Recent developments
New devices for hysteroscopy: imaging systems with readily portable cameras and light sources can be used in examination rooms that are not solely dedicated for hysteroscopy; they enable more flexible use of space.
Endosee
The Endosee device (CooperSurgical) is a hand- held, battery- operated hysteroscopy system that consists of two main parts. The ‘HandTower’ contains a small (3.5-inch diagonal) touchscreen liquid-crystal display monitor, with video and control electronics and a rechargeable battery. The hysteroscopes are single-use, semi-rigid curved cannulas with a diameter of 3.5 mm and a length of 287 mm. The lens camera and light source are placed at the tip and comprise a digital processing chip. There is a port at the proximal end of the cannula to which can be attached a syringe or inflow tubing for saline irrigation. Results of observational studies using the device for diagnostic hysteroscopy have provided promising preliminary results (50-52).
TELE PACK X LED
The TELE PACK X LED (Karl Storx) although not an entirely new system has been upgraded and now incorporates a new LED light source and a 15-inch LED back light monitor (Figure 48.1). In addition, surgical procedures can now be downloaded and recorded via USB ports or on a SD card slot. It remains a portable, all-in-one system, comprising a light source and a monitor, and can be used with all Karl Storz one-chip camera heads and a variety of endoscopes. It is suitable for use in the office setting or operating theatre.
Intrauterine morcellation
Intrauterine morcellation devices with mechanical removal of pathology under direct vision and using normal saline for a distension have been developments that warrant reporting. Smaller devices are now available and from the results of a trial comparing electroresection with hysteroscopic morcellation it seems that the latter is particularly useful for endometrial polypectomy in the outpatient setting in both pre- and postmenopausal women (53). Polyp removal with the morcellator was quicker, less painful, and more likely to be complete than with electrosurgical resection.
Complications are usually self-limiting and consist of vasovagal reactions and a single episode of endometritis. Other pathologies that can be removed with hysteroscopic morcellators include submucosal fibroids and placental remnants as well as adhesions and uterine septa (54-56).
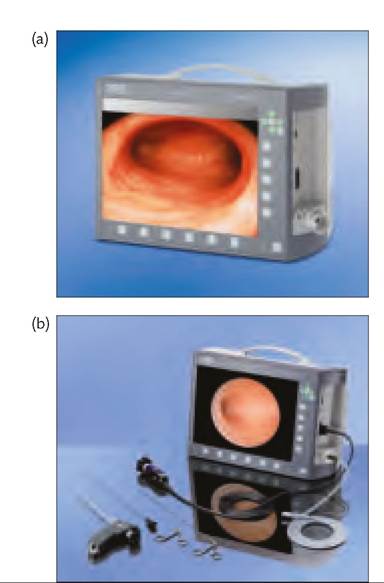
Figure 48.1 (a) TELEPACK X LED; (b) TELEPACK X LED with office hysteroscopy set.
Reproduced from Mencaglia, L., Cavalanti de Albuquerque Neto, L., and Arias Alvarez, R., Manual of Hysteroscopy, 2011, with permission from Endo Press.
The relative safety of hysteroscopic morcellators in all settings needs to be confirmed by the assessment of larger patient cohorts. In the meantime, audit of treatment complications and outcomes is required.