Prevention of Preterm Birth in Multiple Pregnancies
Abdallah Adra
Introduction
Twin pregnancies are associated with an increased risk of perinatal morbidity and mortality, primarily due to spontaneous preterm deliveries. A number of strategies regarding secondary prevention of preterm birth (PTB) have been proposed, including oral tocolytics, bed rest, hospitalisation, home uterine activity monitoring, use of progesterone, cerclage and, most recently, cervical pessary.
There is much heterogeneity among health care providers when it comes to obstetric care of twin gestations,1 and although twins have been well represented in many studies of PTB, these studies have failed to identify adequate predictive tests (short cervical length established more than two decades ago remains the single best predictor) and to establish effective interventions.2Our current armamentarium to prevent PTB is limited, particularly in multiple gestations. The objective of this chapter is to review the evidence and efficacy of the different interventions used in contemporary obstetric practice to reduce PTB in multiple pregnancy. Given the paucity of literature for triplet and higher-order pregnancies, the chapter concentrates mainly on twin pregnancy.
Routine Hospitalisation and Bed Rest
Bed rest with or without hospitalisation has been commonly recommended to women with multifetal gestations. However, a Cochrane review demonstrated no benefit from routine hospitalisation or bed rest for women with an uncomplicated twin pregnancy. No reduction in the risk of preterm birth or perinatal death was evident, although there is a suggestion that fetal growth may be improved.3 Until further evidence is available, bed rest with or without hospitalisation in women with multiple pregnancies is not recommended because of the lack of benefit and the risk of thrombosis and deconditioning associated with prolonged bed rest.
Prophylactic Tocolytics
Based on available evidence, there is no role for the prophylactic use of any tocolytic agent in women with multifetal gestations, including the prolonged use of betamimetics for this indication. The use of tocolytics to inhibit preterm labour in multifetal gestations has been associated with a greater risk of maternal complications such as pulmonary oedema. The administration of oral betamimetics specifically did not reduce the incidence of preterm birth, low-birthweight newborns or neonatal mortality in women with multifetal gestations when compared with placebo, and it has been associated with increased maternal and fetal cardiac stress and gestational diabetes mellitus.4
Cervical Cerclage
While widely accepted in singleton pregnancies, the use of cervical cerclage has been a source of great controversy in twin pregnancies. There are four clinical scenarios where cervical cerclage has been used for the argument of preventing or reducing PTB in multiple gestations: multiples-only indication, history-indicated, ultrasound-indicated and physical-exam indicated cerclage (or rescue cerclage).
Many obstetricians are hesitant to offer cerclage in women with twins regardless of sonographic or physical exam findings, in accordance with several current practice guidelines recommending against cerclage in multiple gestations, largely based on meta-analyses demonstrating lack of benefit in reducing PTB and improving neonatal outcomes, and even a potential harm with cerclage in twins. However, these meta-analyses should be interpreted with caution, as data were obtained from small trials with varying selection criteria and management protocols for mostly history-indicated and ultrasound-indicated cerclage in twins.
Multiples-Only-Indicated Cerclage
Studies suggest no benefit and a possible detrimental effect of elective cerclage performed at the end of the first trimester routinely in twin pregnancy without a known history of cervical insufficiency.
One of the earliest studies assessing the efficiency of elective cerclage in preventing PTB and reducing neonatal mortality followed a group of 50 twin pregnancies occurring after ovulation induction, half of which were non-randomly selected to undergo elective cerclage. The rate of PTB and neonatal mortality was not significantly different between the study and the control group managed expectantly. Hence, the use of prophylactic cerclage to reduce spontaneous PTB for the sole indication of twin pregnancy has not been shown to be beneficial and is not recommended.5History-Indicated Cerclage
History-indicated cervical cerclage is performed early in pregnancy based on poor obstetric or gynaecologic history. However, the targeted population in which history-indicated cerclage is recommended and most likely to be beneficial has still not been well established based on different professional society guidelines. Moreover, these guidelines pertain to women with a current singleton pregnancy whereas no recommendations exist regarding history-indicated cerclage in twin pregnancy owing to a lack of relevant data.
A recent small retrospective case-control study looked at 41 women with a twin pregnancy who had undergone a first-trimester history-indicated cerclage during an 11-year period at a single centre, comparing them to a control group of 41 women who were managed expectantly. Gestational age at delivery was higher in the cerclage group than in those managed expectantly (median 35 vs 30 weeks; P < 0.0001). Rates of spontaneous PTB before 24, 28, 32 and 34 weeks were significantly lower in the cerclage group than in the control group. Median birthweight was higher in the cerclage group, with lower rates of low birthweight (< 2,500 g) and very low birthweight (< 1,500 g) than in the group managed expectantly. Rates were also lower in the cerclage group for stillbirth, admission to the neonatal intensive care unit and composite adverse neonatal outcome.6 In contrast, other retrospective cohort studies of history indicated cerclage have not shown efficacy suggesting the need for adequate randomised trials on cerclage placement in this subset of women.
Ultrasound-Indicated Cerclage
A Cochrane review found that when performed in twin pregnancies, ultrasound-indicated cervical cerclage was correlated with an increased incidence of adverse perinatal outcomes including higher rates of perinatal death, low birthweight and respiratory distress syndrome, and it had no benefit in terms of the prevention of PTB.7 This has led to the SMFM recommendations in the ‘Choosing Wisely' programme advocating against the use of cerclage in twin pregnancy with a short cervix owing to the lack of appropriate studies. Of note, the five trials included in the Cochrane review did not study twin pregnancy exclusively (i.e. they included singleton pregnancies), and in fact ultrasound-indicated cerclage in twins has not been studied in a dedicated randomised controlled trial.
Two retrospective cohort studies compared the perinatal outcomes in 222 twin pregnancies with short cervical length (CL ≤ 25 mm at 16-24 weeks) and who were managed with either ultrasound-indicated cerclage (n = 100) or no cerclage (n = 122). After adjusting for gestational age on presentation, there were no differences in the rate of PTB at 28,32 and 35 weeks between the two groups. However, in the pre-planned subgroup analysis of twin pregnancies with CL ≤ 15 mm before 24 weeks, cerclage placement was associated with a significant prolongation of pregnancy by almost four more weeks, significantly decreased spontaneous PTB at less than 34 weeks by 49% and admission to the neonatal intensive care unit by 58% compared to controls.8,9
These two retrospective cohort studies provide evidence that the use of cervical cerclage in twin gestations with short cervix, mostly in those with CL ≤ 15 mm, can potentially reduce the risk of spontaneous PTB at less than 34 weeks of gestation. Ultimately, the results require confirmation in randomised controlled trials.
Physical Examination-Indicated Cerclage (PEIC)ZRescue Cerclage
The first and only randomised controlled trial evaluating physical examination-indicated cerclage (PEIC) in twins was recently published.
It was a multicentre (eight centres) randomised controlled trial of women with twin pregnancy and asymptomatic cervical dilatation from 1-5 cm between 16 to 23 6/7 weeks. The primary outcome was the incidence of PTB < 34 weeks. The Data Safety Monitoring Board recommended stopping the trial due to significant decrease of perinatal mortality in the cerclage group. Thirteen women were eventually enrolled in each group (cerclage versus no cerclage). The mean gestational age at delivery was 29.1 weeks (cerclage group) versus 22.5 weeks (no cerclage) (p < 0.01). Perinatal mortality was also significantly reduced in the cerclage group. The authors concluded that, despite the small sample size as the enrolment did not reach the intended 52 cases, they were able to show a significant benefit to physical exam indicated cerclage in twin gestation.10Based on this trial and findings of other retrospective cohort studies and case series that have reported on outcomes of mid-trimester emergency cerclage in twin pregnancies, it seems reasonable to conclude that PEIC/rescue cerclage may prolong gestation, reduce PTB at less than 34 weeks and lower neonatal morbidity and mortality.
Results of Meta-analysis/Systematic Review
A recent systematic review and meta-analysis eloquently summarises these findings. It included a total of 16 randomised controlled trials and cohort studies with 1,211 women, comparing the efficacy of cerclage with no cerclage for women with twin pregnancies.11 Outcomes indicated that cerclage placement for twin pregnancies with a cervical length of < 15 mm was associated
with significant prolongation of pregnancy by a mean difference of 3.89 weeks of gestation and a reduction of PTB at less than 37, 34 and 32 weeks of gestation, compared with those pregnancies in the control group. For women with a dilated cervix of > 10 mm, cerclage placement was associated with significant prolongation of pregnancy by a mean difference of 6.78 weeks of gestation; a reduction of PTB at less than 34, 32,28 and 24 weeks of gestation and improvement of perinatal outcomes compared with those in the control group.
However, for twin pregnancies with a normal cervical length (cerclage for an indication for women with a history of PTB or twin alone), the efficacy of cerclage placement was less certain because of the limited data.Management Options
The use of cervical cerclage for PTB in twin pregnancy is somewhat limited to the following scenarios:
• When the cervix is dilated 1-4 cm at 16-24 weeks of gestation (physical examination indicated, rescue or emergency cerclage).
• In asymptomatic women without cervical dilatation before 24 weeks but with a short cervix detected incidentally by transvaginal ultrasound (TVUS) and only when ≤ 15 mm in length (ultrasound-indicated cerclage).
Cervical Pessaries
A cervical pessary is a silicone ring with a small diameter to be fitted around the cervix and a larger diameter to fix the device against the pelvic floor. This effectively rotates the cervix toward the posterior vaginal wall and corrects the cervical angle.
The unequivocal benefits of using the cervical pessary in the prevention of PTB in twin pregnancies have not been established. The results of different clinical trials are not only contradictory, but two of the most recent meta-analyses have yielded conflicting conclusions.
Two randomised clinical trials published in the year 2016 yielded conflicting results.12,13 The first was a multicentre (10 centres, eight countries), randomised clinical trial in unselected twin pregnancies of cervical pessary placement from 20 to 24 weeks of gestation until elective removal or delivery versus expectant management. A total of 1,180 (56.0%) of the 2,107 eligible women agreed to take part in the trial; 590 received cervical pessary and 590 had expectant management. There were no significant differences between the pessary and control groups in rates of spontaneous birth < 34 weeks (primary outcome), perinatal death, adverse neonatal outcome or neonatal therapy. A post hoc subgroup analysis of 214 women with short cervix (≤ 25 mm) also showed no benefit from the insertion of a cervical pessary.12
The second was a prospective, open-label, multicentre, randomised clinical trial conducted in five hospitals in Spain (PECEP-Twins). The objective was to test whether a cervical pessary reduces PTB in twin pregnancies with a sonographic short cervix. Cervical length was measured in 2,287 women; 137 pregnant women with a sonographic cervical length ≤ 25 mm were randomly assigned to receive a cervical pessary or expectant management. Spontaneous PTB < 34 weeks of gestation (primary outcome) was significantly less frequent in the pessary group than in the expectant management group. Pessary use was associated with a significant reduction in the rate of birthweight < 2,500 grams. No significant differences were observed in composite neonatal morbidity outcome or neonatal mortality (none) between the groups. No serious adverse effects associated with the use of a cervical pessary were observed.13
More recently the STOPPIT2 trial was published. In the STOPPIT 2 open label multicentre randomised controlled trial (57 centres), 503 twin pregnancies with cervical length at 22 hospitals in Europe and involving 1,169 women with unselected twin pregnancies revealed that universal early administration of vaginal progesterone at a dose of 600 mg per day from 11 to 14 weeks of gestation, as compared to placebo, did not reduce the incidence of spontaneous birth between 24 and 34 weeks of gestation. Post hoc time to event analysis led to the suggestion that progesterone may reduce the risk of spontaneous birth < 32 weeks in women with cervical length < 30 mm and it may increase the risk for those with cervical length ≥ 30 mm.18
Twins with Short Cervix
17-alpha-hydroxyprogesterone caproate (17-OHPC)
Two trials studied the use of 17-OHPC in reducing the risk of PTB in twin gestations with a short cervix identified by a transvaginal ultrasound examination in the second half of the pregnancy.
A secondary analysis of a double-blind, placebo-controlled randomised controlled trial of 221 women categorised by cervical length (CL) and randomised to receive 250 mg 17-OHPC IM weekly injections versus placebo showed no reduction in the rate of PTB before 35 weeks, neither in women with CL 25th centile (64.3% vs 45.8%, P = 0.18) nor in those with CL > 75th centile (38.1% vs 35.5%, P = 0.85).19
A randomised controlled trial of 165 women, conducted in France and involving asymptomatic women with twin gestation between 24 and 31 (6/7) weeks with CL ≤ 25 mm by TVUS, who were randomised to receive either placebo or 500 mg IM injections of 17-OHPC, repeated twice weekly until 36 weeks or delivery found there was no significant difference in median time to delivery (45 vs 51 days) and treatment with 17-OHPC was associated with a significant increase in rate of preterm delivery before 32 weeks.20
Vaginal micronised progesterone
Two randomised controlled trials have evaluated the effectiveness of vaginal micronised progesterone in reducing the risk of preterm birth in twin gestations with a short cervix identified by a transvaginal ultrasound examination.
A PREDICT trial secondary analysis of a sub-population of high-risk twin pregnancies, including those with CL ≤ 10th centile at 20-24 weeks' gestation, history of spontaneous preterm delivery before 34 weeks and miscarriage after 12 weeks found no significant difference in the mean gestational age at delivery between the progesterone and placebo group either in patients with a short cervix or in those with a history of PTD or late miscarriage. Similarly, there were no significant differences between the treatment groups in maternal or neonatal complications and mean ASQ score at 6 and 18 months of age.21
A randomised controlled trial in asymptomatic women with twins and a CL 20-25 mm at 20-24 weeks (250 women included; 77% had short cervix out of 322 women with dichorionic twin pregnancy!) found a significant reduction in PTB < 34 weeks and in both neonatal morbidity and early neonatal death.22
Individual Participant Data Meta-analyses of Progesterone for Prevention of Preterm Birth in Twin Gestations The first individual participant data meta-analysis published in 2015 involved 13 trials including 3,768 women with twin pregnancy and 7,536 babies. Neither 17-OHPC IM nor vaginal micronised progesterone reduced the incidence of adverse perinatal outcome in unselected women with an uncomplicated twin gestation. In a subgroup of women with a cervical length (CL) ≤ 25 mm, vaginal progesterone reduced adverse perinatal outcome when cervical length was measured at randomisation or before 24 weeks of gestation. The authors concluded that vaginal progesterone may be effective in reducing PTB and neonatal morbidity in women with CL of ≤ 25 mm, but further research is warranted to confirm this finding.16
The second updated meta-analysis of individual patient data, of vaginal progesterone for the secondary prevention of SPTB in women with a twin gestation and a short cervix published in 2017, included six trials. It involved 303 women and 606 infants; 144 women received no treatment or placebo and 159 women received vaginal progesterone. Vaginal progesterone reduced PTB at < 33 weeks (43% in placebo group vs 31% in progesterone group, p = 0.01). Vaginal progesterone significantly reduced respiratory distress syndrome by 30% (RR = 0.7; 95% CI:0.56-0.89), birthweight < 1,500 grams by 47% (RR = 0.53; 95% CI: 0.35-0.80), mechanical ventilation by 46% (RR = 0.54; 95% CI: 0.36-0.81), neonatal death by 47% (RR = 0.53; 95% CI: 0.35-0.81). In a subgroup analysis, it was found that the reduction in the rate of PTB at less than 33 weeks and in neonatal mortality was similar, irrespective of degree of cervical shortening, dose of progesterone and prior history of SPTB.23
Management Options
For unselected twin gestations, based on the literature reviewed, progesterone treatment, whether weekly intra-muscular injections of 17-OHPC or vaginal micronised progesterone, does not reduce the incidence of SPTB and therefore is not recommended.24
For twin gestations with short cervix (< 25 mm) diagnosed at < 24 weeks gestation, it is also fair to conclude that the preventive administration of 17-OHPC has shown no benefits for prolonging pregnancy or reducing perinatal risk. It is thus not recommended in this context. The daily administration of vaginal progesterone may, however, be effective in reducing perinatal risk in women with short cervix (< 25 mm), but results remain conflicting and most international guidelines are still not recommending this intervention outright.24,25
Prevention of Spontaneous Preterm Labour and Birth in Triplets and Higher-Order Pregnancy
The evidence base for interventions to reduce spontaneous preterm labour and birth in triplets and higher-order pregnancy is poor. There are no established proven effective interventions. Given the conflicting evidence for twin gestations, it is reasonable to assume that the few potential preventative interventions for twins are likely to be less effective in triplets and higher-order multiple pregnancy.
Key Points (See Table 20.1)
• The most common cause of perinatal morbidity and mortality in multiple pregnancy is spontaneous preterm labour and delivery.
• Routine bed rest with or without hospitalisation and oral tocolytics have not been shown to be effective in prevention of SPTB in multiple pregnancy.
• Cervical cerclage for the sole indication of multiple pregnancy or if there is a previous history of spontaneous preterm delivery and/or mid-trimester loss has not been shown to be effective.
• Physical examination indicated or rescue cerclage when the cervix is dilated between
1 cm and 4 cm at 16-24 weeks of gestation has some merit in reducing adverse outcomes and can be considered.
• Ultrasound-indicated cerclage when the cervix is ≤ 15 mm and not dilated on transvaginal ultrasound before 24 weeks of gestation in asymptomatic women may reduce PTB and improve neonatal outcomes.
• Cervical pessary in unselected twin gestations for prevention of preterm labour and delivery is not recommended.
• Cervical pessary in women with short cervix on transvaginal ultrasound may reduce PTB and adverse neonatal outcome, but the exact cervical length threshold to intervene is not clear.
• 17-alpha-hydroxyprogesterone caproate (17-OHPC) given intramuscularly weekly has not been shown to be effective in twin gestation for reducing SPTB in unselected twin pregnancy or twin pregnancy where the cervix is short.
• Daily vaginal micronised progesterone has not been shown to be effective in reducing SPTB in unselected twin gestation.
• Daily vaginal micronised progesterone may be effective in reducing SPTB and its consequences in twin gestation where the cervix is short (< 25 mm) before 24 weeks of gestation, but results are conflicting and current international guidelines do not go as far as to recommend its use.
https://doi.org/10.1017/9781108915038.020 Published online by Cambridge University Press
Table 20.1 Summary of management options for prevention of spontaneous preterm delivery in multiple pregnancy
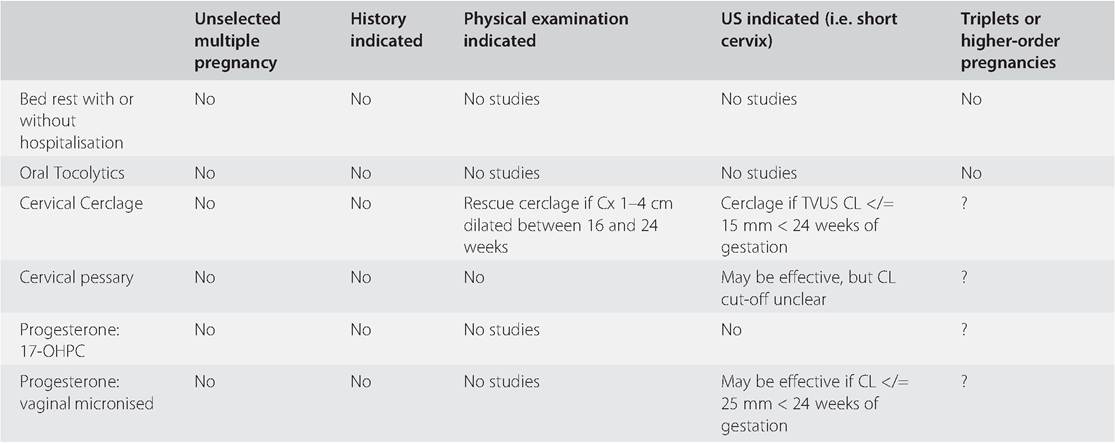
US = ultrasound; Cx = cervix, TVUS = transvaginal ultrasound; CL = cervical length; 17-OHPC = 17-alpha-hydroxyprogesterone caproate
• There is little published evidence to guide recommendations for any intervention to reduce SPTB in triplet or higher-order multiple pregnancy.
Acknowledgements
The author would like to acknowledge Nour Adra, medical student at the American University of Beirut, for her valuable contribution to the content of this chapter, notably through her assistance in finding the relevant literature and organising the list of references.
References
1. Adra A, Khalife D, Usta I et al. Practice patterns of obstetric care in twin gestation: the value of MFM consultation. J Matern Fetal Neonatal Med September 2020;20 (9): 1-7.
2. SMFM Research Committee, Grantz K, Kawakita T et al. SMFM special statement: State of the science on multifetal gestations: unique consideration and importance. Am
J Obstet Gynecol 2019;221(2):B2-B12. https://doi.org/10.1016/j.ajog.2019.04.013
3. Crowther CA, Han S. Hospitalization and bed rest for multiple pregnancy. Cochrane Database Syst Rev 2010, issue 7 Art. No: CD000110.
4. Ashworth MF, Spooner SF, Verkyul DA, Waterman R, Ashurst HM. Failure to prevent preterm labor and delivery in twin pregnancy using prophylactic oral salbutamol. BJOG 1990;97:878-82.
5. American College of Obstetricians and Gynecologists. Multifetal gestations: twin, triplet and higher-order multifetal pregnancies. Practice Bulletin Number 169. Obstet Gynecol 2016;128:e131-e146.
6. Rottenstreich A, Levin G, Kleinstern G et al. History-indicated cervical cerclage in management of twin pregnancy. Ultrasound Obstet Gynecol 2019;54:517-23.
7. Rafael TJ, Berghella V, Alfirevic Z. Cervical stitch (cerclage) for preventing preterm birth in multiple pregnancy. Cochrane Database Syst Rev 2014;9:CD009166.
8. Roman A, Rochelson B, Fox NS et al. Efficacy of ultrasound-indicated cerclage in twin pregnancies. Am J Obstet Gynecol 2015;212(788):e1-e6.
9. Adams TM, Rafael TJ, Kunzier NB, Mishra S, Calixte R, Vintzileos AM. Does cervical cerclage decrease preterm birth in twin pregnancies with a short cervix? J Matern Fetal Neonatal Med 2018;31(8):1-7.
10. Roman A, Zork N, Haeri S et al. Physical exam indicated cerclage in twin pregnancy: A randomized controlled trial. Am J Obstet Gynecol 2020;223 (6):902.e1 -902.e11. https://doi.org/10.1016/j.ajog.2020.06.047
11. Li C, Shen J, Hua K et al. Cerclage for women with twin pregnancies: a systematic review and meta-analysis. Am J Obstet Gynecol 2019;6:543-557.
12. Nicolaides K, Syngelaki A, Poon L et al. Cervical pessary for prevention of preterm birth in unselected twin pregnancies:
a randomized controlled trial. Am J Obstet Gynecol 2016;214:3.e1-e9.
13. Goya M, De la Calle M, Pratcorona L et al. Cervical pessary to prevent preterm birth in women with twin gestation and sonographic short cervix: a multicenter randomized controlled trial (PECEP-TWINS). Am J Obstet Gynecol February 2016;214(2):145-52. https://doi.org/10.1016/j.ajog.2015.11.012
14. Norman JE, Norrie J, MacLennan G et al. The Arabin pessary to prevent preterm birth in women with a twin pregnancy and a short cervix: the STOPPIT 2 RCT. Health Technol Assess. 2021 Jul;25(44):1-66. https//:doi.org/10.3310/hta25440
15. Conde-Agudelo A, Romero R, Nicolaides K. Cervical pessary to prevent preterm birth in asymptomatic high-risk women: a systematic review and meta-analysis. Am J Obstet Gynecol July 2020;223(1):42-65.e2. https://doi.org/10.1016/j.ajog.2019.12.266
16. Schuit E, Stock C, Rode L et al. Effectiveness of progestogens to improve perinatal outcome in twin pregnancies: an individual participant data meta-analysis. BJOG 2015 January;122(1):27-37.
17. Dodd JM, Grivell RM, Obrien CM, Dowswell T, Deussen AR. Prenatal administration of progestogens for preventing spontaneous preterm birth in women with a multiple pregnancy (review). Cochrane Database SystRev 2019 (11). Art. No: CD 012024.
18. Rehal A, Benko Z, Matallana C et al. Early vaginal progesterone versus placebo in twin pregnancies for prevention of spontaneous preterm birth (EVENTS):
a randomised double-blind trial. Am J Obstet Gynecol 2021;224(1):86.e1-86. e19. https//:doi.org/10.1016/j.ajog.2020.06.050
19. Durnwald C, Momirova V, Peaceman A et al. Second trimester cervical length and risk of preterm birth in women with twin gestations treated with 17 alpha hydroxyprogesterone caproate. J Matern Fetal Neonatal Med 2010;23(12):1360-4.
20. Senat M, Porcher R, Winer N et al. Prevention of preterm delivery by 17 alpha-hydroxyprogesterone caproate in asymptomatic twin pregnancies with
a short cervix: a randomized controlled trial. Am J Obstet Gynecol 2013;208(194): e1-e8.
21. Klein K, Rode L, Nicolaides K, Krampl- Bettelheim E, Tabor A for the PREDICT Group. Vaginal micronized progesterone and risk of preterm delivery in high-risk twin pregnancies: secondary analysis of a placebo-controlled randomized trial and meta-analysis.Ultrasound Obstet Gynecol 2011;38:281-7.
22. El-refaie W, Abdelhafez MS, Badawy A. Vaginal progesterone for prevention of preterm labor in asymptomatic twin pregnancies with sonographic short cervix: a randomized clinical trial of efficacy and safety. Arch Gynecol Obstet 2016;293: 61-7.
23. Romero R, Conde-Agudelo A, El-Refaie W et al. Vaginal progesterone decreases preterm birth and neonatal morbidity and mortality in women with a twin gestation and a short cervix: an updated meta-analysis of individual patient data. Ultrasound Obstet Gynecol 2017;49:303-14.
24. Sentilhes L, Senat MV, Ancel PY et al. Prevention of spontaneous preterm birth: Guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF). Eur J Obstet Gynecol Reprod Biol 2017(210):217-24.
25. National Institute for Health and Care Excellence. Multiple Pregnancy: Antenatal Care for Twin and Triplet Pregnancies. Clinical Guideline no. 129. London: National Institute for Health and Care Excellence, 2011.