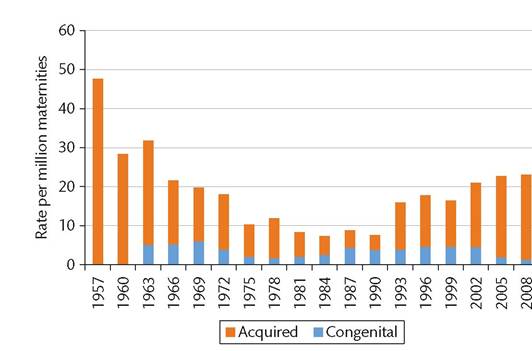
Figure 12.1 Cardiac deaths 1957-2008.
Source data from Cantwell R, Clutton-Brock T, Cooper G, Dawson A, Drife J, Garrod D et al. Saving Mothers' Lives: Reviewing maternal deaths to make motherhood safer: 2006-2008. The Eighth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG 2011; 118 Suppl 1:1-203.
(8); and they now accounted for half of maternal deaths due to cardiac disease (also 0.38 per 100,000 maternities). However, since that time, in the United Kingdom, the rate of death due to acquired heart disease has increased again—it has almost trebled, to 2.18 per 100,000 maternities in 2008, while those due to congenital heart disease had fallen to 0.13 per 100,000 maternities (Figure 12.1) (9).
The United Kingdom Confidential Enquiries into Maternal Deaths and Morbidity report for the triennium 2009-2011 confirmed the fact that cardiac disease now represents the single most common cause of maternal death related to pregnancy (10) (Figure 12.2). What lies behind this worrying increase?Currently, one-third of maternal deaths from cardiac disease are the result of myocardial infarction/ischaemic heart disease. This is in part due to the growing number of women having babies later in life. Figure 12.3 illustrates the changing age distribution of maternal age in the United Kingdom from 1938 through 2013. The most striking feature is a more than halving of births to women under the age of 25 since the early 1970s, paralleled by a more than fourfold increase in
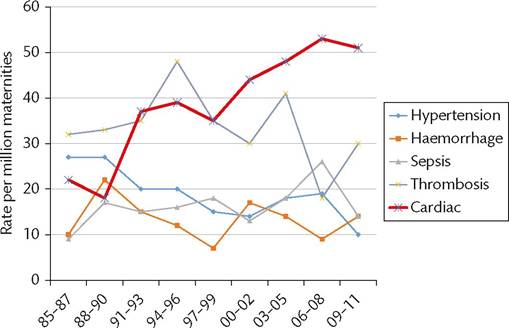
Figure 12.2 Number of deaths by cause by year.
Source data from MBRRACE-UK. Saving lives, Improving Mother's Care. https:// www.npeu.ox.ac.uk/downloads/files/mbrrace-uk/reports/Saving%20Lives%20 Improving%20Mothers%20Care%20report%202014%20Full.pdf.
A further third of deaths are associated with cardiomyopathy. This comprises a variety of conditions, the commonest being hypertrophic cardiomyopathy and the specific pregnancy-related condition of peripartum cardiomyopathy, as well as less common conditions such as restrictive cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy, and left ventricular non-compaction. The overall prevalence of dilated cardiomyopathy is difficult to define because many affected individuals are apparently healthy; about a third of cases are familial (12). The common feature in all cases is left ventricular dilatation and systolic dysfunction in the absence of any obvious cause such as hypertension. The aetiology of peripartum cardiomyopathy remains conjectural, but may include genetic susceptibility, viral myocarditis, immunologically mediated damage, and the antiangiogenic 16 kDa fragment of the hormone prolactin (13).
Rheumatic heart disease, congenital heart disease, and pulmonary hypertension are currently each responsible for about 510% of deaths.
Implications for the baby
Fetal growth is very dependent upon efficient placental perfusion and gas and nutrient exchange. This in turn is determined partly by maternal cardiac output (affecting the maternal blood supply to the placenta), the structure and function of the placenta itself (including the microvasculature), and the efficiency of the fetal circulation. In women with heart disease, even when apparently normal cardiac output is maintained, there is a tendency for babies to be smaller than average (Figure 12.4). The reasons for this are not clear, but might in some cases be associated with reduced maternal stature, impaired nutrition, or genetic effects. Easier to understand is a greater reduction in mean centile birthweight when there is reduced cardiac output. Beta-blockers are commonly used in women with cardiac disease who have a tendency to arrhythmia (myocardial excitability is increased by the hormonal changes of pregnancy) and these are known to cause (usually mild) fetal growth restriction (14). However, the most serious forms of growth restriction are associated with maternal cyanosis, due not only to the lower oxygen tension in the blood, but also to the compensatory maternal high haemoglobin concentrations, which increase blood viscosity and impair placental blood flow. In such cases, moderate to severe fetal growth restriction almost always occurs, commonly requiring early delivery even if the mother's condition remained stable.
The priorities in prepregnancy counselling
The number one priority in prepregnancy counselling is to make sure that the mother and her family are fully and correctly informed of the risks facing both the mother and the baby in any future pregnancy. At one time it was traditional to separate cardiac conditions into three categories: mild, moderate, or severe.
Mild lesions are those where the maternal risk of mortality is less than 1%, and this will include such common conditions as mitral valve prolapse or a well-functioning bicuspid aortic valve. However, it must be remembered that even a risk of death of 1 in 1000 is still more than 10 times higher than the background risk for a healthy woman in a developed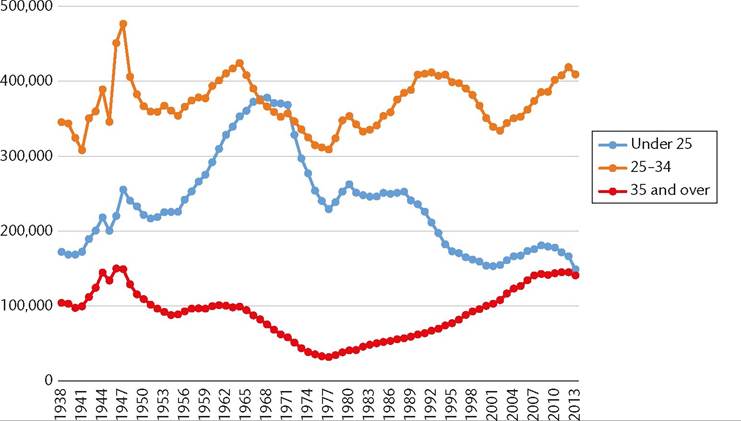
Figure 12.3 Births per year by maternal age group in the United Kingdom.
Source data from http://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/livebirths/bulletins/livebirthsinenglandandwalesbycharacteristicsofmother1/ 2014-10-16.
country, so one must be careful to explain that ‘low risk' does not mean ‘no risk. A moderate-risk lesion is one where the risk of maternal mortality or morbidity is between 1% and 10%, and includes significant mitral or aortic stenosis, women with a systemic right ventricle, cyanotic lesions without pulmonary hypertension, or a Fontan type circulation (a single systemic ventricle where the blood returning from the body travels to the lungs via direct blood vessel connections without a pumping chamber). Some women faced with up to a one in ten chance of dying in pregnancy will choose to remain childless. It must also be appreciated that some of these conditions confer a particularly high risk of growth restriction, particularly, for example, in women with a Fontan circulation, where in one series the mean birthweight was just over 2 kg (15).
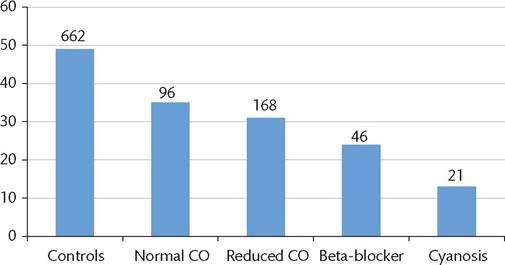
Figure 12.4 Centile birthweight by cardiac lesion group. CO, cardiac output.
Source data from Gelson E, Curry R, Gatzoulis MA, Swan L, Lupton M, Steer P, Johnson M. The effect of maternal heart disease on fetal growth. Obstet Gynecol 2011, Apr;117(4):886-91.
It has been traditional in the past for women with a risk of mortality exceeding 10% (such as women with Eisenmenger syndrome, truncus arteriosus syndrome, pulmonary hypertension, or Marfan syndrome with an aortic root dilated to more than 4 cm) to be advised against pregnancy.
However, the principle of patient autonomy has now superseded the traditional paternalistic model of healthcare, and shared decision-making has become the new standard of practice (16). The perception of risk is subjective and varies from one person to another. Sometimes women, their partners, and family will not consider having children to be a major priority and instead value longevity for the woman. On the other hand, some women feel that their lives are incomplete without having children, and will be prepared to take even high risks to achieve motherhood. In this regard, it is vital that women understand that there may also be a risk to their baby, both of the recurrence of their heart disease if it is congenital, and fetal growth restriction and/or preterm birth.It is the clinician’s responsibility to ensure that all decisions are taken in full knowledge of the facts. Sometimes these facts are unwelcome, for example, one might have to tell a woman who has not previously thought much about it, that her life expectancy is reduced. Even if she survives her pregnancy, she might face the prospect of needing major surgical intervention or even dying while her children are young. While it might seem harsh to have to confront her with these unwelcome facts, a 2015 United Kingdom Supreme Court judgment in the case of Nadine Montgomery ruled that women should be given full information and stated that ‘the onus should not be upon the patient (to ask), who may not know that there is anything to ask about’ (17, 18). Counselling should be done jointly by an obstetrician and a cardiologist, and risks should be discussed in a sensitive manner, aiming to inform but not frighten unnecessarily. It is also important to say that risk assessment can never be precise. A 10% risk of dying is a population statistic; for the one woman in ten who dies the outcome is 100% mortality. In terms of whether the decision is contraception or a pregnancy, only women themselves can decide because only they have the full insight into their own priorities. Preconception counselling should not be aimed at discouraging women from becoming pregnant; rather, it should empower them to make informed choices.