Screening and prevention in gynaecology
Cervical cancer
With this background in mind, this chapter will explore past and current screening activities among women for early detection and
Box 61.1 Wilson and Jungner criteria for principles and practice of screening
1 The condition should be an important health problem.
2 There should be a treatment for the condition detected.
3 Facilities for diagnosis and treatment should be available.
4 There should be a latent stage of the disease.
5 There should be a test or an examination for the condition.
6 The test should be acceptable to the population.
7 The natural history of the disease should be adequately understood.
8 There should be an agreed policy on whom to treat.
9 The total cost of finding a case should be economically balanced in relation to medical expenditure as a whole.
10 Case-finding should be a continuous process, not just a ‘once and for all' project.
Source data from Wilson JMG, Jungner G. Principles and Practice of Screening for Disea.se. Public Health Papers No. 34. Geneva: World Health Organization; 1968.
prevention of gynaecological cancers, beginning with cervical cancer. There is a well-characterized and strong association between cervical cancer incidence and level of societal development. Approximately 86% of incident cancers and 88% of deaths from cervical cancer are estimated to occur in less developed regions of the world (7). The high incidence of cervical cancer among less educated and socioeconomically disadvantaged women is well documented (8, 9).
Cervical cancer screening and early detection
Cervical cytology testing involves collecting exfoliated cells from the cervix and examining these cells microscopically. The concept of utilizing exfoliated cells to identify women with invasive cervical cancer was introduced by Papanicolaou and Babes in the 1920s (10).
Subsequently, Papanicolaou refined his technique and in 1941 he published on the use of conventional cytology to identify invasive cervical cancers and in 1954 published on how to identify and classify cervical cancer precursors (11). In the first paragraph of theBox 61.2 Modified version of principles and practice of screening
1 The screening programme should respond to a recognized need.
2 The objectives of the screening should be defined at the outset.
3 There should be a defined target population.
4 There should be scientific evidence of screening programme effectiveness.
5 The programme should integrate education, testing, clinical services, and programme management.
6 There should be quality assurance, with mechanisms to minimize potential risks of screening.
7 The programme should ensure informed choice, confidentiality, and respect for autonomy.
8 The programme should promote equity and access to screening for the entire target population.
9 Programme evaluation should be planned from the outset.
10 The overall benefits of the screening should outweigh the harm.
Source data from Andermann A, Blancquaert I, Beauchamp S, Dery V. Revisiting Wilson and Jungner in the genomic age: a review of screening criteria over the past 40 years. Bull VPorld Health Organ 2008;86:241-320. 1941 article, the authors comment: ‘The death rate from carcinoma of the female genital tract is approximately 32,000 per year in the United States and of this figure, four-fifths or 26,000 deaths may be said to be due to cancer of the uterus. This rate has remained practically constant during the past twenty five years’. What is interesting is that in 2016, the situation in many developing countries is not very different from that in the United States more than 70 years ago. Even in 1941 it was noted that early diagnosis and treatment yielded ‘a high percentage of cures in both carcinoma of the fundus and of the cervix’. It was not, however, until the 1960s that cervical cytology began to be used widely in many developed countries as a tool for cervical cancer prevention.
Papanicolaou classified cervical cytology findings into five categories, classes I-V, and focused on how closely the cells resembled truly malignant cells (Table 61.1).
Prior to the implementation of large cervical cytology-based programmes in British Columbia, Canada, and Europe in the 1950s and 1960s, no randomized trials were performed to evaluate the impact of cervical cancer screening on cervical cancer incidence and mortality and all data on the effect of screening came from observational studies. However, the marked reduction in the incidence of and mortality from cervical cancer before and after the introduction of screening programmes in a variety of developed countries was interpreted as strong non-experimental support for organized cervical cancer screening programmes.
The International Agency for Research on Cancer (IARC) conducted a comprehensive analysis of data from several of the largest screening programmes in the world in 1986 and showed that well- organized screening programmes were effective in reducing the incidence of and mortality from cervical cancer (13). In the Nordic countries, following the introduction of nationwide screening in the 1960s, cumulative mortality rates of cervical cancer demonstrated a significant decreasing trend. The greatest decrease was in Iceland (84% from 1965 to 1982) where the screening interval was the shortest and the target age range the widest. The smallest reduction in cumulative mortality (11%) was in Norway where only 5% of the population had been part of organized screening programmes (14). The decreases in Finland, Sweden, and Denmark were 50%, 34%, and 27% respectively. The highest reduction in cervical cancer incidence was in the 30-49-year age group where the focus of screening was the most intense.
In addition, the association between mortality trends and the extent of coverage of the population by organized screening was most pronounced when the proportional reductions in the age-specific rates were related to the target ages of the screening programmes
Table 61.1 Classification of cervical cytology
| Class | Description |
| I | Absence of atypical or abnormal cells |
| II | Atypical cytology, but no evidence for malignancy |
| III | Cytology suggestive of, but not conclusive for, malignancy |
| IV | Cytology strongly suggestive of malignancy |
| V | Cytology conclusive for malignancy |
Source data from Papanicolaou GN.
Atlas of Exfoliative Cytology. Boston, MA: Commonwealth Fund University Press; 1954.(15). The age-specific trends indicated that the target age range of a screening programme was a more important determinant of risk reduction than the frequency of screening within the defined age range. This finding was in agreement with the estimates of the IARC working group, that for interscreen intervals of up to 5 years, the protective effect of organized screening was high throughout the targeted age group (>80%) (16).
It is apparent therefore that the extent to which screening programmes have succeeded or failed to decrease the incidence of and mortality from cervical cancer is largely reflected in (a) the extent of coverage of the population at risk by screening, (b) the target age of women screened, and (c) the reliability of cytology services in that programme (17).
The contrast between Finland, which had an organized screening programme, and Norway, where an equivalent number of smears were performed opportunistically, indicated another important aspect of screening. Even though the difference in the total number of smears taken in the two countries was not great, the reduction in mortality was substantial for all ages in Finland, whereas in Norway, only women aged 30-49 years showed a reduction in mortality rates: even for that age group, the reduction was only half that in Finland. These data suggest that spontaneous or opportunistic screening fails to reach the most at-risk women in the population, that is, middle-aged and older women of high relative risk, and therefore has far less of an impact on the incidence of and mortality from cervical cancer. Other reasons for the failure of opportunistic screening to reduce cervical cancer mortality include suboptimal follow-up and management of women with abnormal smears and the lack of coordinated campaigns of informing and educating women about cervical cancer prevention. This results in women at high risk of disease being excluded from screening.
Mortality from cervical cancer in the United Kingdom fell by 30% after the introduction of screening in the 1960s; however, some of this decrease in mortality was attributed to decreasing rates in older women and could have been a cohort effect unrelated to screening. The need for an effectively managed national programme in the United Kingdom was realized by the mid 1980s, which led to the introduction of a computerized call and recall system for women aged between 20 and 64 years. The invitation- based system, together with target payments for general practitioners, improved population coverage from 40% to 60% in 1989, to 80% in 1992, and to 83% in 1993. In an audit of this programme in 24 self-selected districts in the United Kingdom by Sasieni et al. (18), it was estimated that the number of cases of cervical cancer in the participating districts would have been 57% (95% confidence interval (CI) 28-85%) greater had there had been no screening. Furthermore, they estimated that screening prevented between 1100 and 3900 cases of invasive cervical cancer in the United Kingdom.
Population coverage achieved 80.6% in 2004 in the United Kingdom, but had declined to 77.8% in 2014 (5-year coverage), with the lowest coverage in the age group 25-29 years (19). Fortyseven per cent of women who develop cervical cancer in the United Kingdom have not been screened in the past 5 years or have never been screened in the United Kingdom (20).
Cervical cancer screening programmes
In many developing countries, screening is opportunistic, sporadic, or does not occur at all. In 1986, the WHO estimated that while approximately 40-50% of women in developed countries had been screened in the past 5 years, only 5% of women in developing countries had been screened. In addition, most screening activity in developing countries was limited to women attending primary healthcare, antenatal and family planning clinics in urban areas, with no organized efforts to ensure that high-risk women attended for screening, treatment, and follow-up (21).
While there is a paucity of data on screening programmes and incidence of and mortality from cervical cancer in many developing countries, there have been a number of attempts to establish screening programmes. Some of these programmes have met with marginal success; many, however, have failed to either become established or to have an impact on cervical cancer incidence and mortality. From a developing country perspective, good populationbased cancer survival data are not available in the majority of countries, particularly those in Africa, Asia, and Central America. Sankaranarayanan et al. (22), analysed 366,357 cancer cases, including cervical cancer, and nine other sites that were registered from 1990-2001 and followed up until 2003. Only two registries were included from Africa—one from the Gambia and the other from Uganda. The 5-year age-s tandardized relative survival rate (Figure 61.1) for cervical cancer did not exceed 22% in the Gambia and in Uganda the equivalent 5-year survival rate for cervical cancer was 13%. In contrast, in countries such as China, Singapore, South Korea, and Turkey the median relative survival rates were 76-82% for breast cancer and 63-79% for cervical cancer. Gondos et al. (23) evaluated the population-based Cancer Registry of Kampala which collected data on 14 of the commonest types of cancer diagnosed and registered between 1993 and 1997. The 5-year relative survival was 8.3% for patients with colorectal cancer and 17.7% for cervical cancer—the very poor survival most likely reflecting limited access to early detection and treatment.
Gakidou et al. (24) reported on cervical cancer screening from 57 countries across all levels of economic development included in the World Health Surveys, a set of household surveys implemented by the WHO in 2002. In the 30 developing countries surveyed, the population-weighted means of crude and effective coverage of cervical cancer screening were 45% and 19%, respectively. Effective coverage ranged from over 80% in Austria and Luxembourg to 1% or less in Bangladesh, Ethiopia, and Myanmar. In fact, in many countries, the majority of women have never had a pelvic examination—more than 90% of women in Malawi, Ethiopia, and Bangladesh reported never having a pelvic examination, for example.
A key limitation to establishing screening programmes in low- resource settings has been the Pap smear which requires an infrastructure with robust referral structures, reliable quality control, and human and financial resources that are not sustainable in low- and middle-income countries (LMIC). This recognition has prompted a significant paradigm shift in the thinking about cervical cancer prevention in the past 20 years, a shift that took into account the many limitations in low-resource settings as well as the competing health needs (such as infectious diseases, maternal and neonatal morbidity and mortality, human immunodeficiency virus infection (HIV), malaria, tuberculosis, among many others), the impact of war and civil strife on society and its essential structures, environmental challenges, widespread poverty, poor governance, and inadequate state expenditure on healthcare.
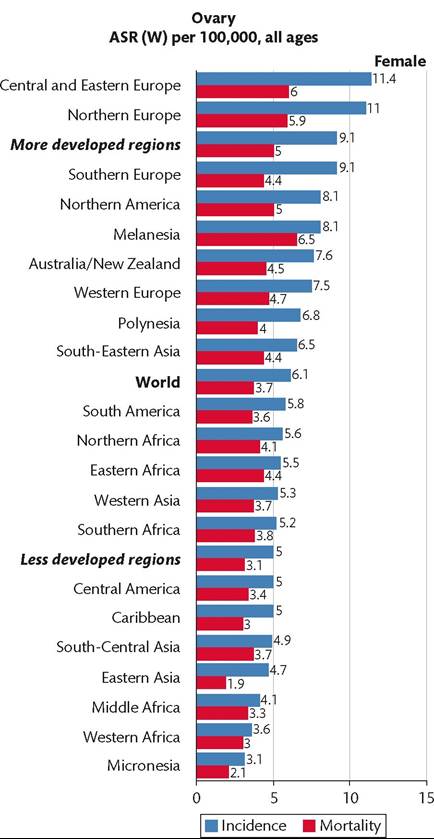
Figure 61.1 Age-standardized relative survival rate per 100,000 women in different regions of the world. ASR (W), age-standardized rate (to world standard population).
Source data from http://globocan.iarc.fr.
Initially attempts were made in India to ‘downstage’ cervical cancer by simple visual inspection with the naked eye during a genital examination. Later, the application of acetic acid (as is done in colposcopy) was added and called VIA (visual inspection with acetic acid). Many other modalities were tried including cervicography, spectroscopy, and others. Later, molecular testing for HPV DNA was introduced into the menu of options for screening women in both developed and developing countries. New technologies such as liquid-based cytology were designed to improve the accuracy of cervical cytology, which is now approved by the United States Food and Drug Administration.
Screening programmes in developing countries
In India, some attempts to establish screening programmes through hospital or clinic outpatient services and the use of mobile cancer detection clinics have shown a reduction in cervical cancer incidence. Luthra et al. (25) reported on a study in which 38,707 women
Subsequently, there have been a number of very successful screening studies conducted in India. Most recently, Shastri et al. (26) reported on a randomized controlled trial in which 75,360 women from ten clusters in the screening group and 76,178 women from ten comparable clusters in the control group were recruited in Mumbai. Women aged 35-64 years were recruited and screened by primary healthcare workers. The screening group received four rounds of cancer education and VIA at 24-month intervals, whereas the control group received one round of cancer education at the time of recruitment. Both groups were actively monitored at 24-month intervals for cervical cancer incidence and mortality. Women who were positive on VIA were referred to the local tertiary hospital where they received repeat VIA, colposcopy, and Pap smears. Those diagnosed with cervical cancer precursors or invasive cancer were treated according to standard protocols.
In the screening group, 89% of women participated and 79.4% complied with the protocol. After 12 years of follow-up, the incidence of invasive cervical cancer was 26.74/100,000 in the screening group and 27.49/100,000 in the control group. There were 67 and 98 cervical cancer deaths in the screening and control groups, respectively. This translated into a 31% reduction in cervical cancer mortality in the screening group compared with the control group (mortality relative risk (RR) 0.69; 95% CI 0.54-0.88; P = 0.003).
Parham and colleagues (27) from 2006 to 2013, up-scaled screening services (using VIA) for cervical cancer from 2 to 12 clinics in Lusaka, Zambia through which 102,942 women were screened. The majority (72%) were in the target age range of 25-49 years and 28% were HIV positive. Twenty per cent of women were VIA positive of whom 56.4% were treated with cryotherapy and 44% were referred for histopathological evaluation. Most women received same-day services (including 82% who were VIA negative and 5% undergoing same-visit cryotherapy). Among those referred for histopathological examination 44% had cervical intraepithelial neoplasia grade 2 (CIN 2) or greater. Detection rates for CIN 2+ and cancer were 17 and 7 per 1000 women screened, respectively. This study shows that screening can be performed and up-scaled in remarkably low-resourced settings. This project included many partners and leveraged funding for HIV resources that were provided by a number of organizations such as PEPFAR. The project is yet to report on the ongoing impact on cervical cancer reduction and/or prevention.
In contrast to the two very successful projects previously described, a study conducted by the WHO in six African countries in 2005 encountered many challenges, which are typical of screening programmes in low-resource settings (28). The sites chosen were Madagascar, Malawi, Nigeria, Uganda, United Republic of Tanzania, and Zambia and the study was completed in 2009. During this time period, only 19,579 women were screened from the six countries and overall 10% (n = 1980) were VIA positive and 1.7% (n = 326) had lesions suspicious for cancer. Just under 40% of women underwent screening and treatment on the same day and nearly two- thirds received treatment (cryotherapy) within a week of being screened. Of the women eligible for cryotherapy, 679 (34%) did not undergo the procedure for a range of reasons. Of the 326 women who had cervices suspicious for cancer, there was no information on 230 women and only 96 women were known to be investigated, of whom 79 had cancer and 17 either had no cancer or the outcome was unknown. Overall, 77 or the 326 women with possible cancer (24%) were known to have undergone treatment. By contrast, in the Shastri trial (26), compliance with treatment for invasive cancer was 86.3% in the screening group and 72.3% in the control group.
CONCORD-2
This seminal study (29) analysed individual tumour records from 279 population-based cancer registries in 67 countries for 25.7 million adults aged 15-99 years and 75,000 children from 0 to 14 years diagnosed with cancer during 1995-2009 and followed up to 31 December 2009. Five-year survival from colon, rectal, and breast cancers had increased steadily in most developed countries. For example, for breast cancer, 5-year survival rose to 85% or higher in 17 countries worldwide. Liver and lung cancer remained lethal in all nations with 5-year survivals ranging from 15% (North America) to 7% (Mongolia and Thailand). For cervical cancer, data were available for 602,225 women. The global range in 5-year net survival was very wide, particularly in Africa, Central and South America, and Asia. National estimates of 5-year survival ranged from less than 50% to greater than 70% with marked regional variations and very little improvement in the time periods of 1995-1999 and 2005-2009.
As mentioned earlier, cytology-b ased screening programmes have either not been initiated or sustained in many developing countries, and in particular in SSA. Research in the past years has focused on evaluating alternative approaches to screening, particularly approaches that use low technology and that can give a result if not immediately, then within a short time period, to enable women to be treated at or shortly after the screening visit. The two tests most studied are VIA and testing for HPV DNA of high-risk types known to have a causal relationship with cervical cancer.
HPV DNA testing
There have been multiple studies on the use of HPV DNA testing for secondary prevention of cervical cancer, in both the developed and developing world. A study that evaluated HPV infection in 10,575 cases of paraffin-embedded samples of histologically confirmed cases of invasive cancer from 38 countries in Europe, North America, central South America, Africa, Asia, and Oceania taken over a 60-year period, found that 85% (n = 8977) of the cases were positive for HPV DNA (30). The eight most common types of HPV detected were types 16, 18, 31, 33, 35, 45, 52, and 58 and their combined contribution to the 8977 positive cases was 91%. HPV types 16, 18, and 45 were the three most common types in each type of cervical cancer (squamous cell, adenocarcinoma, and adenosquamous carcinoma) and in the different countries studied. A recent study of HPV types in women with invasive cervical cancer in Africa which involved 570 cases of confirmed invasive cervical cancer from Ghana, Nigeria, and South Africa, found that HPV 16 infection was present in 51.2% of cases and HPV 18 in 17.2% of cases (31). Hence the distribution of HPV 16 and 18 appears to be similar in LMICs to that demonstrated in high-income countries.
Denny et al. (32) randomly assigned 6555 previously unscreened women aged 35-65 years to one of three study arms: (a) HPV and treat, in which all women with a positive HPV DNA test underwent cryotherapy; (b) visual inspection and treat, in which all women with a positive VIA test underwent cryotherapy; and (c) control, in which further evaluation or treatment was delayed for 6 months. At 36 months there was a sustained decrease in the detection of highgrade cervical cancer precursors in the HPV and treat arm compared to the control arm (1.5% vs 5.6%—difference 4.1%) and the difference in the VIA and treat arm was less at 3.8% compared to 5.6% in the control arm (difference 1.8%). In another randomized controlled trial, Sankararanayanan et al. (33) randomized 131,746 healthy women aged 30-59 years to four groups: (a) screening with HPV, (b) cytological testing, (c) VIA, and (d) standard of care which did not include screening in India at the time. They found that in the HPV testing group the hazard ratio for the detection of advanced cancer was 0.47 (95% CI 0.32-0.69). There was also a statistically significant reduction in the number of deaths from cervical cancer in the HPV group compared to the control group. There were no significant reductions in the numbers of advanced cancers and deaths in the cytological or the VIA group compared to the control group. These data support a programme that utilizes HPV DNA testing and links positive tests to treatment without the intervening steps of colposcopy and histology.
Ronco et al. (34) summarized four randomized controlled trials that used HPV-based screening for cervical cancer compared with cytology-based screening, using cervical cancer precursors as the endpoint in all trials. A total of 176,464 women aged 20-64 years were randomly assigned to HPV-based (experimental arm) or cytologybased (control arm) screening in Sweden, the Netherlands, England, and Italy. Women were followed for a median of 6.5 years and 107 cancers were identified. Detection of cervical cancer was similar between the screening methods during the first 2.5 years of follow-up (RR 0.79; 95% 0.46-1.36) but was significantly lower in the experimental arm thereafter (RR 0.45; 95% 0.25-0.81). The cumulative incidence of cervical cancer in women who had negative tests at entry was 4.6/100,000 and 8.7/100,000 at 3.5 and 5.5 years respectively in the experimental arm, and 15.4/ 100,000 and 36/100,000 respectively in the control arm. In these four randomized controlled trials, HPV- based screening provided 60-70% greater protection against invasive cervical cancer compared to cytology. The authors asserted that the data supported primary screening with HPV DNA testing with extension of screening intervals to at least 5 years.
There are currently new HPV DNA tests being developed that are not only affordable but can give results within 2.5 hours of screening, almost equivalent to a point- of-care test (35). This approach may enable larger numbers of women to be reached and enable a significant impact on cervical cancer incidence and mortality, particularly if the option of self-testing is included in the screening algorithm (36, 37).
Primary prevention of cervical cancer
Since 2006, two prophylactic HPV vaccines have been available, and each has shown a greater than 90% efficacy in preventing HPV type 16- and type 18-associated high-grade cervical cancer lesions. While both vaccines have been introduced in national immunization programmes (NIPs) in many developed countries, roll out in NIPs in LMICs has been limited. Besides cost, other challenges facing developing countries include the fact that an adolescent health platform does not exist (immunization is included in the care of young children only) and reaching the target population is not easy, the necessity for a cold chain and medical waste management, cultural issues, and reticence to discuss a sexually transmitted infection among others. Despite these challenges, most Latin American middle-income countries have introduced HPV vaccination in their NIPs; on the other hand, only two LMICs in Asia (Bhutan and Malaysia) and five sub-Saharan African countries (Botswana, Lesotho, Rwanda, South Africa, and Uganda) have introduced HPV vaccination in their NIPs as of April 2016.
Ladner et al. (38) reported on 21 HPV vaccination programmes in 14 countries that vaccinated a total of 217,786 girls. All these programmes received vaccine through the Gardasil Access Program that provides HPV vaccine at no cost to help national institutions gain experience in implementing HPV vaccination. Overall, 88.7% of the targeted populations were vaccinated with just over 90% adherence with the three-dose regimen. School-based health clinicbased models predicted high coverage as was management by a non-governmental organization. These programmes convincingly show that it is possible to introduce HPV vaccination into LMICs with a high vaccine uptake and adherence.
On World Cancer Day 2013, Gavi, the Vaccine Alliance, announced that it will provide support for the rollout of HPV vaccination in eight developing countries: Ghana, Kenya, Lao PDR, Madagascar, Malawi, Niger, Sierra Leone, and Tanzania— a price of $4.50 per dose was negotiated. After two rounds of applications, 23 countries have now been approved for Gavi assistance targeting approximately 400,000 girls for HPV vaccination (39). Further, Gavi plans to reach 30 million by 2020 by introducing the vaccine into 40 countries.
Ovarian cancer
Ovarian cancer is a rare gynaecological cancer with an estimated world age-standardized rate of 6.1/100,000, with rates between 9 and 11/100,000 in well-developed regions compared to less than 5/100,000 in less developed regions (40). In 2015, 255,700 women were expected to be diagnosed with ovarian cancer and 163,800 women were estimated to die of it in the world; the corresponding figures for less developed regions were 150,300 and 93,800 respectively. Neither early detection nor screening has been able to reduce mortality from the disease, and the only possible means of reducing mortality is prevention.
Two-thirds of women diagnosed with ovarian cancer are over the age of 55 years and a family history of ovarian or breast cancer in a first-degree relative triples the risk (41). The risk is particularly high among carriers of a BRCA gene mutation with a lifetime risk of 39-46% with BRCA1 mutations and risk of 12-20% with BRCA2 mutations (41, 42). The frequency of BRCA1 and BRCA2 germline mutations in women with ovarian cancer is reported to be between 3% and 27% (43, 44). Germline BRCA mutations are known to be associated with longer survival rates after ovarian cancer diagnosis and a generally favourable response to platin-based therapy (45, 46).
An Australian study recruited 1001 women with non-mucinous ovarian cancer into a population-based case-control study and women were screened for point mutations and large deletions in both genes (47). Survival outcomes and responses to multiple lines of chemotherapy were assessed. Germline mutations were found in 14.1% of patients overall, including 16.6% of serous carcinoma patients (high-grade serous was 22.6%). Of note, 44% had no reported family history of breast or ovarian cancer, and patients carrying mutations had improved rates of progression-free survival and overall survival. In the relapse setting, patients carrying mutations more frequently responded to both platin and non-platin regimens than mutation-negative patients, even those with early relapse post primary treatment. Another important factor to consider in testing for BRCA1/2 mutations is the significant activity of poly (ADP-ribose) polymerase inhibitors in BRCA mutation carriers (48).
Epithelial ovarian cancers have been traditionally divided according to morphological appearance but it now clear that they are a heterogeneous groups of cancers primarily classified by cell type into serous, mucinous, endometrioid, clear cell, transitional, and squamous cell tumours. They are further subdivided into benign, borderline, and malignant carcinomas depending on the degree of cell proliferation, nuclear atypia, and stromal invasion (49). Recently, based on histopathology, immunohistochemistry, and molecular genetic analysis, at least five main types of ovarian cancer are identified: high-grade serous carcinoma (70%), endometrioid carcinoma (10%), clear cell carcinomas (10%), mucinous carcinomas (3%), and low-grade serous carcinoma (<5%) (50). These tumours account for 98% of ovarian carcinomas, can be reproducibly diagnosed on light microscopy, and are inherently different diseases as indicated by differences in epidemiological and genetic risk factors, precursor lesions, patterns of spread, molecular events during oncogenesis, response to chemotherapy, and prognosis (50, 51).
Screening for ovarian cancer
The discovery of cancer antigen 125 (CA125) initiated a sustained effort to identify and use biomarkers to detect ovarian cancer. Transvaginal ultrasound is the other early detection method that has been evaluated widely with CA125 for the early detection of ovarian cancer. Most studies, however, produced disappointing results— even with a specificity of 99% it was evident that as many as 25 surgeries would need to be performed to uncover one case of ovarian cancer (52). Unfortunately, at this moment, there is no reliable early detection test that can detect ovarian cancer in its early stages. There is no convincing evidence to support the introduction of organized screening programmes for ovarian cancer in public health services.
In 2015, Jacobs et al. (53) published data on a trial in which postmenopausal women aged 50-74 from 13 centres in the United Kingdom were recruited. Women were randomly allocated to annual multimodal screening (MMS) with serum CA125 augmented with ultrasound and interpreted with use of the risk of ovarian cancer algorithm, annual transvaginal ultrasound screening (USS) or no screening in a 1:1:2 ratio. The primary outcome was death due to ovarian cancer. A total of 202,638 women were randomized; 50,640 to MMS, 50,639 to USS, and 101,359 to no screening. At a median follow-up of 11.1 years, 1282 cases of ovarian cancer were diagnosed. Of the women diagnosed with ovarian cancer, in the MMS group 0.29% had died of ovarian cancer, 0.30% in the USS group, and 0.34% in the no-screening group. Using the Cox proportional hazards model, a mortality reduction of 15% over 1-14 years was evident in the MMS group and 11% in the USS group. Overall, the reduction in deaths from ovarian cancer in the three groups was not statistically significant, although there was a trend in favour of MMS in years 7-14, if prevalent cases were removed and primary peritoneal cancers were excluded. In an editorial in response to the article, Narod et al. (54) point out that the goal of screening is to prevent death from cancer and that the trial by Jacobs et al. (53) observed a reduction in the annual hazard of dying of ovarian cancer in the short term (the mean follow-up period from diagnosis to death was 2.3 years). They contend that it is necessary to wait for 1012 years from diagnosis to conclude that an ovarian cancer patient is cured and there are many factors that delay the time from diagnosis to death but do not reduce the absolute numbers of deaths. Whether screening will prevent death from ovarian cancer or delay it by a few years is still too early to tell. Based on all deaths from ovarian/peri- toneal cancers over the entire period, the hazard ratio was 0.89 and was not significant (P = 0.23).
Prevention of ovarian cancer
There are several ways that the risk of epithelial ovarian cancer may be reduced both in high- and average-risk women; however, much less is known about the means to prevent germ cell and stromal tumours. Studying women with BRCA1 and BRCA2 mutations have provided opportunities to address the feasibility and outcome of prophylactic surgery in the prevention of pelvic serous ovarian carcinoma. Rebbeck et al. (55) identified women with germline disease-associated BRCA1 or BRCA2 mutations who had undergone prophylactic oophorectomy from 11 different institutions. Of 259 subjects who underwent prophylactic oophorectomy, 8 (3.1%) received a diagnosis of ovarian cancer or primary papillary serous peritoneal cancer at or after oophorectomy compared to 58 of 292 matched controls who did not undergo surgery (19.0%). Of the eight cancers in the surgical group, six were stage one ovarian cancers diagnosed at the time of surgery. Neither breast nor ovarian cancer developed in 185 out of 259 subjects who underwent prophylactic oophorectomy.
Crum et al. (56) proposed a model of pelvic serous cancer that is comprised of two distinct pathways of tumour development. The first accepts that Mullerian epithelium is established in the ovary over time in the form of endosalpingiosis, cortical inclusions, or endometriosis. These cells could evolve through metaplasia, or exfoliation of tubal epithelial cells, among other routes, into cancer. These cells could serve as the epithelial source for serous carcinoma. The second pathway Crum et al. (56) propose entails malignant transformation of the distal fallopian tube mucosa, initiating as tubal intraepithelial carcinoma within pre-existing normal-appearing but probably genetically altered epithelium.
Over the last decade, ovarian cancer has been divided into two basic categories that have different aetiologies, molecular pathogenesis, and clinical behaviour. Type 1 tumours are less common, present at a lower stage, and usually arise from a precursor lesion (57). Type 2 tumours present with advanced stage disease and account for the majority of deaths from ovarian cancer (58). There is now evidence to support the proposal that most type 2 ovarian cancers develop from epithelial cells of the fallopian tube, making prophylactic salpingectomy a mode of primary prevention.
Strategies with potential to prevent ovarian, fallopian tube, and peritoneal cancer include the following:
• Oral contraception reduces the risk of both type 1 and 2 ovarian cancer and is considered safe in BRCA1 and BRAC2 mutation carriers (59).
• Tubal ligation both in the general population and high-risk women (60).
• Risk-reducing salpingo-oophorectomy may reduce ovarian cancer by 80% in women with BRCA1 and BRCA2 mutations (55).
• Improved identification and genetic testing of women who are at inherited high risk of ovarian cancer—although the Australian study showed that 44% of women with BRCA1 and BRCA2 gene mutations did not give a family history of ovarian cancer (61).
• Salpingectomy as an alternative strategy to other sterilization techniques to be performed opportunistically at the time of hysterectomy or other pelvic surgery to potentially reduce the incidence as well as death rates from ovarian cancer in the general population, albeit high-quality data on the impact in the general population is lacking as ovarian cancer is a rare disease (62).
• Other risk-reducing strategies include parity and a history of breastfeeding.
Endometrial cancer
Endometrial cancer primarily affects postmenopausal women at an average age of diagnosis in the sixth decade of life. It is the most common invasive gynaecological cancer in developed countries and its incidence in developing countries is increasing. Globally, 345,000 new cases and 82,400 deaths were estimated to occur in 2015. In the United States, 54,900 new cases and 10,200 deaths were estimated to occur in 2015. The number of newly diagnosed cases in Europe in 2012 was 100,000, with an age-standardized incidence rate of 13.6 per 100,000 women (63). In the mid 1970s there was an increased diagnosis of endometrial cancer in the United States of 15,000 cases in excess of the prevailing trend, which was and is attributed to the widespread use of unopposed oestrogen in postmenopausal women. Other risk factors associated with endometrial cancer include:
• obesity
• polycystic ovarian syndrome
• tamoxifen use
• nulliparity
• early menarche
• late menopause
• oestrogen-producing ovarian tumours.
Women with hereditary non-polyposis colorectal cancer (HNPPC/Lynch syndrome) have a markedly increased risk of endometrial cancer compared to women in the general population, ranging from 20% to 60% (64, 65).
There is no evidence that population-based screening has a role in the early detection of endometrial cancer among women at moderate risk and who are asymptomatic. There is no standard or routine test that can be used for detection of endometrial cancer. Screening women for endometrial cancer has only been recommended for women with hereditary Lynch syndrome. Women at risk for endometrial cancer should be educated and strongly advised to report any abnormal symptoms ranging from abnormal bleeding to vaginal discharge and/or pelvic pain.
Factors associated with a decreased risk of endometrial cancer:
• Oral contraception (66).
• Physical activity (67).
Factors associated with an increased risk of endometrial cancer:
• Increased exposure to excess and prolonged endogenous oestrogen, as occurs in women who are obese, experience anovulation secondary to polycystic ovarian syndrome, nulliparity, early menarche, and late menopause (68). Most women with endometrial cancer have an identifiable source of excess oestrogen and typically have a high body mass index, together with other components of the metabolic syndrome, such as diabetes, hyperlipid- aemia, and hypertension (69).
• Exogenous exposure to oestrogen as a risk factor for endometrial cancer was first shown in 1975 and subsequently confirmed in other studies leading to the withdrawal of prescribing unopposed oestrogen in women with a uterus. This resulted in a rapid decrease in endometrial cancer incidence (70-72). It is estimated that the use of unopposed oestrogen therapy increases the risk for endometrial cancer 10- to 30-fold if treatment continues for 5 years or more (73).
• Combined oestrogen-progestin replacement therapy. Beral et al. (74) in the Million Women Study, conducted a cohort study in the United Kingdom in women aged 50-64 years and observed a statistically significant decreased risk of endometrial cancer associated with continuous combined oestrogen-progestin therapy compared to never users (RR 0.71; 95% CI, -0.56 to 0.90).
• In other landmark studies, the Women's Health Initiative (WHI) Postmenopausal Hormone therapy trials were launched in 1991 and recruited 161,808 women. The trials had two studies, the oestrogen and progestin (E+P) study of women with a uterus and a group randomized to placebo, and the oestrogen-alone study of women without a uterus and a similar group who were given placebo. Over 100 publications were written from the data collected over a 15-year period, and the findings were dramatic. In the E+P group compared to placebo there was an increase in heart attack, risk of stroke, blood clots, and breast cancer, but a decrease in colorectal cancer and fewer fractures (75).
• In the oestrogen-alone group, compared to placebo there was no difference in risk for heart attack, there was an increased risk of stroke and blood clots, the effect on breast cancer was uncertain, there was no difference in risk for colorectal cancer, but there was a reduced risk of fracture (75).
• In 2013, Manson et al. (76), reported an integrated overview of findings from the two WHI hormone therapy trials with extended post-intervention follow-up in 27,347 postmenopausal women aged 50-79 years enrolled from 40 centres in the United States.
• Overall, the risks of E+P during the intervention phase outweighed the benefits but many of the benefits dissipated in the post-intervention phase. However, cardiovascular disease events remained non-significantly elevated and a reduction in endometrial cancer emerged.
• However, overall, the data from both arms of the study did not support the use of E+P or E alone for the prevention of chronic disease.
Early detection of endometrial cancer
All women at menopause should be advised on the risk factors and early symptoms and signs of endometrial cancer and strongly encouraged to report any postmenopausal bleeding, spotting, pain while urinating, and vaginal discharge to their doctor and seek prompt medical attention. Primary care practitioners should reoriented to recognize early symptoms and signs in order to recognize those with suspected endometrial cancers and promptly refer them.
Measuring endometrial thickness by USS and endometrial sampling with cytological testing have been proposed as screening modalities for endometrial cancer. However, there is no evidence to support their role as primary screening modalities for endometrial cancer in asymptomatic postmenopausal women (77). The sensitivity of the Pap test is too low to be suitable for endometrial cancer screening. Although endometrial cancer may be diagnosed following pelvic examination, USS, and biopsy in symptomatic women, there is no evidence that screening by endo- or transvaginal USS and endometrial sampling reduces mortality from endometrial cancer in asymptomatic women. In women with postmenopausal bleeding, the sensitivity of endometrial sampling to detect endometrial cancer and atypical hyperplasia and endometrial disease, including endometrial polyps, is low (78). On the other hand, screening for endometrial cancer among asymptomatic women may be associated with harms due to anxiety, unnecessary biopsies, discomfort, and infections.
Screening for vulval and vaginal cancer
There are no known screening tests for the prevention of either vulval or vaginal cancer; however, greater health awareness may lead to early detection of disease and better clinical outcomes. Both are rare diseases, both have a relationship with HPV 16 infection, and both are more common in women with previous cervical or anal abnormalities.
Two types of vulval cancer are described: basaloid/warty types and keratinizing types. The basaloid warty types are associated with younger women and similar risk factors as for cervical cancer and HPV infection of the cervix. The keratinizing cancers have a low prevalence of HPV infection, occur in older women, and are frequently associated with background lichen sclerosus et atrophicus (79, 80). Over the past decades, the incidence of vulval intraepithelial neoplasia (VIN) and invasive vulval cancer have been increasing, with data emerging from population-based studies (81, 82).
The majority of cancers of the vulva are squamous (>90%). HPV DNA is identified in more than 80% of VIN lesions, whereas 4050% of invasive vulval cancers have identifiable HPV DNA (83). In 2005, an expert working group was convened by the IARC (84). The group performed a meta-analysis on studies that had done genotyping in intraepithelial and invasive anogenital cancers, specifically for HPV 16. Most studies were performed in Europe and the United States. These studies combined showed HPV prevalence of 84% in VIN with 87.7% in VIN 3 and 40.4% of 1873 vulval cancers. HPV prevalence in vaginal intraepithelial neoplasia (VAIN) was 93.6%, and was 100% in VAIN 1 but 70% in 136 vaginal cancers. Overall prevalence in anal intraepithelial neoplasia (AIN) was 92.7%, 94% of AIN 3 lesions and 84.3% in 955 anal cancers. Other types of HPV were found in all the various lesions; however, over three-quarters of HPV-positive cases were HPV 16 in this analysis.