Screening and Diagnosis of Complications of Shared Placentation
Caitlin D. Baptiste and Lynn Simpson
| Screening | Diagnosis | Management | |
| Twin-to-twin | Ultrasounds q2 weeks | Quintero staging | Stage I: Consider |
| transfusion syndrome | starting at 16 weeks | system: | expectant |
| assessing: | Polyhydramnios (MVP | management with | |
| MVP of each sac | > 8 cm) in one twin | ultrasound | |
| Identification of fluid- | and oligohydramnios | surveillance at least | |
| filled bladder in each | (MVP < 2 cm) in the | once per week. | |
| twin | other twin | Stages II, III, IV: Referral | |
| +/- Doppler flow of | Fluid-filled bladder | to fetal centre for laser | |
| the umbilical artery if | not visible in the | treatment if between | |
| there is discordance in | donor twin for 60 | 16 and 25 6/7 weeks. | |
| MVP or growth | minutes Doppler abnormalities Hydrops fetalis in one or both twins Death of one or both twins | Otherwise, consider amnioreduction. Stage V: Counsel on 10% risk of death and 10-30% risk of neurologic complications for cotwin. Consider expectant management. | |
| Selective intrauterine | Perform fetal growth | Estimated EFW of | Type I: Expectant |
| growth restriction | assessments q3-4 | either twin is 20% Staging system (based on umbilical artery Doppler's of IUGR twin: | Consider delivery between 34 and 37 weeks. Types II/III: Discuss options for selective termination via cord occlusion if prior to |
(cont.)
| Screening | Diagnosis | Management | |
| Positive end- diastolic flow Persistent absent or reversed end- diastolic flow Intermittent absent or reversed end- diastolic flow | viability. After viability, if expectant management is pursued, at least weekly ultrasound are recommended, or inpatient admission may be considered. Delivery between 32 and 34 weeks may be considered for REDF or AEDF, respectively. | ||
| Twin anaemia polycythaemia syndrome | Perform MCA Doppler studies q2 weeks starting at 20 weeks | Either: (1) MCA-PSV ≥ 1.5 MoM in one twin and ≤1.0-0.8 MoM in the other twin (2) An inter-twin MCA- PSV discordance ≥ 1.0 MoM | Weekly ultrasound surveillance at diagnosis Optimal timing and type of treatment remain unclear |
| Twin-reversed arterial perfusion syndrome | Screen during first- trimester ultrasound where monochorionicity is suspected and one twin appears anomalous or there is large CRL discordance | Doppler studies confirm retrograde arterial flow from the normal pump twin to the anomalous acardiac twin | Depending on gestational age at diagnosis, consider selective reduction (cord occlusion, interstitial laser or radiofrequency ablation) for anomalous twin or expectant management with increased ultrasound surveillance assessing for hydrops in pump twin. |
| Discordant anomalies | All monochorionic twin pregnancies should obtain detailed fetal anatomy between 18 and 22 weeks and a fetal echocardiogram. | Depending on gestational age at diagnosis, consider selective termination via cord occlusion of anomalous twin. Refer to appropriate medical and surgical paediatric specialists. | |
The Facts
Twins comprise 3-4% of all live births and their chorionicity greatly affects the rate of complications. In a monozygotic pregnancy, when the embryo splits ≥ 4 days after fertilisation, shared placentation, or monochorionicity, occurs. Monochorionic- diamniotic (MCDA) twins occur when an embryo splits 4-8 days after fertilisation and monochorionic-monoamniotic (MCMA) twins occur when splitting occurs ≥ 8 days after fertilisation. If division occurs ≥ 13 days after fertilisation, the twins will be conjoined. In the absence of assisted reproductive technology, 70% of twins are dichorionic. Although less than a third of twin pregnancies are monochorionic, these pregnancies account for 75% of the complications in twins.1
The estimated date of delivery for twin pregnancies should be confirmed when the crown-rump length (CRL) measures between 45 and 84 mm (around 11 0/7 to 13 6/7 weeks gestation). If there is a discrepancy in the CRL, the larger of the two should be used to estimate gestational age.2 Ultrasound after 7 0/7 but before 13 6/7 weeks is the most effective way to determine chorionicity and amnionicity. Establish chorionicity by (1) assessing the membrane thickness at the site of insertion of the amniotic membrane into the placenta, (2) identifying the T sign (monochorionic) or lambda sign (dichorionic) or (3) counting the number of placental masses.2 Please see Chapter 3 for more on zygosity, chorionicity and amnionicity.
Labelling twin fetuses allows for reliable and consistent identification of both twins. Use several characterising features to describe each twin, including location within the maternal uterus (superior, inferior, right, left), placental location (if dichorionic), placental cord insertion site, gender or discordant anomalies.
Monochorionic pregnancies may be complicated by twin-twin transfusion syndrome (TTTS), selective intrauterine growth restriction (sIUGR), twin anaemia polycythaemia syndrome (TAPS), twin-reversed arterial perfusion syndrome (TRAP) and discordant congenital anomalies.
In the setting of monoamnionicity, cord entanglement may occur. All monochorionic pregnancies are at increased risk of co-twin death, which has potential implications for the surviving twin.It remains difficult to predict in the first trimester which MCDA pregnancies will develop TTTS and how severe the condition will be. Currently, no single screening test exists to identify which MC pregnancies will develop complications and therefore all MC pregnancies are subject to costly and time-intensive antenatal surveillance, which has impact on both the patient and health care resources.3
Despite the plethora of complications monochorionic twins present, the prognosis improves with adequate surveillance and access to fetal therapy. In a recent cohort of 3,621 twin pregnancies in Denmark, 15% were monochorionic, of which 92.3% of MCDA and 66.7% of MCMA pregnancies resulted in at least one live born infant compared to 98.2% of dichorionic twins.4 It is important to remember that the frequency and location of testing (inpatient versus outpatient) also influences the survival rate of these pregnancies with a shared placenta.
The Issues
All monochorionic twins have shared circulation through vascular anastomoses in the placenta. There are three types of anastomoses: arterio-arterial (A-A), veno-venous (V-V) and arterio-venous (A-V). Blood flow in A-V anastomoses is unidirectional and can lead to
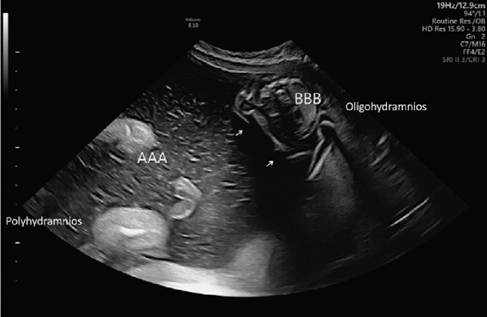
Figure 8.1 Monochorionic- diamniotic twin pregnancy with oligohydramnios-polyhydramnios sequence diagnostic of stage I IIlS. The separating membrane is seen draping around the stuck twin (arrows).
discordant blood flow between the two fetuses. If uncompensated, this unidirectional flow may lead to an imbalance of volume between the twins (Figure 8.1). The number and location of these anastomoses leads to the various complications seen in monochorionic twins.
Pregnancies affected by growth discordance or sIUGR commonly have a sharing imbalance, high rates of velamentous cord insertions and large A-A anastomoses. Pregnancies affected by TTTS commonly have low numbers of A-A anastomoses whereas pregnancies complicated by TAPS have only a few, small, A-V anastomoses and few A-A anastomoses. These complications in order of prevalence, starting with the most common, are reviewed in what follows.Twin-Twin Transfusion Syndrome
Twin-twin transfusion syndrome affects 10-15% of MCDA twins and usually occurs between 15 and 26 weeks of gestation. Although it can occur in any monozygotic pregnancy, it is exceptionally rarely seen in dichorionic-diamniotic (DCDA) twins and not often observed in MCMA twins. Twin-twin transfusion syndrome accounts for up to 17% of perinatal mortality in all twins and up to half of perinatal deaths in MCDA twins. The diagnosis is made when one twin in an MCDA twin pregnancy has oligohydramnios (defined as a maximum vertical pocket (MVP) < 2 cm) and the other twin has polyhydramnios (MVP > 8 cm).
The most common staging system by Quintero includes five stages based on sonographic findings (Table 8.1). This simple and replicable diagnostic staging system allows for standardisation of the diagnosis, improves communication between referring providers and fetal centres and helps identify cases most likely to benefit from treatment. However, it does not accurately predict outcomes or perinatal survival for an individual pregnancy. Twintwin transfusion syndrome often does not progress in a predictable manner and robust natural history data are lacking. Most natural history data predate the standardised Quintero staging and therefore outcomes in these studies are not stratified by stage.5 For example, stage I disease may evolve into stage IV or V disease without clearly progressing through stages II and III. Studies looking at the natural progression of staged disease report that 85% of stage I disease resolves or remains stable and only 15% progress to a higher
Table 8.1 Quintero staging system for twin-twin transfusion syndrome
| Stage | Findings on ultrasound |
| I | Polyhydramnios (MVP > 8 cm) in one (recipient) twin Oligohydramnios (MVP < 2 cm) in other (donor) twin |
| II | Fluid-filled bladder not visible in donor twin |
| III | Doppler abnormalities: Umbilical artery Doppler shows absent or reversed end-diastolic flow Ductus venous with reversed flow in a-wave Umbilical vein pulsations in either twin |
| IV | Hydrops fetalis in one or both twins |
| V | Death of one or both twins |
stage.5 On the contrary, stage III/IV disease presenting before 26 weeks of gestation, if left untreated, has a perinatal loss rate of 70-100%.
Screening for Twin-Twin Transfusion Syndrome in the First Trimester
Although one cannot accurately predict disease in the first trimester, findings on ultrasound between 11 and 14 weeks may predict adverse outcomes. These include discordant nuchal translucency (NT) measurements and discordant CRLs.[I] A systematic review and metaanalysis of early prognostic factors in monochorionic twin pregnancies found a significant association between NT > 95% in one or both fetuses and the development of TTTS. However, the positive predictive value of one or both fetuses having an NT > 95% was only 22%. The same review noted a significant association between CRL discordance ≥ 10% and the later development of TTTS but again, the positive predictive value was only 28%. Collectively, these first-trimester ultrasound findings have been reported to have a false negative rate of 52%.6 Although enlarged and/or discordant NT and discordant CRL demonstrate poor individual prognostic ability for the development of TTTS, the International Society for Ultrasound in Obstetrics and Gynecology recommends referral to a fetal medicine expert for all twin pregnancies where the CRL discordance is ≥ 10% or the NT discordance is ≥20%.2,3
Screening for Twin-Twin Transfusion Syndrome in the Second Trimester
Regular ultrasound in the second trimester is the mainstay of screening for TTTS. Although there are no randomised controlled trials on the optimal frequency of ultrasound surveillance in MCDA pregnancies, current recommendations suggest ultrasound every two weeks starting at 16 weeks of gestation. Ultrasound surveillance in the second trimester should include:
Screening for Twin-Twin Transfusion Syndrome with Fetal Echocardiogram
The role of routine fetal echocardiography in the assessment of TTTS remains unclear. Since the development of the initial Quintero staging of TTTS, much has been learned about the cardiovascular effects of TTTS on fetuses. Even in early stages of TTTS, changes in myocardial function are present in the recipient twin. Although several groups have evaluated changes in fetal cardiac function as a potential modifier of the current staging system, none of these proposed systems has been widely adopted. Currently, data are insufficient to change the current staging of TTTS based on findings on fetal echocardiography.
Diagnosis of Twin-Twin Transfusion Syndrome
When TTTS is diagnosed or suspected, prompt consultation with a fetal treatment centre is paramount. When indicated, laser therapy improves outcomes to a double survivor rate of 60-70% and a single survivor rate of 80-90%.2 Despite the favourable obstetric prognosis after treatment, pregnancies complicated by TTTS remain at increased risk of neurodeve- lopmental disability. Although neurologic outcomes after laser therapy are improved compared to untreated TTTS cases, 9% of surviving children of TTTS pregnancies treated with laser have major neurodevelopmental delays at 6 years of age.2 Please see Chapter 13 for further management of TTTS.
Selective Intrauterine Growth Restriction
Discordant growth, complicated by sIUGR of one fetus, affects 10-15% of monochorionic pregnancies. Discordant growth is commonly due to both vascular anastomoses and unequally shared placental territories. The smaller twin in pregnancies complicated by growth discordance commonly has a velamentous or marginal cord insertion and placental pathologic evaluation usually shows unequal placental sharing (Figure 8.2).7 This discrepant placental share may be modified, for better or worse, by placental anastomoses. The natural history of the discordant growth in MCDA twins depends on both the discordance in placental territories and the pattern of vascular anastomoses between their circulations. Therefore, when TTTS simultaneously complicates these pregnancies and laser therapy is performed, the elimination of these anastomoses can disrupt their protective effect and lead to poor outcomes for the smaller twin.
Various diagnostic criteria exist for growth abnormalities in MCDA twins. Selective intrauterine growth restriction in MCDA twins may be diagnosed if the estimated fetal weight (EFW) of either twin is 20-25% regardless of whether either twin meets criteria for IUGR and others use a combined EFW < 10th percentile and an inter-twin discordance of >20% to define sIUGR.
Both placental insufficiency and inter-twin vascular anastomoses affect the umbilical artery Doppler waveforms in MC twins. A classification system for sIUGR has been created based on Doppler assessment of the umbilical artery of the smaller twin (Table 8.2).9
The smaller twin in Type I sIUGR has positive end-diastolic flow in the umbilical artery and these pregnancies have a favourable prognosis. These cases are managed similarly to
Table 8.2 Classification of selective intrauterine growth restriction
Type Umbilical artery Doppler findings of growth-restricted fetus
I Positive end-diastolic flow
II Persistent absent/reversed end-diastolic flow
III Intermittent absent/reversed end-diastolic flow
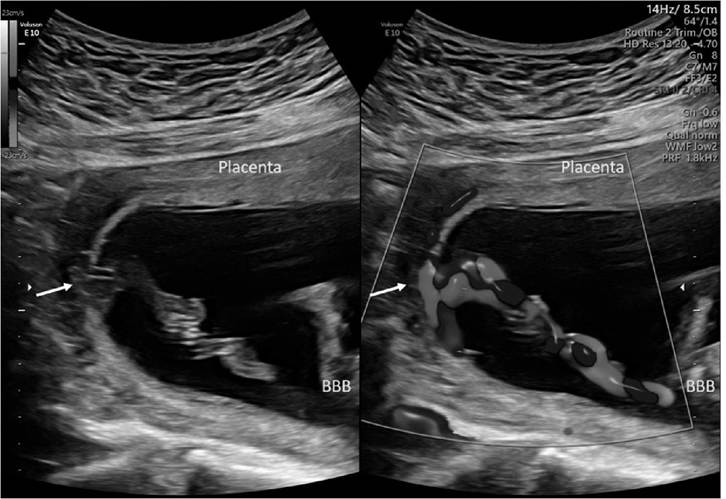
Figure 8.2 Split-screen Ultrasounddemonstratingavelamentous PCI(arrows) by two-dimensional(left) and colour flow (right) imaging with the anterior placenta severalcentimetres from the cord insertion. (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
that of singletons with IUGR with antenatal testing and indicated early delivery. Please see Chapter 16 for more on management of fetal growth pathology in multiple pregnancy. Adverse outcomes are somewhat unpredictable in these cases, but the intrauterine fetal demise rate of the smaller twin remains low at 2-4%.
The prognosis and management for Type II sIUGR, with persistently absent or reversed end-diastolic flow in the umbilical artery of the smaller twin, depends on the gestational age at diagnosis (Figure 8.3). These pregnancies are commonly affected by unequal placental sharing; the placental territory for the growth-restricted fetus is usually small and the number of vascular anastomoses fewer than with Type I sIUGR. Overall, 70-90% of Type II sIUGR cases will show signs of deterioration on fetal testing by 30 weeks of gestation. In a Japanese study in which selective termination was not available, the natural history showed
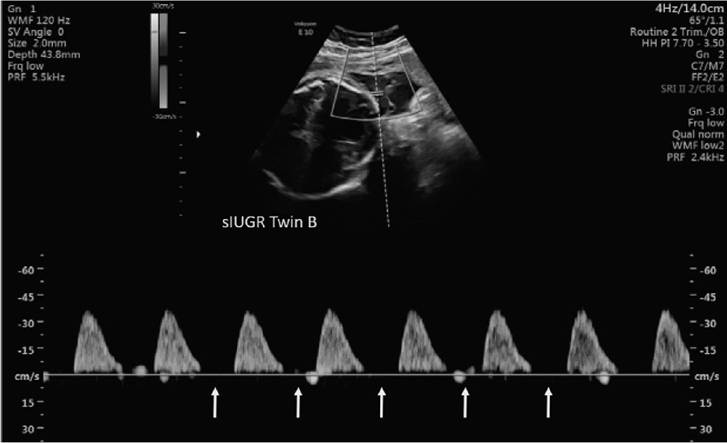
Figure 8.3 Dopplervelocimetry of an MCDA twin with sIUGR demonstrating persistent absent end-diastolic flow (arrows). (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
a 37% intact survival rate for the smaller twin and a 55% intact survival rate for the larger twin, with a mean gestational age at delivery of 28 weeks.10
In the setting of Type II sIUGR, if the pregnancy is viable, consider hospital admission to increase fetal monitoring and perform Doppler interrogation of the ductus venosus to help predict imminent fetal deterioration. If persistently abnormal Doppler findings develop prior to viability, consider selective termination via cord occlusion. A series evaluating 90 cases of Type II and III sIUGR treated with cord occlusion showed a 93% survival rate of the remaining twin with a mean gestational age at delivery of 36.4 weeks.11
In pregnancies complicated by Type III sIUGR, the Doppler studies of the umbilical artery show intermittently absent or reversed end-diastolic flow that indicates the existence of large placental A-A anastomoses. The degree of placental territory discordance may be greatest in this type of sIUGR, but the placental vascular anastomoses help compensate for the territorial discordance. Given its variable nature, it is easy to miss this Doppler finding; it is generally more prominent and easily seen near the placental cord insertion. Due to the large anastomoses, there is a higher risk of acute feto-fetal transfusion and neurologic injury to the normally grown twin even if both are born alive. Although the overall prognosis of Type III is better than Type II sIUGR, the unpredictable clinical evolution of these cases makes them difficult to manage. If expectant management is undertaken at viability, at least weekly ultrasounds are recommended.12
One of the main risks of sIUGR and discordant twin growth is intrauterine demise of the smaller fetus. As with all cases of single fetal demise in a monochorionic pregnancy, there is risk to the remaining twin (see Chapter 12 on single fetal demise). Even when both twins survive, sIUGR may be associated with neurologic impairment of one or both twins.12 This may in part be due to increased rates of prematurity but also due to the shared vasculature in utero. Please see Chapter 16 for further management of growth abnormalities in multiple pregnancies.
Twin Anaemia Polycythaemia Sequence
Twin anaemia polycythaemia sequence is a complication of monochorionic pregnancies when one twin, the donor, develops anaemia and the other twin, the recipient, becomes polycythaemic. The incidence of TAPS affects 2-5% of uncomplicated monochorionic pregnancies and 3-16% of cases post laser therapy for TTTS. Different governing bodies have different recommendations for screening and diagnosing TAPS. The International Society of Ultrasound in Obstetrics and Gynecology recommends screening for TAPS in monochorionic pregnancies starting at 20 weeks of gestation and obtaining an ultrasound every two weeks to assess the middle cerebral artery peak systolic velocity (MCA-PSV) by Doppler velocimetry. However, there is a lack of evidence that monitoring for TAPS with MCA-PSV at any gestational age, including >26 weeks, improves outcomes. Therefore, several groups, including the Society for Maternal Fetal Medicine, do not recommend performing routine screening for TAPS in otherwise uncomplicated monochorionic twin pregnancies.6,13
A recent Delphi process was conducted among international experts to determine the key diagnostic features and optimal monitoring approach for TAPS.14 Based on their consensus, monitoring for the development of TAPS should occur every two weeks, although the gestational age at which to start screening remains unclear. If TAPS is diagnosed, obtain ultrasound assessment weekly. Evaluation on ultrasound should include MCA-PSV as well as evaluating for evidence of fetal hydrops and cardiac compromise.
Expert opinion considers a diagnosis of TAPS if either of the following are detected: (1) MCA-PSV ≥ 1.5 MoM in one twin and ≤ 0.8 MoM in the other twin or (2) an inter-twin MCA-PSV discordance ≥ 1.0 MoM (Figure 8.4). Other studies suggest a diagnosis of TAPS if the MCA-PSV is >1.5 MoM in the recipient and 1.5 MoM
MCA PSV recipient < 1.0 MoM No signs of fetal compromise
Stage 2 MCA-PSV donor > 1.7 MoM
MCA PSV recipient < 0.8 MoM No signs of fetal compromise
Stage 3 MCA findings as above with any of the following:
Abnormal umbilical artery Doppler studies (absent or reversed end-diastolic flow) Pulsatile flow in the umbilical vein
Increased pulsatility index or reversed flow in the ductus venosus
Stage 4 Hydropsindonortwin
Stage 5 Intrauterine demise of one or both twins preceded by diagnosis of TAPS
* Based on Slaghekke et al. Twin anaemia-polycythaemia sequence: diagnostic criteria, classification, perinatal management and outcome. FetalDiagnosis and Therapy 2010: 27: 181-90.
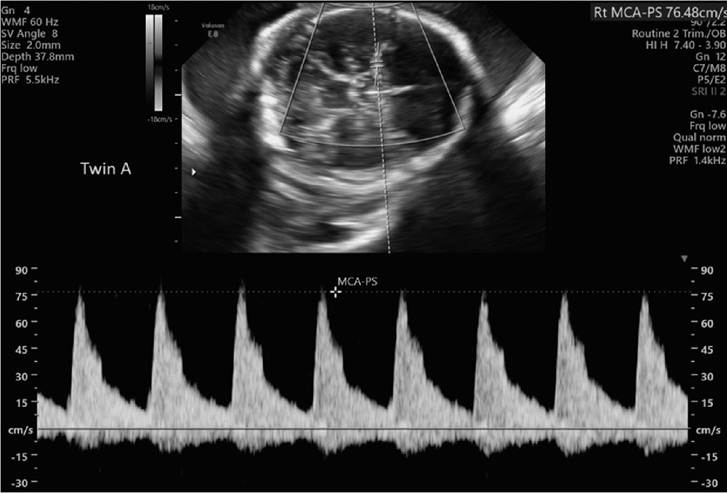
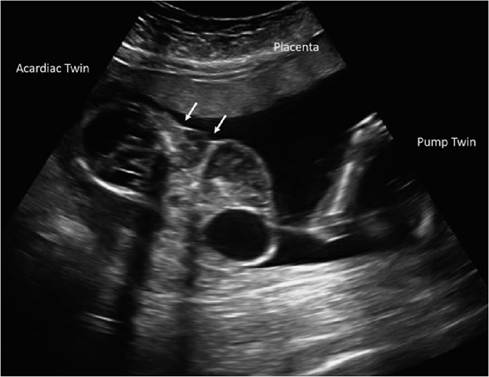
Figure 8.5 The amorphous acardiac twin of this MCDA pregnancy complicated by TRAP appeared stuck (arrows) but continued to grow in the second trimester, resulting in cardiac failure in the pump twin which wastreated with cord occlusion of the acardiac twin.
If a single demise is diagnosed in the first trimester, perform Doppler assessments to exclude reversed perfusion of the demised twin. For ongoing pregnancies affected by the TRAP sequence, one or more of the following poor prognostic factors raise the risk for pump twin mortality:16 evidence of congestive heart failure or hydrops fetalis, abnormal Doppler studies in the umbilical artery of the pump twin, EFW acardiac to EFW pump > 0.7, polyhydramnios or monoamniotic pregnancy.16 Without early detection and therapy, mortality rates for the pump twin range from 50% to 70%. Concern for the TRAP sequence should prompt an early referral to a fetal therapy centre to discuss the options of termination of the entire pregnancy, selective reduction (cord occlusion, interstitial laser or radiofrequency ablation) or conservative management with serial surveillance. The anomalies of the acardiac twin are incompatible with life, so the focus should be on improving the survival of the pump twin. Early detection, close follow-up and selective cord occlusion of a large or rapidly growing acardiac mass can increase survival for the pump twin to 80-90%. Please see Chapter 15 for further management of the TRAP sequence.
Single Fetal Demise
Due to the inter-twin vascular anastomoses within the single placenta and the acute drop in vascular resistance that occurs when one twin dies, the risk of severe neurologic handicap in the remaining twin is 10-30% with a 10% risk of death.5 Please see Chapter 12 for more details on management of single fetal demise in MC pregnancies.
Screening and Diagnosis of Complications of Monochorionic- Monoamniotic Twins
Monochorionic-monoamniotic twins make up 1-2% of all monozygotic twin pregnancies and occur when an embryo splits ≥ 8 days after fertilisation. Monochorionic-monoamniotic twins share both a chorion and amnion and lack a dividing membrane.
The absence of a dividing membrane early in pregnancy should be considered an MCMA pregnancy until a dividing membrane is visualised, which may not be possible until about 12 weeks. It is important not to incorrectly diagnose MCMA in what is actually an MCDA pregnancy complicated by TTTS where the donor twin is ‘stuck’ underneath a draped dividing membrane. In a monoamniotic twin pregnancy, both twins should move throughout the uterus and neither twin should appear stuck in the same location throughout the exam.
Monoamnionicity can be confirmed by the presence of cord entanglement on obstetric ultrasound, particularly when colour flow imaging is utilised (Figure 8.6). Cord entanglement is detected prenatally in almost all cases of MCMA twins and is responsible for the perinatal mortality rate of 70%. Recommendations for monitoring for cord entanglement and its impact on the monoamniotic twins vary. Any advice for twin surveillance, including whether monitoring should take place as an inpatient or outpatient, must balance the reduced fetal morbidity and mortality against the inconvenience and possible psychological and financial strain on the mother and her family, costs to the health care system and the possibility of iatrogenic prematurity or other adverse events.
Although the same complications that plague MCDA twins may occur in MCMA twins, the frequency varies. For example, the incidence of TTTS in MCMA pregnancies is 2-3% compared to the 10-15% seen in MCDA twins. This is likely due to the nearly universal presence of A-A anastomoses seen in MCMA twins, which are protective against TTTS and significant growth discordance.
Similar to MCDA twins, ultrasound assessment of MCMA twins may begin at 16 weeks, with assessment every two weeks pending the findings. Many providers consider admission
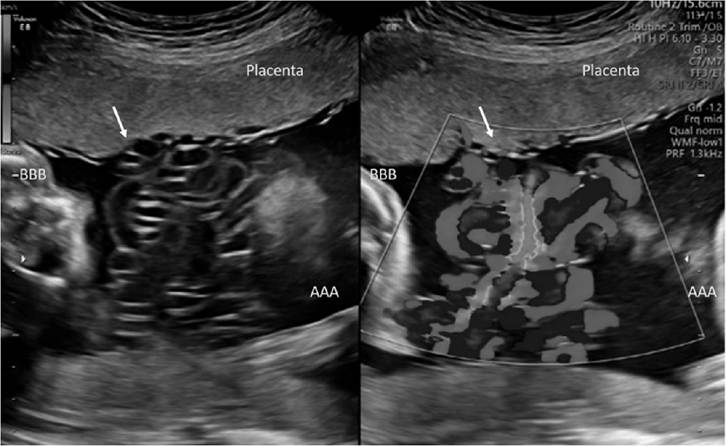
Figure 8.6 Split-screen ultrasound demonstrating Umbilicalcord entanglement (arrows) by two-dimensional(left) and colour flow (right) imaging in monoamniotic twins. (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
with increased monitoring between 24 and 28 weeks with delivery at 32-34 weeks. Great debate exists on whether and when to admit patients with MCMA twins to the hospital for increased surveillance of the twins. A recent retrospective analysis - the MONOMONO study - reported on 195 MCMA pregnancies at 22 participating sites in the United States and Europe and found no significant differences in outcomes between inpatient and outpatient monitoring. In this study, the peak fetal death rate was at 29 weeks with no fetal or neonatal deaths after 32 weeks, regardless of the location of testing.17 Please see Chapter 17 for further discussion on management of MCMA twins.
Structural Anomalies
Compared to singletons, the rate of major congenital anomalies is fourfold higher in monozygotic twins and threefold higher than that of dizygotic twins. Of monozygotic twins, those with monochorionic-monoamniotic placentation have the highest rate of congenital anomalies. The rates of discordant anomalies are also very high and thus careful attention must be paid to evaluating each fetus individually for anomalies. Given the increased rate of congenital anomalies and heart defects, all monozygotic pregnancies should undergo a detailed anatomical survey and fetal echocardiogram. While an assessment for major anomalies may occur during the first trimester, a follow-up anatomical survey at 18-22 weeks should be performed given its higher detection rate for major malformations (50% vs 70%). Please see Chapters 7 and 11 for further discussion on screening for fetal abnormalities in multiples and management of discordant twin anomalies, respectively.
Preterm Birth Risk Assessment
All twin pregnancies are at risk of preterm birth. As a screening tool for preterm birth, cervical length assessment is recommended during the fetal anatomy scan but may be obtained more frequently during the second trimester. Asymptomatic women found to have a cervical length < 25 mm in mid trimester are at an increased risk of spontaneous preterm birth. A cervical length < 20 mm between 20 and 24 weeks is a reasonable predictor of preterm birth before 32-34 weeks.2 Unfortunately, there is no effective strategy to prevent preterm birth in multiple gestations, so the impact of detecting a short cervix in a patient with twins is uncertain. Please see Chapters 19 and 20 for more discussion of preterm birth in multiple gestations.
The Management
An organised and standardised approach to the management of monochorionic twins improves outcomes. Checklists from the Society for Maternal Fetal Medicine and the American College of Obstetrics and Gynecology help optimally care for monochorionic twin pregnancies.
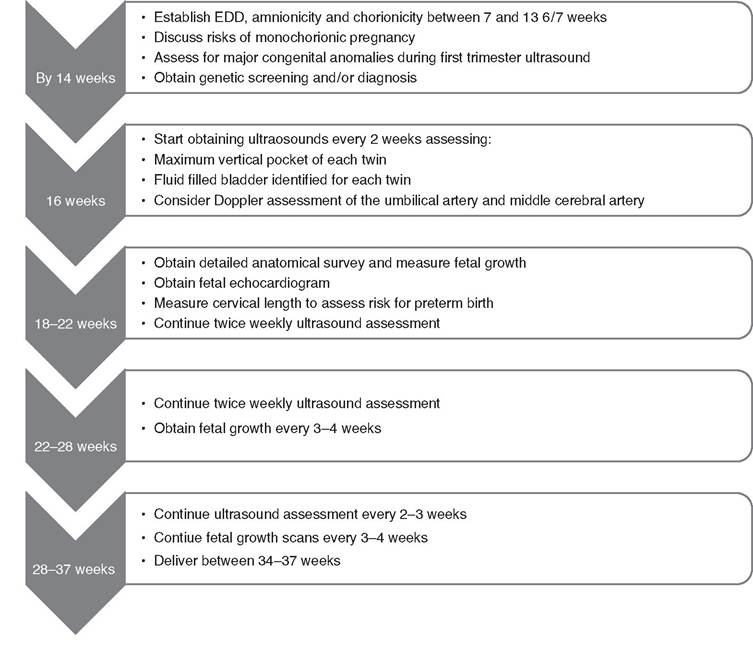
By 14 weeks, confirm the estimated date of delivery (EDD), chorionicity and amnioni- city. During the first few prenatal visits, counsel the patient on the increased maternal risks of twin pregnancies such as hypertensive disorders of pregnancy, gestational diabetes and postpartum haemorrhage. Neonatal risks including TTTS, discordant growth, sIUGR, preterm birth and the potential sequelae to a surviving co-twin in the event of a single twin demise should also be discussed early in care. Review options for genetic screening and diagnosis during the initial prenatal visit.
Begin serial ultrasound monitoring of all monochorionic pregnancies at 16 weeks of gestation. Ultrasound assessment should include measuring the MVP of each sac and visualisation of a fluid-filled bladder for each twin. Obtain ultrasounds every two weeks until 26 weeks and then every two to three weeks until delivery. Assess fetal growth every three to four weeks starting at 16 weeks and continue until delivery. Obtain Doppler studies if either twin is growth restricted or growth or fluid discordance is noted. Perform a detailed anatomical survey and a fetal echocardiogram at 18-22 weeks. If there is concern for TTTS or discordant growth with selective IUGR, consider early consultation with a fetal therapy centre. If possible, perform screening ultrasounds and serial surveillance of monochorionic twins early in the workweek to allow time for referral and travel to a fetal therapy centre to help avoid delays in care when complications are encountered.
The Society for Maternal Fetal Medicine recommends delivery of uncomplicated monochorionic diamniotic pregnancies by 37 6/7 weeks and delivery of uncomplicated monochorionic monoamniotic pregnancies by caesarean section between 32 and 34 weeks of gestation. See Chapter 23 for more discussion on delivery timing in multiple pregnancies.
Key Points
• Establish EDD, amnionicity and chorionicity in the first trimester.
• Start serial ultrasound surveillance at 16 weeks and repeat every two weeks until 26 weeks with an assessment of MVP in each sac, presence of fetal bladders and Doppler studies if TTTS and/or sIUGR are diagnosed.
• In the second trimester, obtain a detailed fetal anatomical survey and fetal echocardiogram of both twins.
• Obtain baseline cervical length in the second trimester to assess risk for preterm birth.
• Assess twin growth every three to four weeks.
• Refer to fetal therapy centre if there is concern for TRAP, TTTS, sIUGR or TAPS.
• Deliver MCDA twins between 34 and 37 weeks.
• Deliver MCMA twins between 32 and 34 weeks by caesarean section.
Management of Monochorionic-Diamniotic Twin Pregnancies
References
1. Sebire NJ, D'Ercole C, Hughes K, Carvalho M, Nicolaides KH. Increased nuchal translucency thickness at 10-14 weeks of gestation as a predictor of severe twin to twin transfusion syndrome. Ultrasound Obstet Gynecol 1997 Aug;10(20):86-9.
2. Khalil A et al. ISUOG practice guidelines: role of ultrasound in twin pregnancy. Ultrasound Obstet Gynecol 2016;47:247-63.
3. Mackie FL, Hall MJ, Morris RK, Kilby MD. Early prognostic factors of outcomes in monochorionic twin pregnancy: a systematic review and meta analysis. Am J Obstet Gynecol 2018 Nov;2019(5):436-46.
4. Kristiansen MK, Joensen BS, Ekelund CK, Petersen OB, Sandager P. Perinatal outcome after first-trimester risk assessment in monochorionic and dichorionic twin pregnancies: a population-based register study. BJOG 2015 Sep;122(10):1362-9.
5. Simpson LL. Twin-twin transfusion syndrome. Am J Obstet Gynecol 2013 Jan; 208(1):3-18.
6. Kagan KO, Gazzoni A, Sepulveda- Gonzalez G, Sotiriadis A, Nicolaides KH. Discordance in nuchal translucency thickness in prediction of severe twin-to-twin transfusion syndrome.
Ultrasound Obstet Gynecol 2007. May;29(5):527-32.
7. Da Paepe ME, Shapiro S, Young L, Luks FL. Placental characteristics in selective birth weight discordance in diamniotic- monochorionic twin gestations. Placenta 2010. May;31(5):380-6.
8. Buca D, Pagani G, Rizzo G et al. Outcome of monochorionic twin pregnancy with selective intrauterine growth restriction according to umbilical artery Doppler flow pattern of smaller twin: systematic review and meta-analysis. Ultrasound Obstet Gynecol 2017 Nov;50(5):559-68.
9. Gratacos E, Lewi L, Munoz B et al. A classification system for sIUGR in MC pregnancies according to UA Doppler flow in the smaller twin. Ultrasound Obstet Gynecol 2007 Jul;30(1):28-34.
10. Ishii K, Murakoshi T, Takahashi Y et al. Perinatal outcome of monochorionic twins with selective intrauterine growth restriction and different types of umbilical artery Doppler under expectant management. Fetal Diag Ther 2009;26 (3):157-61.
11. Parra-Cordero M, Bennasar M, Martlnez JM, Eixarch E, Torres X, Gratacos E. Cord occlusion in monochorionic twins with early selective intrauterine growth restriction and abnormal umbilical artery Doppler: a consecutive series of 90 cases. Fetal Diagn Ther 2016;39(3):186-91.
12. Bennasar M, Eixarch E, Martinez JM, Gratacos E. Selective intrauterine growth restriction in monochorionic diamniotic twin pregnancies. Seminars in Fetal and Neonatal Medicine 2017;22:376-82.
13. Slaghekke F, Kist WJ, Oepkes D et al. Twin anemia-polycythemia sequence: diagnostic criteria, classification, perinatal management and outcome. Fetal Diagn Ther 2010;27:181-90.
14. Khalil A, Gordijn S, Ganzevoort W et al. Consensus diagnostic criteria and monitoring of twin anemia polycythemia sequence: a Delphi procedure. Ultrasound Obstet Gynecol 2019 Oct 12.
15. Bornstein E, Monteaguode A, Dong R, Schwartz N, Timor-Tristch IE. Detection of twin reversed arterial perfusion sequence at the time of first-trimester screening. The added value of 3dimensional volume and color Doppler sonography. J Ultrasound Med 2008:1105-9.
16. Moore TR, Gale S, Benirschke K. Perinatal outcome of forty-nine pregnancies complicated by acardiac twinning. Am J Obstet Gynecol 1990; 163:907.
17. MONOMONO Working Group. Inpatient vs outpatient management and timing of delivery of uncomplicated monochorionic monoamniotic twin pregnancy: the MONOMONO study. Ultrasound Obstet Gynecol 2019 Feb;53(2):175-83.