Risk factors for pelvic floor trauma
Some women are at higher risk of severe childbirth trauma than others. In recent years, attempts have been made to identify and modify risk factors in order to prevent perineal trauma.
Of the numerous factors associated with perineal trauma, ethnic origin, nulliparity, and maternal age are considered non modifiable factors. The potentially modifiable risk factors are mainly obstetric: macrosomia, epidural anaesthesia, prolonged second stage of labour, instrumental delivery, and episiotomy.Maternal risk factors
Ethnicity
A meta-analysis of admittedly heterogeneous studies showed that Asian ethnicity was associated with an increased risk of severe perineal trauma (48). A United States study of maternal morbidity in ethnic groups also found that severe perineal trauma was more likely in Asian women and was the least common complication in nonHispanic black women (49). Similarly, a study in Californian hospitals found that Asian women had disproportionately high rates of major trauma (50). Interracial marriages, larger babies, gestational diabetes, and increasing body mass index (BMI) were considered responsible for the increased risk in this study. Another study showed that South Asian women have a threefold higher rate of OASIS compared to Australian women (51). However, in this study women were categorized according to the country they were born in.
The variation in perineal trauma rates among different ethnic groups has been attributed to differences in anatomy, skin thickness, and resistance as well as communication challenges. Women may misunderstand instructions during the course of labour and delivery (51). Asian women seem to have a weaker skin, less resistant to stretching (52). A reduced lumbar curvature may result in intraabdominal forces directed more towards the pelvic floor rather than the anterior abdominal wall (53).
Parity
Nulliparity is a non-disputable risk factor for OASIS. Reduced tissue elasticity seems to play a role. Anal sphincter injuries were associated with nulliparity (odds ratio (OR) 9.8; 95% confidence interval (CI) 3.6-26.2) in a study by Zetterstrom et al. (54). Smith et al. showed that 6.6% of nulliparous and 2.7% of multiparous women sustained OASIS after vaginal delivery. The incidence of intact perineum was 9.6% and 31.2% in nulliparous and multiparous women, respectively (1). Lower rates of OASIS of 1.7% were found in a study of 20,000 vaginal deliveries with a similar difference in incidence between prim- iparous women at 2.9% and multiparous at 0.8% (55).
A retrospective cohort study (56) of 20,674 deliveries also concluded that anal sphincter trauma occurred in 16% of women with first vaginal deliveries and 18% with vaginal birth after caesarean section. A meta-analysis by Oberwalder et al. (57) showed a 26.9% incidence of anal sphincter defects in nulliparous women and an 8.5% incidence of new sphincter defects in multiparous women.
The first vaginal delivery seems to have the greatest impact as a risk factor for POP (58). A study by Mant et al. (59) showed that compared with nulliparous women, women with one child were four times more likely and women with two children were 8.4 times more likely to experience POP. Leijonhufvud et al. also showed an increased risk of both stress incontinence and POP with increasing parity (60).
Maternal age
Maternal age has been commonly identified as a risk factor mainly because of the adverse impact of ageing on tissue integrity and elasticity. Maternal age at the time of first delivery seems to have a significant association with pelvic floor trauma (61). Changes in biomechanical properties of the pelvic floor with increasing age may be responsible for the increased pelvic floor injury rates.
Hornemann et al. found maternal age to be the second most important risk factor for severe perineal lacerations (62).
However, clear cut-off threshold values for maternal age could not be defined in this study.Rortveit and Hunskaar (40), however, showed that women 25 years or younger at first birth had a lower risk of incontinence than older women (23% vs 28%; P <0.01). Groutz et al. found that first vaginal delivery at an older age carries an increased risk for postpartum stress urinary incontinence (63).
Smoking
Nulliparous women who smoked throughout pregnancy had a 28% lower risk of OASIS compared to non-smokers (64). Multiparous women also showed comparable findings, although not statistically significant. Nonetheless, the usefulness of these findings is limited, as smoking cannot be recommended due to the other severely adverse outcomes it may cause. These results may be due to the negative effect of smoking on fetal growth (29).
Body mass index
Women with a higher BMI appear less likely to sustain OASIS despite being more likely to have macrosomic babies and instrumental deliveries (65-67). While increasing BMI was correlated with a lower incidence of OASIS, there was an increase in first- and second- degree tears (68). An explanation for the protective effect of higher BMI, although not evidence based, is that the increase in adipose tissue increases the elasticity of the perineum. Also, obese women may have larger perineal bodies.
Obesity was found to be a risk factor for POP in parous women. Dolan et al. (69) reported an almost fourfold increased likelihood of severe stress urinary incontinence in obese women.
Obstetric factors
Instrumental delivery
Instrumental delivery and particularly forceps (41,70, 71) delivery is an independent risk factor for severe perineal trauma (72). Forceps and vacuum delivery is associated with an increased risk of faecal incontinence by two- to sevenfold (71, 73). Vacuum extraction is generally thought to be less traumatic than forceps. A meta-analysis (74) has implicated both modes of operative delivery, with forceps carrying a greater risk than vacuum.
The shanks of the forceps require more space and may cause injury by additional stretching of the introitus and perineum.Duration of the second stage of labour
A prolonged second stage of labour has been associated with an increased risk of neuromuscular injury. Cheng et al. (75) found that third- or fourth-degree tears were increased when the second stage of labour was prolonged. Maternal exhaustion may necessitate instrumentation, which itself increases the risk of perineal trauma. However, a prolonged second stage of labour does not only result in maternal exhaustion, but sustained pressure on the perineum also predisposes to pelvic floor injury. Prolonged active second stage of labour predisposes to pudendal nerve injury (76).
Episiotomy
Episiotomy is the commonest obstetric procedure; however, there is little evidence to demonstrate any benefit from routine episiotomy. Episiotomy has been shown to double the risk of OASIS when used in non-instrumental deliveries, supporting its restrictive use (77).
Restrictive use of episiotomy seems to reduce perineal and anal sphincter trauma. A Cochrane review showed that compared with routine use, restrictive episiotomy resulted in less severe perineal trauma (relative risk (RR) 0.67; 95% CI 0.49-0.91) (78). The ideal episiotomy rate should be no more than 20-30%. Routine episiotomy did not prevent urinary incontinence at 3 months postpartum according to Klein et al. (79).
There are different types of episiotomy. The most common ones are midline or median and mediolateral episiotomy. Compared to mediolateral episiotomy, median episiotomy increases the risk of anal sphincter injuries (79) (Figure 59.6).
Regional anaesthesia
The effect of epidural analgesia on the rates of perineal trauma is complex, due to many confounding factors. Some studies showed protective effects (80) and others harmful effects (81) as well as no effect (82). The harmful effects seen in studies may be a result of its association with instrumental deliveries (83) as after controlling for instrumental delivery, epidural use was no longer a risk factor for perineal trauma (84).
Epidural analgesia is used in more nul- liparous than parous women. Those with epidural analgesia have a longer second stage of labour, an increased use of augmentation of labour and more use of epidural analgesia with the occipitoposterior position may increase the risk of anal sphincter damage (85, 86). On the other hand, women with epidural analgesia have a higher rate of episiotomy and epidural analgesia results in a more controlled second stage that might reduce the risk (85).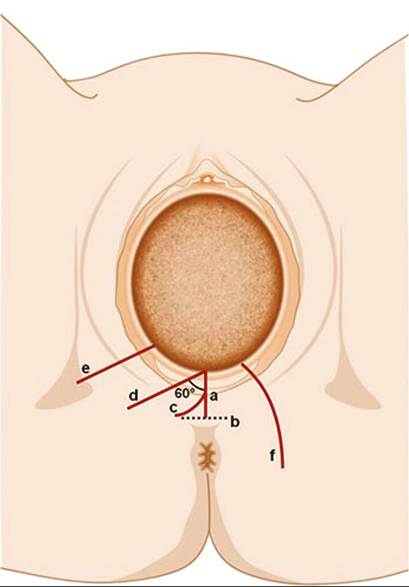
Figure 59.6 Types of episiotomy: (a) midline episiotomy; (b) modified median episiotomy; (c) J-shaped episiotomy; (d) mediolateral episiotomy; (e) lateral episiotomy; (f) radical lateral (Schuchardt incision).
Reproduced from Kalis et al. Episiotomy. In: SK Doumouchtsis (Ed) Childbirth Trauma, p. 71 (2016) with permission from Springer.
Oxytocin augmentation and birth position
Oxytocin augmentation has been linked with increased perineal trauma and particularly OASIS (87). The lithotomy position has also been associated with increased risk of OASIS irrespective of parity (88). This may be due to increased pressure directed to the anal sphincter during expulsion compared to lateral positions. However, women delivering in the lithotomy position often had other risk factors such as high birthweight, fetal malpresentation, and prolonged labour.
Malpresentation and malposition
In vacuum-assisted deliveries, occipitoposterior position was a significant risk factor for OASIS (OR 4.7; P <0.001) (89). Persistent occipitoposterior position leading to a difficult delivery increases postpartum incontinence (90). Face and brow presentations also increase the risk of incontinence because of the larger presenting diameter.
Fetal factors
Birthweight
Increased birthweight has been shown to increase perineal trauma and subsequently predispose to damage of pelvic floor innervation and stress incontinence (1,91), with some stating that weight of more than 4000 g has the greatest negative impact on perineal trauma (2).
Increased birthweight is associated with third- and fourth-degree tears, pudendal nerve injury, and significantly weaker anal squeeze pressures (76) and stress incontinence (92, 80). De Leeuw et al. showed a significant correlation between birthweight and third- degree tears (93).
Vaginal birth of macrosomic babies may be associated with disruption of the fascial supports of the pelvic floor and injury to the pelvic and pudendal nerves. Shoulder dystocia and manoeuvres used were also associated with an increased risk of anal sphincter damage (94).