Transport of the Pregnant Patient
Pam Adams and C. David Adair
The main objective of obstetric transports is to provide safe and rapid transport of the high-risk obstetrics (HROB) patient to a facility most appropriate to meet the needs of the mother and the fetus (1).
This is accomplished by careful assessment, stabilization, and transport by skilled personnel who are comfortable dealing with obstetric and neonatal crisis and emergencies. There is definitive evidence that perinatal and neonatal outcomes are significantly improved when delivery occurs in a tertiary referral center that includes a Level 3 NICU. In utero transport results in reduced morbidity for infants of high-risk pregnancies. There is a 90% survival rate for infants transported in utero versus an 81% survival rate of out-born infants transported after delivery, proving that in most cases the mother is truly the best transport incubator (2).There are many factors that must be considered when caring for a pregnant patient in the transport environment. Foremost is an understanding that two patients are being transported. The fetus cannot be visually assessed; therefore, the crew must be trained in assessment of the fetus in utero. This includes training in reviewing and interpreting fetal monitoring tracings as well as having knowledge of antepartum testing. The teams must understand that all treatments and interventions provided to the mother have the potential to adversely or positively affect the status of the unborn fetus.
Interfacility transfers are classified as either one-way transports or two-way transports. A one-way transport involves moving the patient using a local transport vehicle (ground ambulance or helicopter) that can respond promptly and move the patient from one facility to another. During a one-way transport, the referring physician calls for a transport vehicle and then usually remains responsible for the patient’s care until she reaches the receiving facility.
This type of transfer can be tricky as many referral facilities turn the patient over to a transport crew that they assume will provide the same level of care that was given at the referring facility. The reality is that many times the level of care is actually decreased in transport, without the knowledge of the referral physician who is still ultimately responsible for that patient throughout the transfer. If the patient’s condition worsens en route, appropriate evaluation and intervention are dependent on the skill level and expertise of the transport personnel. In an effort to address this potential problem, referring facilities may desire to send one of their nurses or physicians with the patient. This can lead to added problems, as those persons are often unfamiliar with the uniqueness of transport medicine. They are not accustomed to working in the unstable environment of a moving transport vehicle where vibration, motion, noise, and a cramped, poorly lit workspace make it challenging to continually assess and alter patient care. In addition, should the patient originate from a small community facility, the facility may not be able to function well with one less caregiver or ambulance for several hours while they are on a transport (3).A two-way transport usually involves using the transport system that is associated with or contracted by the receiving facility. With a two-way transport, the receiving facility accepts responsibility of the patient when their transport team arrives and assumes her care. This type of transport is usually preferable for the receiving facility, as the caregivers on this transport team often originate from and are viewed as an extension of the receiving facility. They work under standing protocols designed to meet the needs of this type of obstetric patient. Should a situation arise where they have questions or concerns regarding care, they will contact their medical director, thereby releasing the referral physician from any further liability.
A disadvantage of this type of transport is the length of time it can take for the team to arrive to assume care of the patient. Thal is often the reason that referring hospitals use local transport providers.Prior to using either type of transport team, it is wise for the referral facilities to have full knowledge of exactly what training and experience each team has received for HROB patients and what equipment they use and what treatments they can provide. It is also important that written letters of agreement are made between both the referral and receiving facilities clearly stating each institution’s responsibility to assure compliance with local, state, and federal laws.
TEAM CONFIGURATION
All EMS and transport crew members will eventually be called upon to transport a pregnant medical, trauma, or laboring patient. When this request occurs in the pre-hospital environment, the crews will follow the standing orders of their field medical director.
Transport teams that accept the responsibility of caring for HROB patients must be capable of meeting the needs of the most critical OB and neonatal patients. For transporting HROB patients from one facility to another (interfacility transport), the teams’ training should encompass triage, assessment, stabilization, and decision making regarding how and when to safely move these patients. Suggested
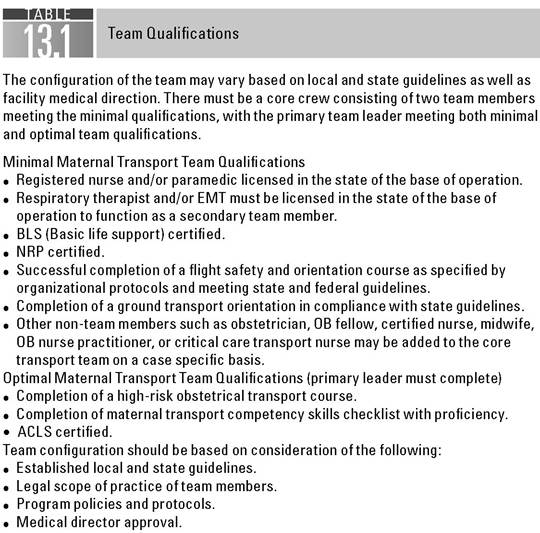
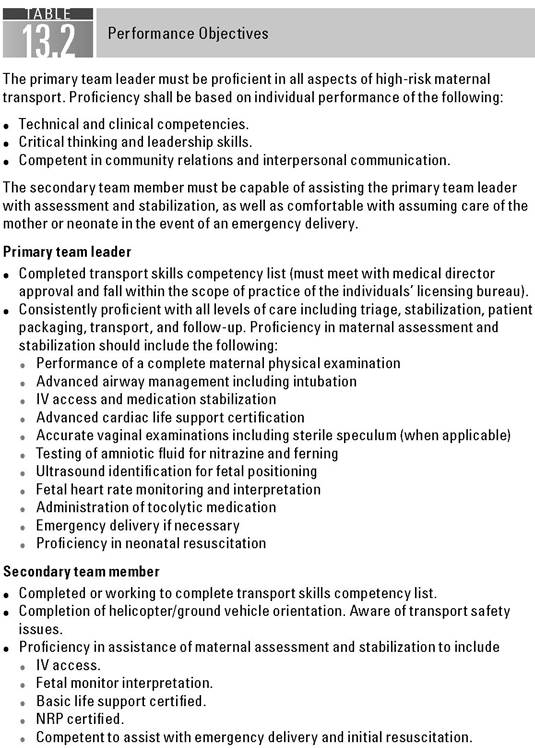
minimal and optimal qualifications for each team member should be considered while keeping in compliance with his or her scope of practice as well as local and state guidelines (Table 13.1). The level of care that team members can provide is then categorized according to their individual performances defining them as either primary or secondary team members (Table 13.2). The team members must have completed or must be in the process of completing the skills competency checklist and should possess complete knowledge and understanding of the standing orders mandated by their institutions’ medical director (Table 13.3) (4).
Beginning with the initial report received, the patient can be placed into a Priority 1, 2, or 3 status based on her acuity (Table 13.4) (4). This priority level is

The items included in the transport competency checklist of each individual program will be based on the program's protocols and medical direction. Primary team members must demonstrate competency in all of the areas listed on the transport checklist. Secondary team members must be working toward completion of competencies for their position on the team.
A. Triage
• Accept verbal report from sending facility.
• Categorize transport according to severity and mode of transport.
• Estimate ETA for referral facility.
• Activate appropriate transport personnel and vehicle.
• Notify medical director, NICU, perinatal center of new admission.
• Prepare appropriate equipment for departure.
B. Vaginal examinations
• Perform vaginal examinations on laboring women in controlled setting with a preceptor. Differentiate between normal and abnormal rate of cervical dilation, effacement, and descent of presenting part.
• Must show competency by consistently demonstrating 90% accuracy when determining dilation, effacement, and station as well as fetal presentation and position.
• Examination competency includes showing proficiency in determining all dilation stages from a closed/thick cervix to complete dilation.
C. Speculum examinations for PROM
• Demonstrate proficiency in proper insertion of speculum.
• Assess color, amount, and odor of the amniotic fluid.
• Visualize cervix to assess dilation when applicable.
• Confirm rupture of membranes with nitrazine or fern test.
D. Ultrasound identification of fetal position
• Proficiency in utilizing ultrasound examination to determine fetal position (in accordance with institutional policy and nurse practice act).
• Confirmation of correct fetal position vital prior to transport.
E. Fetal heart rate monitoring and interpretation
• Completion of basic fetal monitoring course or equivalent.
• Passing of fetal monitoring test with 90% or higher.
• Recognize normal and abnormal fetal heart rate patterns and identify nonreassuring tracings.
• Promptly initiate appropriate nursing interventions for non-reassuring FHR tracings and notify appropriate physician.
• Recognize normal and abnormal contraction patterns.
• Initiate appropriate nursing interventions for abnormal contraction status and notify appropriate physician.
• Apply direct fetal monitoring devices in accordance with nurse practice act, institution policy, and medical direction when necessary
F. Obstetrical pharmacology administration
• Competency validation of medication knowledge including medication desired effect, route, dosage, adverse effect, interactions, and considerations.
• Monitor the mother and the fetus for desired and deleterious effects of administered medications. Prepare for medication discontinuance and reversal if necessary.
G. Medical directing standing orders
• Competency validation of knowledge of standing orders.
• Requesting of further orders from medical direction when completion of standing orders achieved if needed.
Team Education Competency (continued)
H. Equipment
• Competency validation of safe usage of equipment in multiple transport settings.
• Yearly or more frequent equipment updates or in-service.
I. Neonatal resuscitation procedures
• Current neonatal resuscitation procedure—(NRP) certification.
• Advanced procedures—Intubation, UVC insertion, medication administration in accordance with medical direction, institution policy, and nurse practice act.
J. Transport vehicle safety competency
• Safety orientation of ground vehicle or air ambulance to include location of emergency exits, fire extinguishers, securing of self and equipment, life vests and floats, emergency oxygen, survival kits, radio usage and ELT activation for air ambulance.
• Function as air crew member with rotor wing transport using safety instruction such as rotor safety, obstacle watch, participation in take off and landing safety checklist, etc.
• Knowledge and adherence to safety rules for each type of transport vehicle.
• Location of vehicle oxygen, suction, and emergency telecommunication transmitting ability.
The transport coordinator and/or medical director of the transport team shall evaluate the skills and clinical competencies. Methods of evaluation and documentation may include any or all of the following:
• Written examination
• Skills labs
• Case presentations with oral examination
different than that of current trauma criteria where the Priority 1 patient has no vital signs, yet the HROB Priority 1 patient is still the sickest and most acute of the pregnant patients requiring transportation. In some circumstances, the teams may want to reconfigure their team members based on the priority status of the patient and the training level of the team currently in place. This allows for more qualified personnel to be added to, or changed out, based on: patient acuity, possibility of delivery prior to returning to the receiving facility, etc.
TRANSPORT TEAM PRELIMINARY ASSESSMENT
The transport of the HROB patient is very challenging in many aspects (5,6). The team members must appreciate that two patients are being transported. It is imperative to perform an accurate assessment on both patients and begin stabilization efforts prior to moving the patients. The evaluation begins with the initial report received from the referring facility. This report helps both the referring facility and the transport team to determine if additional stabilization techniques should be implemented by the referral physician while the team is en route and allows the team to prepare a preliminary care plan prior to their arrival.
To ensure that the patient report is provided in a clear and concise manner, it is helpful to use a specialized “triage form.” When both the referral facility and the team have a copy of this form, report flow is much smoother and ensures that nothing is forgotten in the process.

Definitions
• Primary team leader—defined as a team member proficient in all aspects of HROB transport (completed transport skills checklist).
• Secondary team leader—defined as a team member who is capable of assisting with the primary team leader with assessment and stabilization as well as comfortable with assuming care of the mother or the neonate in the event of an emergency delivery (working to complete transport skills checklist).
Priority 1 Team Configuration
At least one primary team leader and either a second primary team member or a very skilled secondary team member must accompany all Priority 1 patients.
Examples of Priority 1 Patients
This patient is usually the most severe patient and can become unstable rapidly. Examples of this type of patient include
• Multipara with ruptured or bulging membranes.
• Multipara with >3 cm and regular contraction pattern.
• Primigravida @ 4 cm or greater.
• Preeclampsia, eclampsia, or HELLP syndrome
• Premature labor with regular contraction pattern (Bradycardia—baseline rate of 160 bpm for ≥10 minutes
Variability
Fluctuations in the baseline FHR of two cycles per minute or greater. Visually quantitated as the amplitude of the peak to trough in beats per minute— classified as absent, minimal, moderate, and marked
■ Absent variability—amplitude from peak to trough undetectable.
■ Minimal variability—amplitude from peak to trough more than undetectable and ≤5 bpm.
■ Moderate variability—amplitude from peak to trough 6 to 25 bpm.
■ Marked variability—amplitude from peak to trough >25 bpm.
Acceleration
Visually apparent abrupt increase (onset to peak is dialysis, trauma, drug abuse
■ Surgical complications—trauma, acute abdomen, previous C/S, thoracic emergencies
■ Fetal conditions requiring specialized neonatal treatment upon delivery such as diaphragmatic hernia, omphalocele, neural tube defects, fetal heart dysrhythmias, fetal hydrops, etc.
B. Emergency childbirth
Emergency delivery may be necessary at the referral facility if stabilization attempts are unsuccessful. Emergency childbirth situations may include
■ Breech presentation
■ Shoulder dystocia
■ Umbilical cord prolapse
■ Meconium stained amniotic fluid delivery
■ Prolonged fetal non-reassurance
■ Nuchal cord
■ Potential for delivery in confined spaces in transport
■ Postpartum hemorrhage
■ Uterine inversion
■ Uterine rupture
Preterm Labor (PTL) and/or Preterm Premature Rupture of Membranes (PPROM) Premature births are the number one obstetric problem in the United States. Approximately 70% of all maternal transports are secondary to complications of preterm labor and/or premature rupture of membranes. According to the National Center for Health Statistics, 543,000 babies were born prematurely in the United States in 2006 (9). This is a 36% increase since the1980s. While medical facilities and NICUs have excellent success rates with very premature infants, approximately 12 babies die daily due to prematurity. While organizations such as March of Dimes provide fund-raising and education for the prevention of prematurity, the United States was given a “D” on an overall report card for this condition (9).
Some methods of stabilization of the preterm patient should include (10-12)
■ Prompt identification by rapid assessment of preterm labor patients.
■ Prompt interventions using stabilization techniques beginning with the least invasive and working in a progressive manor:
■ Dehydration can cause contractions that mimic labor
■ Give IVF bolus of 500 to 1,000 mL of LR or NS to a healthy patient with adequate urine outputs (>30 mL per hour) and no underlying disease processes, and repeat prn
■ Ensure patient bladder remains empty; use of Foley Catheter recommended for transport
■ Infection may cause contractions; consider antibiotics following completion of blood draws and cultures dependant on medical direction protocols
■ Avoid repeated vaginal exams unless patient appears more active or c/o urge to have bowel movement or push, especially if already PPROM in which case vaginal exam should be especially avoided
■ Consider starting tocolytics immediately coinciding with the IV fluid bolus. Although there is controversy with regard to continuing using these tocolytics once at the receiving facility, most transport teams and receiving physicians will agree that having the ability to administer rapid-acting tocolytics during transport is a huge benefit in getting the patient from point A to point B.
■ Tocolytics
• Brethine (Terbutaline Sulfate)—a β-sympathomimetic. Decreases smooth muscle contractility, resulting in uterine and bronchial relaxation
Dosage—0.25 mg SQ—may repeat every 20 minutes for three doses
Side effects—tremors, light-headedness, flushed feeling, restlessness, maternal and fetal tachycardia, palpitations, nausea and vomiting
Contraindications—hold for maternal pulse >120 bpm. Active bleeding, insulin-dependent diabetes, cardiac or chronic HTN
Is one of three drugs that when used together can increase chances of pulmonary edema (MgSO4 and steroids are the other two)
• Magnesium sulfate (MgSO4)—relaxes smooth muscle of uterus by substituting itself for calcium. Often first-line drug for PTL/ PPROM and HTN. Is a smooth muscle relaxer used to relax the uterus.
Loading dose: 4 to 6g loading dose over 30 minutes (unless contraindicated—lower dose with decreased renal clearance). Administered IVPB only, never mainlined. Never give IM.
Maintenance dose: 1 to 4 g per hour
Therapeutic level: 4 to 7 mEq/L
Side effects—flushing, sweating, nausea and vomiting, drowsiness. Lower doses should be given in renal impairment or decreased urine output/preeclamptic patients. Must maintain urine output >30 mL per hour to prevent possible toxicity as MgSO4 is excreted through urine
Frequent assessment of vitals, pulse ox, DTRs, lung sounds
Toxicity: weakness, visual disturbances, general muscle relaxation, loss of DTRs, respirations or advanced expertise including surgical intervention will determine if and when the patient should be moved
■ Air versus ground (pros and cons) (11-14)
■ Air: pro—rapid response to patient and rapid return to receiving facility
■ Air: con—weather, patient fear of flight, too confined a space for some HROBs
■ Ground: pro—more room for reconfiguring team to include taking additional staff, ability to transport isolette and mother together in some instances
■ Ground: con—vibrations in ambulance are adverse for many OB patients especially advanced dilation or bulging amniotic sac, traffic delays, slower response to patient, and return of patient
■ Care and considerations en route (13,14)
■ Patient positioning in vehicle (Trendelenberg, lateral, knee-chest)
■ Is position providing maximal uterine perfusion?
■ Can both ends of the patient be accessed (head and abdominal area)?
■ Is the facility equipped for emergency delivery/neonatal resuscitation?
■ Prepare to give additional tocolytics en route
■ Consider premedicating all HROB with antinausea, antianxiety medications to prevent nausea/vomiting secondary to medications and motion sickness
■ Fetal and uterine surveillance en route
■ Continuous fetal and uterine monitoring preferable
■ Consider inability to note FHR due to noise
■ Consider inability to palpate uterine contractions in moving vehicle
■ Consider ignoring surveillance as breach of standard of care
■ When to say NO to maternal transport
■ Sometimes safer to assist referring facility than move the patient
■ Active and advanced labor—is it an EMTALA violation?
■ Maternal hemorrhage, severe hypotension, shock
■ Fetal compromise with repetitive late decelerations, non-reassuring FHR tracings
■ Ensure the referral physician understands possible need to keep the patient
LEGAL CONSIDERATIONS
The transfer of a pregnant patient from one facility to another raises some medicolegal considerations. The largest area of concern is the liability issue of who assumes patient responsibility during the transport. Prior to any transfer, the risks and benefits of the transport should be discussed with the patient and the family as well as documented extensively. According to the COBRA laws, the referral physician must discuss the patient status with the receiving physician, who then accepts the patient transfer (15,16). Evaluation and stabilization of the patient should be performed prior to moving the patient to ensure that no harm will come to the patient as a result of the transfer and that the benefits of transfer clearly outweigh the risks (14,17).
It is important that both the referral and the receiving facilities understand that not all transport teams are created equally with regard to obstetric transport knowledge and expertise. According to a 2001 article in the AirMedicalJournal, 203 air medical transport programs were surveyed, with 133 programs responding to a series of questions regarding the air medical transport of HROB patients. It was concluded that “many programs appeared poorly prepared for these patients” (HROB). This study also showed that only 52% of the programs required their staff to have neonatal resuscitation certifications (18). There is NO universally mandated training required for teams who perform maternal transport, regardless of whether they are a local ambulance called for a one-way transport or a team sent from a receiving facility providing a two-way transport.
While there has been some discussion amongst specialty transport organizations to develop suggested maternal transport guidelines or protocols, none have been adopted as of yet. This leaves it up to the individual transport agencies to decide what, if any, type of training they wish for their employees to have. Some transport team administrators feel that OB transports are a low-volume type of transport (overall 2006, released January 7, 2009.
10. Management of Preterm Labor. ACOG Practice Bulletin. Number 43, May 2003.
11. Nelson M. The high-risk obstetric patient. In: Air Medical Crew Core Curriculum. Pasadena, CA: US Department of Transportation; 1988:177-190.
12. AAMS. Guidelinesfor Air Medical Crew Education Dubuque, IA: Kendall Hunt Publishing; 2004.
13. National Flight Nurses Association, Flight Nursing Core Curriculum. “Obstetrical Transport” Chapter 16 & “Neonatal Transport” Chapter 17; 1997.
14. Lee G. Flight Nursing principles and practice. 1st Ed. St. Louis, MO: Mosby; 1991.
15. Cady R., Rostant D. Liability Issues in Perinatal Nursing. Washington, DC: AWHONN; 1999.
16. Frew SA, Roush WR, LaGreca, K. COBRA: implications for emergency medicine. Ann Emerg Med 1988;17:835.
17. Mandeville L., Troiano, N. High-risk & Critical Care Intrapartum Nursing. 2nd Ed. Philadelphia, PA: J.B. Lippincott; 1999.
18. Jones AE, Summers RL, Deschamp C, Galli RL. A national survey of the air medical transport of high-risk obstetric patients. AirMedJ. 2001;20(2):17-20.