Quality, respectful care after stillbirth
Stillbirth has a profound impact on the mother, father, and families and also healthcare providers and societies worldwide with substantial psychosocial and economic burden (14).
Extreme shock and distress is commonly experienced by parents and families at diagnosis of a fetal death. The majority of grieving mothers have significant grief-related depressive symptoms which often last for many years (14). Fathers also experience overwhelming and long-lasting grief and may find it difficult to express themselves (15). The lifechanging effects of stillbirth on the family extend to siblings, grandparents, and the wider family (Figure 34.5).The needs of parents
A recent survey of bereaved parents conducted by the International Stillbirth Alliance (ISA), sought the most important things parents wanted to know when their baby was stillborn. The findings are summarized in Box 34.1. Overwhelmingly, parents wanted to know why their baby died, a question that included both cause of death, reasons for its occurrence, and whether it could have been prevented. These questions were associated with questions about their pregnancy and labour and a pervading sense of guilt among mothers, who asked whether they had done something wrong and if their baby had suffered. Other questions were about the baby's

Figure 34.5 Ned and Heidi with Sophie, who was stillborn.
appearance and current location and information about the immediate care of the mother. Missed opportunities to answer the parents' questions might be avoided by simple measures that recognize the parents' need to know about their child (Box 34.1). A recent review showed that fathers want to be involved in decision-making and often focus on practical tasks (15).
Parents face many difficult decisions in the context of overwhelming grief and frequently have a diminished capacity to absorb and retain information.
Fathers want to protect and support their partner and may feel frustrated and helpless if they cannot do this (15). Maternity staff who provide calm, supportive, and objective information, balancing guidance with parental autonomy, can assist parents to make informed decisions and minimize regret. Staff should ensure their own values and opinions do not influence grieving parents. Critical information should be repeated, and verbal information should be reinforced with parent-centred printed materials. Parents need to be given privacy, time, and honesty. The more time dedicated to discussions with parents and the more information made available, the easier it is for parents to discuss dilemmas and find answers to questions. In the ISA surveys, parents often reported less than optimal care after the stillbirth, particularly to do with information sharing and decision support (3) (Figure 34.6).Acknowledgment and understanding
The grief women experience after stillbirth may be aggravated by social stigma, blame, and marginalization (2). Negative perceptions and misunderstanding of stillbirth are commonplace and are major barriers to appropriate support for parents and families who have a stillborn child. Parents often report feelings that their stillborn child is less valued in the community than the death of an older child. In
Box 34.1 What do parents want to know after their baby is stillborn? Summary of qualitative survey data (n = 3503)
Why and how
• Why did it happen?
• How did it happen?
About the baby
• Where is my baby? What is happening to my baby?
• Did my baby suffer?
• Details about the baby—weight, eye colour, gender, and length.
• How can we create memories of our baby (including holding and caring for the baby and taking the baby home)?
• What are we 'allowed' to do (e.g. baby care, funerals, birth certificates, and taking the baby home)?
About care in pregnancy and labour
• Did I do something wrong?
• Why didn't they listen to me (voiced by women who felt that concerns raised in pregnancy were ignored or dismissed)?
• Why not sooner? This related to a range of care decisions made in their pregnancy.
About their own care
• How do I cope?
• How do I tell other children?
About the future
• Can we have another baby? How soon?
• What are the chances of stillbirth happening again?
• How long will it take to get over this?
Source data from Flenady V, Wojcieszek AM, Middleton P, Ellwood D, Erwich J, Coory M, et al. Stillbirths: recall to action in high-income countries. The Lancet 2016;13(387):691-702.
poorer regions of the world in particular, parents also consistently report that their baby was perceived as a taboo object and linked to sins of the mother (2). Even in HICs, negative perceptions are commonplace. Fatalistic attitudes that stillbirth is inevitable (‘nature’s way’) are not only inaccurate and unhelpful to parents but hold back efforts in prevention as many stillbirths are due to conditions that are potentially preventable.
Privacy but not abandonment
Parents should be given privacy during the hospital stay, and generally away from sounds of crying babies, and all staff should be aware of their loss. Parents often report feeling abandoned after a stillbirth and, while privacy is important, this should not impede the provision of optimal care.
Parenting and creating memories
Spending time and parenting the baby is often associated with positive memories and can aid the grieving process by creating a bond and sense of identity of the child. Activities such as seeing and holding a stillborn baby should be carefully and compassionately offered and parents supported in their choice (16). ‘Cuddle cots’ (or similar) (Figure 34.7) provide a cooled environment enabling parents to spend more time with their baby and are being increasingly used. Memory-making activities should be suggested and parents supported in their decision about these options. These activities may include bathing and dressing the baby, talking to the baby and using the baby’s name, engaging in religious or naming ceremonies, introducing the baby to extended family, and capturing interactions in photographs and movies.
Having items of memorabilia may reduce negative outcomes and should be offered such as photos, hand/footprints, and special clothing or blankets (17).Healthcare professional support
While high-quality evidence on specific interventions to improve outcomes for parents after stillbirth is lacking (18), a recent systematic review including non-randomized studies highlighted the importance of actions and attitudes of staff (15). Caring for bereaved parents requires understanding of the current evidence on perinatal loss, the impact of losing a baby, and the diversity of parents’ experiences (19). A parent-centred approach that addresses sociocultural context and respects the unique needs of each bereaved parent underpins compassionate communication, and information provision and supported decision-making is vital (19). Continuity of care following diagnosis of stillbirth is important to parents. A coordinated multiprofessional approach to care with staff well known to the parents is critically important from the time of diagnosis and birth through to follow-up visits and ideally, for those wishing to have another baby, into subsequent pregnancies. Stillbirth has a significant impact on obstetricians and midwives, professionally and personally, and many feel inadequate in providing care at this time with training and support often lacking (15, 20). Perinatal bereavement care requires organizational responses including staff development to address training gaps and debriefing and clinical supervision to prevent burnout of staff in highly emotionally demanding roles.
Follow-up after leaving the hospital
With little evidence to guide the type and frequency of follow-up, it is important that parents are aware of support services available to them and that a time is made for a follow-up visit to the hospital. Upon discharge, parents should be provided with the contact number of a staff member known to them to respond to questions that may arise before the follow-up visit, and to also suggest to them to make a list of questions in preparation for their follow-up visit.
Many parents find it very distressing to return to the unit where their baby was stillborn and, where possible, these appointments should take place in another setting. If practicable, the option of home visits should be offered to parents. Six to eight weeks is the usual timing of the follow-up appointment with the aim to have all results of investigations available. If important results will not be available at that time (e.g. autopsy), parents need to be made aware and an alternate or additional appointment time made. Once again, compassionate, respectful care is critical to the parents at this time. Referring to the baby by name is important to many parents where a name was given. A coordinated, thoughtful, and multiprofessional approach to care is needed. In addition to discussion on the reasons for the death, counselling about future pregnancy planning should include attention to optimal maternal health including smoking cessation support and weight management if relevant (21). In addition, the visit should include discussion of parent’s grief and coping and recommendations or referral for ongoing support if necessary.Social and tangible support
Adequate social support from family and local social networks can improve outcomes for parents. Family and friends and the wider
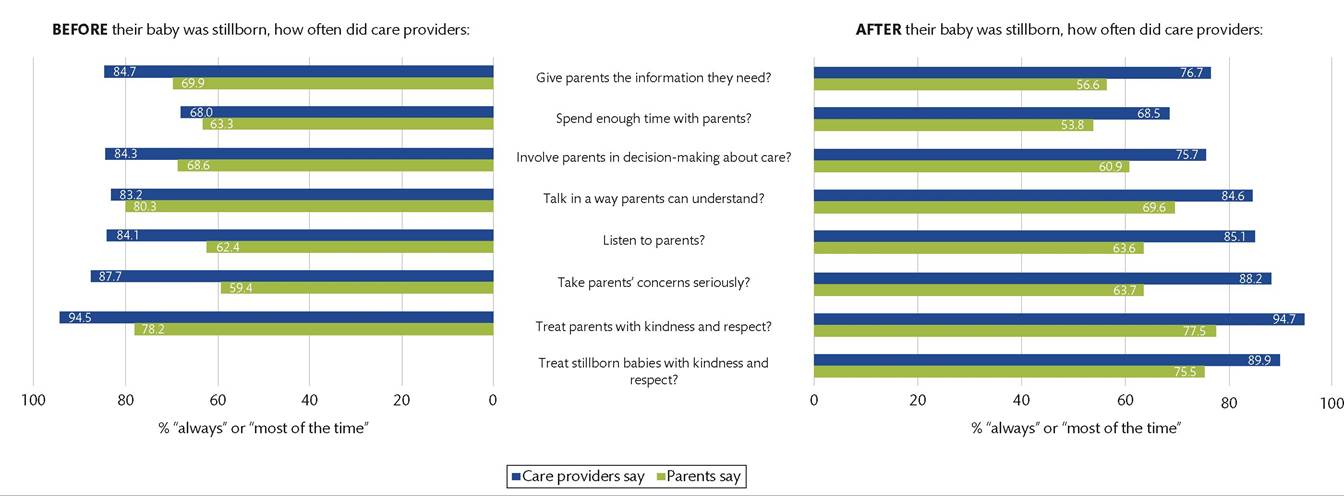
Figure 34.6 Quality antenatal and bereavement care: survey data from parents (n = 3503) and care providers (n = 2020). Data from parents refers to the care parents, themselves, received in the pregnancy in which their baby was stillborn. Datafrom care providers refers to the care provided to all parents, in general, at each care provider's facility.
Reproduced from Flenady V1 WojcieszeFAM1 Middleton P1 Ellwood D1 Erwich I1 Coory M1 et al. StiIIbirths: recall to action in high-income countries. The Lancet 2016; 13(3.37): 691 -702 with permission from Elsevier.

Figure 34.7 A 'cuddle-cot' which is designed to cool a stillborn baby to enable parents to spend longer time with their baby after birth.
community need to understand the enormity of the loss of stillbirth to parents and the need for their child to be acknowledged as part of the family. Effective leave arrangements and tangible support, such as government assistance with funeral costs, and paid leave from work commitments is important for parents (14).
Mental health interventions
Grief is a normal response and most parents and families do not require specialized services including professional counselling. High-risk groups who may have complicated grief such as parents who have previously lost children, and women undergoing termination of pregnancy for fetal anomalies, may benefit from referral to specialists services. Prescribing sedatives for women is common in some settings, despite the addictive nature of these medications and the limited evidence for benefit. Pharmacological management of grief should only be considered in the presence of an established psychological disorder for which medication is indicated.