The management of normal labour
Labour is a physiological process and the management of normal labour should focus on fetal and maternal monitoring and the provision of analgesia when required or requested. Surveillance of the progress of labour allows interventions to be introduced when appropriate.
The first stage
Evidence suggests that the low-risk woman in spontaneous labour can have intermittent auscultation of the fetal heart rate for 1 minute every 15 minutes in the first stage of labour. A landmark randomized controlled trial (6) showed that continuous electronic fetal monitoring in these women did not significantly improve fetal outcomes when compared to intermittent auscultation but resulted in higher intervention rates such as caesarean sections and operative vaginal deliveries. In this study, the incidence of neonatal seizures was higher in the intermittent auscultation group but short-term and long-term neurological and developmental outcomes were similar in both groups.
Friedman proposed that, in the active phase of the first stage of labour, cervical dilatation should progress at the rate of at least 1 cm/ hour (2). This represented the lower tenth centile of the rate of cervical dilatation in a cohort of spontaneously labouring nulliparous women. Expectant management is appropriate in labours which are progressing normally. Routine amniotomy is not shown to be beneficial (7). Proponents of amniotomy argue that this allows visualization of the colour of the amniotic fluid which, if clear, is a hallmark of the healthy fetus. There may also be a modest shortening of the duration of labour following amniotomy (8).
The second stage
Women who have reached the second stage of labour and who are being monitored by intermittent auscultation should have the fetal heart rate recorded for 1 minute every 5 minutes soon after a contraction. There is evidence that delayed pushing or allowing a period of passive second stage (‘pelvic phase'), that is, not encouraging bearing down efforts immediately, reduces the need for operative vaginal delivery (9).
An upright or squatting position during the second stage is also associated with a reduction in need for this intervention. Some birth attendants use a ‘hands-on' technique for vaginal delivery where their hands are used to guard the maternal perineum in an attempt to prevent perineal lacerations. Evidence appears to show that both a ‘hands-on' or a ‘hands- poised' approach give similar outcomes (10) though expert consensus on this matter is quite divided. Performing an episiotomy routinely for delivery is not recommended. A policy of restricted versus liberal use of an episiotomy is shown to reduce the risk of severe perineal injury (11). An episiotomy is more commonly performed when a big baby is suspected, in the presence of malposition of the fetal head and during operative vaginal delivery with the forceps or ventouse. If an episiotomy is performed, a mediolateral episiotomy is less likely to be associated with obstetric anal sphincter injuries than a midline episiotomy (12).The third stage
Following delivery of the fetus, the uterus contracts. Shortening muscle fibres in the myometrium result in a reduction in the surface area underlying the placenta. This causes detachment of the placenta. Active management of the third stage of labour is a
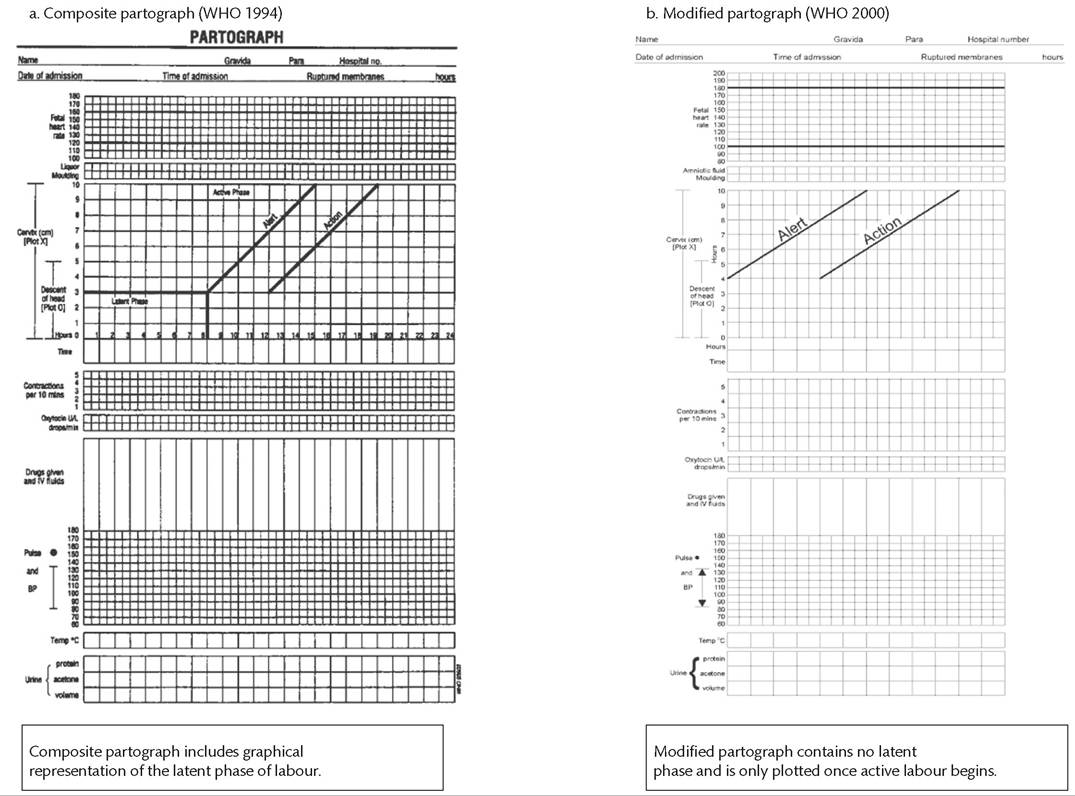
Figure 26.1 Twoversions of the WHO partogram: the composite partogram includes a latent phase with 'Alert'and Action' lines as proposed by Philpott. The modified partogram does not include a latent phase.
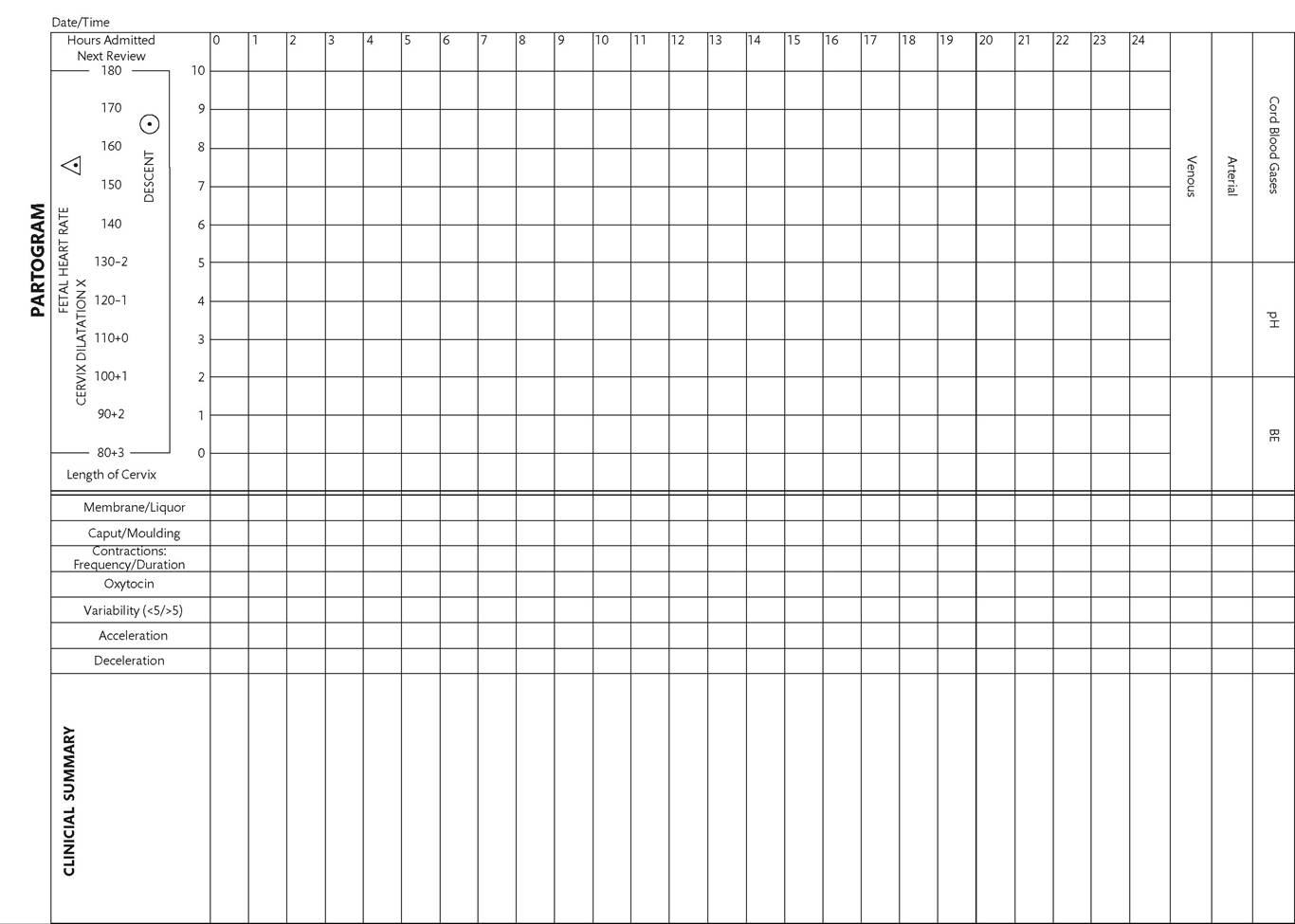
Figure 26.2 The partogram used at the Singapore General Hospital. 'Action'and Alert' lines are omitted. Spaces are allocated for clinical documentation.
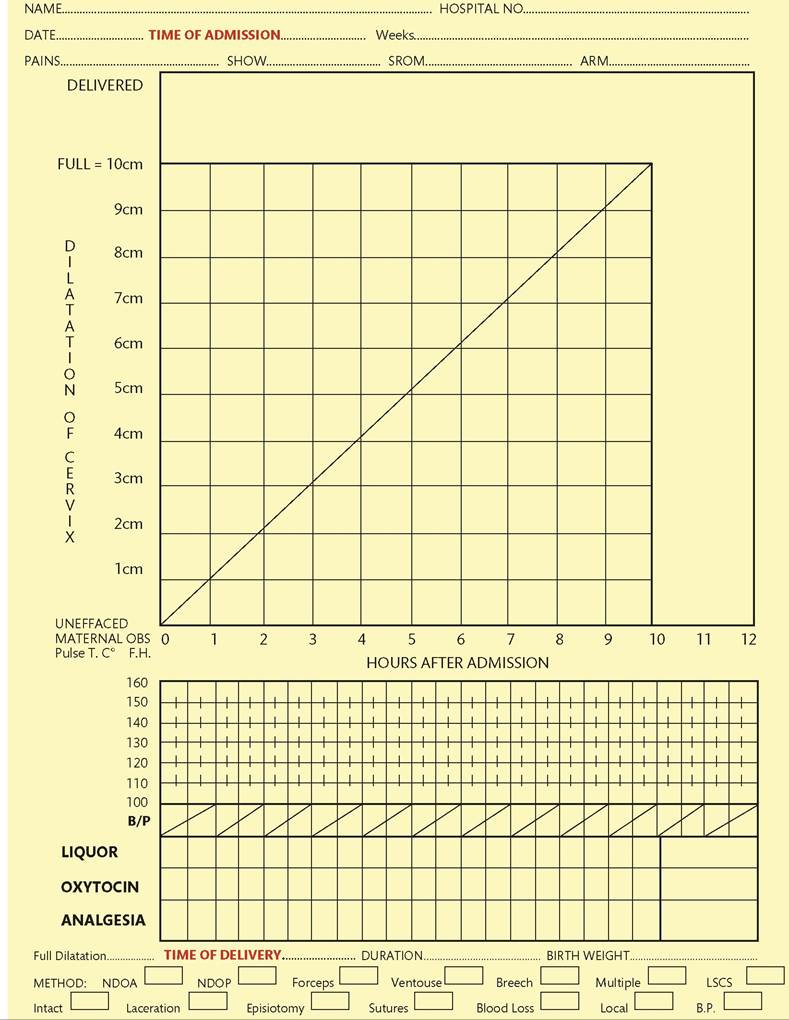
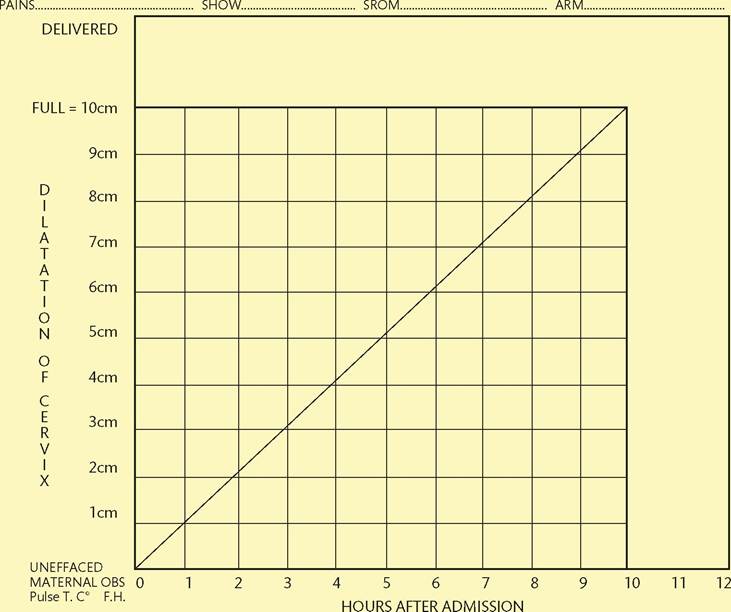
Figure 26.3 The active management of labour partogram used at the National Maternity Hospital in Dublin, Ireland, which does not include a latent phase.
fundamental aspect of modern obstetrics and has been shown to reduce postpartum blood loss. Active management of third stage refers to administration of a uterotonic, controlled cord traction, and uterine massage. The WHO recommends oxytocin as the first- choice prophylactic uterotonic (13) though, in clinical practice, a combination of oxytocin and ergometrine is also commonly used. Both preparations show similar efficacy in reducing postpartum haemorrhage but the combination of oxytocin and ergometrine is associated with a higher incidence of hypertension as well as nausea and retching.
Delayed clamping of the umbilical cord refers to the practice of occluding the umbilical cord between 1 and 3 minutes following delivery and not immediately after. Evidence shows that this practice is beneficial because it reduces neonatal anaemia and reduces the prevalence of iron deficiency in the infant at 4 months (14). This may have potentially positive effects on neonatal development. It has also been shown that delayed cord clamping does not result in adverse effects with the exception of a modest increase in neonatal jaundice. Fears that delayed cord clamping may result in increased postpartum blood loss because controlled cord traction is also delayed have proven to be unfounded. A large randomized controlled trial by the WHO has shown that controlled cord traction and uterine massage are not essential components of the active management of the third stage of labour with the use of oxytocin. However, if ergometrine is used, there is an increased incidence of retained placenta. Hence, controlled cord traction can safely be delayed without resulting in an increase in postpartum blood loss (15).