Delivery in the Emergency Department
Isaac Delke
In the United States, 99% of all births have been in hospitals over the past several decades (1). In many areas, the emergency department (ED) is where the obstetric patient enters the hospital.
These patients are subsequently sent to the labor and delivery suite if the hospital has an obstetric service. Sometimes, however, emergency medical system (EMS) personnel and/or ED staff are faced with a gravida ready to deliver, and they must be prepared to handle such a situation. The apprehension experienced by emergency birth attendants is not simply due to the lack of expertise with normal deliveries but also is due to the awareness of the potential for serious maternal and perinatal complications.This chapter presents basic steps in the management of imminent delivery. It focuses on (i) EMS preparedness, (ii) normal spontaneous vaginal delivery, and (iii) complications of vaginal delivery (shoulder dystocia, breech presentation, cord prolapse, and postpartum hemorrhage and/or perineal lacerations). Preparedness and knowledge of the management of obstetric emergencies that commonly confront the ED staff maximize the potential for effective intervention and optimal outcome.
EMS PREPAREDNESS
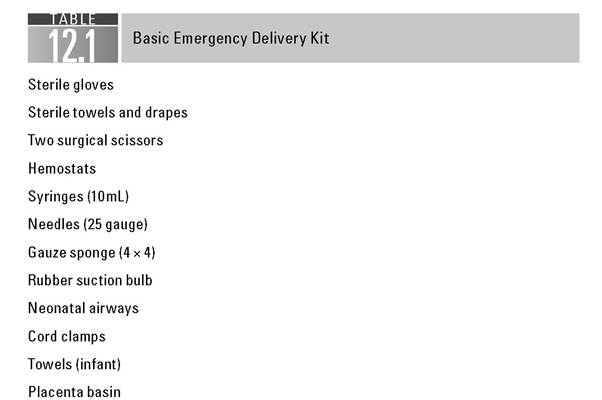
EMS personnel must be trained to recognize and manage precipitate delivery appropriately. This requires knowledge by EMS personnel of available obstetric and neonatal units in the system’s catchment area for appropriate transport. The transport team should be trained to assist in the precipitate delivery of an infant and skilled in the use of basic obstetrical kits. Prehospital protocols should be reviewed often so that EMS personnel remain prepared for the rare and potentially catastrophic pregnancy-related events. Whether patients deliver in the prehospital setting or on immediate arrival to the ED, every ED should be ready for emergency delivery by preparing a basic delivery kit, along with resources for the initial care and potential resuscitation of the newborn (Table 12.1).
Because of the relatively infrequent delivery in the prehospital setting or ED, extra care should be taken to educate EMS and ED personnel through educational programs, annual in-services, and equipment orientation sessions.Spontaneous vaginal delivery
The initial step in the management of a woman in active labor is to obtain vital signs and initiate supportive therapy, including obtaining venous access and monitoring the mother and fetus. Pelvic examination should reveal fetal presentation, including visible or palpable head or, in the case of breech presentation, the fetal buttock or extremity. Sometimes, confirmation of fetal cardiac activity and presentation may be accomplished using portal ultrasound. The stage of labor and the parity of the patient should be taken into account when considering transport of a patient in labor to another facility or to the labor and delivery suite.
Delivery of the Head
If delivery of the head is already well on its way, the attending physician should prepare for the delivery after a stat call to obstetric and pediatrician staff. Ideally, the patient should be on the delivery table in the lithotomy position. If the patient is on a bed or stretcher, her legs should be supported. As time allows, the perineum may then be prepared by washing with mild soap and water and swabbing with povidone-iodine or chlorhexidine topical solution. Drapes should be placed over the patient, and the birth attendant should use gowns, masks, and gloves. The mother should be informed, assured, and instructed to enhance maternal cooperation to accomplish a controlled delivery. If the fetus is dead, there is no risk of further fetal trauma, and focus is totally on the mother.
The Ritgen Maneuver
As the head becomes increasingly visible, the vaginal outlet and vulva are stretched until they ultimately encircle the largest diameter of the baby’s head (crowning).
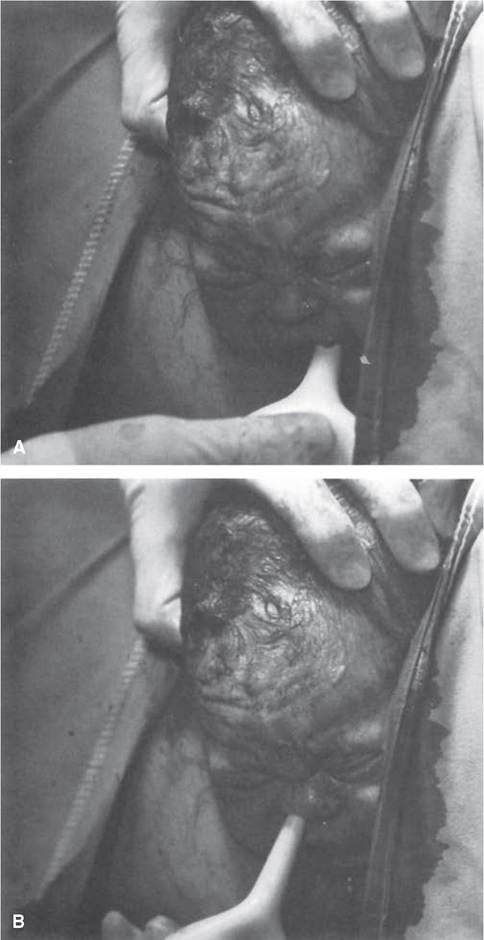
As the infant’s head emerges from the introitus, the perineum should be supported by placing a sterile towel along the inferior portion of the perineum. Forward pressure should be extended on the chin of the fetus through the perineum just in front of the coccyx, while the other hand exerts mild counterpressure superiorly against the occiput to prevent rapid expulsion of the fetal head, which may lead to perineal or periurethral tears (Fig. 12.1). It also favors extension of the head, so that delivery occurs with its smallest diameters passing through the introitus and over the perineum. The head is delivered slowly, with the base of the occiput rotating around the lower margin of the symphysis pubis as a fulcrum, while the bregma (anterior fontanel), brow, and face pass successively over the perineum (2,3). The mother is then asked to breathe through contractions rather than bearing down and attempting to push the baby out rapidly.The use of routine episiotomy for a normal spontaneous vaginal delivery has been discouraged in recent years, because it has been demonstrated to

FIGURE 12.1 The Ritgen maneuver.
increase the incidence of third- and fourth-degree perineal lacerations occurring at the time of delivery. If an episiotomy is necessary, it may be performed as follows: 5 to 10 mL of 1% lidocaine solution is injected with a 25-gauge needle into the posterior fourchette and perineum. While protecting the fetal head, a 2 to 3 cm midline cut is made with scissors to extend the vaginal opening. The incision must be supported with manual pressure from below, taking care not to allow the incision to extend into the rectum.
Delivery of the Shoulders
After delivery of the head, the occiput promptly turns toward one of the maternal thighs, so that the head assumes a transverse position. The successive movements of restitution and external rotation indicate that the bisacromial diameter (transverse diameter of the thorax) has rotated into the anteroposterior diameter of the pelvis.
The anterior shoulder should then be delivered by gentle downward traction in concert with maternal expulsive efforts. Traction should be exerted only in the direction of the long axis of the infant, because, if applied obliquely, it causes bending of the neck and excessive stretching of the brachial plexus. The posterior shoulder is then delivered by upward traction. Some practitioners, including the author, prefer to deliver the anterior shoulder prior to its external rotation (head-and-shoulder delivery) to avoid potential shoulder dystocia. The rest of the body almost always follows the shoulders without difficulty. A point of practical concern is the need to maintain control of the newly born infant such that inadvertent dropping does not occur.Clearing the Nasopharynx
To minimize the likelihood of aspiration of amniotic fluid debris, meconium, and blood that might occur once the thorax is delivered and the infant can inspire, the face is quickly wiped and the nares and mouth are aspirated (Fig. 12.2). A soft rubber ear syringe or its equivalent, inserted with care, is suitable for this purpose.
Nuchal Cord
After delivery of the head and anterior shoulder, check for a nuchal cord by passing a finger around the fetal neck. A nuchal cord occurs in about 25% of cases and ordinarily does no harm. If a cord is felt, it should be drawn down between the fingers and, if loose enough, slipped over the infant’s head. If it is applied too tightly to the neck to be slipped over the head, it should be cut between two clamps only after delivery of the anterior shoulder and the infant should be delivered promptly.
Clamping the Cord
The timing of cord clamping should be dictated by convenience, and cord clamping is usually performed immediately after delivery of infant. The cord is clamped after thoroughly clearing the infant’s airway, which usually takes about 30 seconds. The infant is not elevated above the introitus at vaginal delivery. The umbilical cord is cut between two clamps placed 4 or 5 cm from the fetal abdomen.
Later, an umbilical cord clamp is applied 2 or 3 cm from the fetal abdomen. A segment of the umbilical cord is saved for blood gas analysis.Delivery of the Placenta
The placenta should be allowed to separate spontaneously. Immediately after delivery of the infant, the height of the uterine fundus and its consistency are ascertained. As long as the uterus remains firm and there is no unusual bleeding, the usual practice is to watch carefully for any of the following signs of placental separation.
1. The uterus becomes globular and firm. This sign is the earliest to appear.
2. There is often a sudden gush of blood.
3. The uterus rises in the abdomen because the placenta, having separated, passes into the lower uterine segment and vagina, where its bulk pushes the uterus upward.
4. The umbilical cord protrudes farther out of the vagina, indicating that the placenta has descended.
These signs usually appear within 5 minutes. The mother may be asked to bear down, and the intra-abdominal pressure so produced may be adequate to expel the placenta. If these efforts fail, the attendant, again having made certain that the uterus is contracted firmly, lifts the fundus cephalad with the abdominal hand, keeping the umbilical cord slightly taut (Brandt-Andrews method). Aggressive traction on the cord risks uterine inversion, tearing of the cord, or disruption of the placenta, which can result in severe vaginal bleeding (2,3). As the placenta passes through the introitus, pressure on the uterus is stopped. The placenta is then gently lifted away from the introitus. Care is taken to prevent the membranes from being torn off and left behind. If the membranes start to tear, they are grasped with a ring forceps and removed by gentle traction. After removal of the placenta, the uterus should be massaged gently to promote contraction. The placenta, membranes, and umbilical cord should be examined for
abnormalities of cord insertion, confirmation of a three-vessel cord, and completeness of removal of placenta and membranes.
Oxytocin Agents
After delivery of the placenta, the primary mechanism by which hemostasis is achieved at the placental site is by a well-contracted myometrium. Oxytocin (Pitocin, Syntocinon, etc.), ergonovine maleate (Ergotrate), methylergonovine maleate (Methergine), and misoprostol (Cytotec) are used in various ways in the conduct of the third stage of labor, principally to stimulate myometrial contractions and thereby reduce the blood loss (Table 12.2).
Oxytocin, ergonovine, methylergonovine, and misoprostol are all used widely in the conduct of the normal third stage of labor, but the timing of their administration differs at various institutions. Oxytocin, and especially ergonovine, given before delivery of the placenta will decrease blood loss somewhat. However, the use of oxytocin, and especially ergonovine or methylergonovine, before delivery of the placenta may entrap an undiagnosed, and therefore undelivered, second twin. This may prove injurious, if not fatal, to the entrapped fetus. In most cases following uncomplicated vaginal delivery, the third stage of labor can be conducted with reasonably little blood loss.
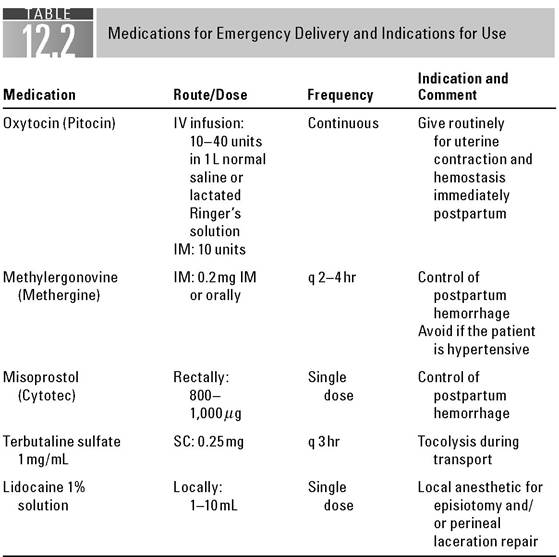
IM, intramuscular; IV, intravenous; SC, subcutaneous.
If an intravenous (IV) access has been established, oxytocin 10 to 20 units in 500mL normal saline, already premixed, is administered after delivery of the placenta at a rate of 10 mL per minute for a few minutes, until the uterus remains firmly contracted and the bleeding is controlled. Then the infusion rate is reduced to 2 mL per minute until the mother is ready for transfer from ED to the labor and delivery suite or the postpartum unit. In instances where there is no IV access, oxytocin can also be given as 10 units intramuscularly. The use of nipple stimulation in the third stage of labor also has been shown to increase uterine pressures and to decrease the duration of the third stage of labor and blood loss (2,3).
Infant Care
Once the cord has been divided, the infant is immediately placed supine with the head lowered and turned to the side in a heated unit that has appropriate thermal regulation.
After delivery, the infant should be held securely or placed on the mother’s abdomen and wiped dry, while any mucus remaining in the airway is suctioned. The infant’s clinical status should be assessed at 1 and 5 minutes after delivery. In the setting of an uncomplicated delivery, the mother may hold the child immediately while the cord is being cut, provided that the child has responded well to initial stimulation and has a clear airway and good respiratory effort (2,3).
Breastfeeding
If both mother and baby are stable and no medical contraindications exist, breastfeeding should be encouraged as soon as possible after birth. Benefits include promotion of uterine contractions that control hemorrhage at the placental insertion site, encouragement of maternal-newborn bonding, provision of easily digestible and balanced nutritional support for the baby, and transmission of antibodies (immunoglobulin A) that protect the enteric mucosa against invasion by colonizing bacteria.
COMPLICATIONS OF EMERGENCY VAGINAL DELIVERY
Shoulder Dystocia
Shoulder dystocia is an obstetric emergency that can lead to significant neonatal morbidity (brachial plexus injury, fractured humerus or clavicle, etc.) and mortality (severe asphyxia), if not managed appropriately. The major maternal consequence of shoulder dystocia is postpartum hemorrhage, usually from uterine atony but also from vaginal and cervical lacerations.
Shoulder dystocia is first recognized after delivery of the fetal head, when gentle downward traction is insufficient to deliver the anterior shoulder. After delivering the infant’s head, it retracts tightly against the perineum (the turtle sign). Shoulder dystocia is the impaction of fetal shoulders at the pelvic outlet after delivery of the head. Typically, the anterior shoulder is trapped behind the pubic symphysis, leading to a delay of delivery of the rest of the infant. It usually occurs in the delivery of larger infants with disproportionately large shoulders compared with the fetal head. Shoulder dystocia also occurs with an extremely rapid delivery of the head, or as a result of Pverzealous external rotation of the fetal head by the birth attendant. Shoulder dystocia cannot be predicted from clinical characteristics or labor abnormalities.
The reported incidence varies from 0.2% to 3.0% of all vaginal deliveries. The lack of uniformly accepted definition or criteria for the diagnosis of shoulder dystocia contributes to its varying incidences (4,5).
Various maneuvers have been described to free the anterior shoulder from its impacted position beneath the maternal symphysis pubis. Unfortunately, there is no one superior algorithm to manage shoulder dystocia. The specific maneuver used is probably not as critical as a careful, quick, and organized action to relieve the shoulder dystocia and avoid desperate and potentially traumatic traction of the fetal head.
Management
Key Management Points: A previously uncompromised fetus/infant may be able to withstand 5 to 7 minutes of shoulder dystocia without suffering permanent injury from lack of oxygen (5). Once you recognize shoulder dystocia:
■ Call for help: obstetric, pediatric, and anesthesia teams.
■ Designate a care-team member as a timekeeper. Tracking the time is necessary both to allow periodic reassessment of the situation in case of severe shoulder dystocia and for documentation after delivery.
■ Inform patient/family as to why certain actions are being taken— communication points:
■ “The baby' s shoulders are stuck”
■ “I’m going to need to focus on getting the baby out”
■ “I may need to ask for your help”
■ Empty the patient’s bladder.
■ McRoberts position plus suprapubic pressure.
■ Delivery of the posterior arm after an episiotomy.
■ Rotational maneuvers: Woods/Rubin.
■ All-fours position (Gaskin maneuver).
■ Fracture clavicle.
■ Zavanelli maneuver.
■ Abdominal rescue.
The most popular techniques include the following:
1. McRoberts Position and Suprapubic Pressure. This consists of sharply flexing the woman’s legs on her own abdomen (Fig. 12.3). This has been
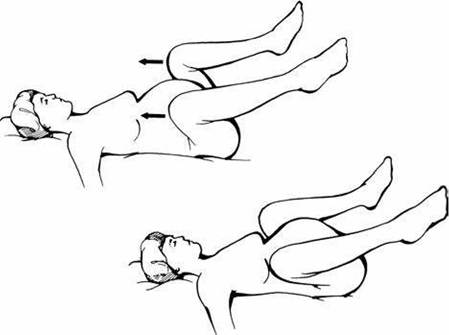
FIGURE 12.3 The McRoberts position.
shown to straighten the sacrum relative to the lumbar vertebrae, with accompanying rotation of the symphysis pubis toward the patient’s head and a decrease in the angle of pelvic inclination. This position does not increase the dimensions of the pelvis, but the cephalic rotation of the pelvis frees the impacted anterior shoulder. The bladder should be drained if this has not been done already. Then, moderate suprapubic pressure is applied obliquely by an assistant while downward traction is applied to the fetal head by the attendant. The success rate of McRoberts position in resolving shoulder dystocia, used either alone or in combination with suprapubic pressure, is reported between 42% and 58% (5).
2. Delivery of the Posterior Arm. If McRoberts position and suprapubic pressure fail to effect delivery, attempt to deliver the posterior arm. Posterior arm extraction, when successful, will replace the bisacromial diameter with the axilloacromial diameter, thereby reducing the obstructing diameter in the pelvis. Insert a hand along the posterior shoulder, grasp and flex the forearm at the elbow, sweep it across the chest, and bring it through the vagina. It is usually easy to do this using your hand that is opposite the fetal face. The mother should not be pushing during this maneuver.
If the head is tightly retracted against the maternal perineum, it may be necessary to perform episiotomy or proctoepisiotomy in order to insert your hand into the vagina to deliver the posterior arm.
After delivery of the posterior arm, gentle downward traction on the fetal head will usually result in delivery of the anterior shoulder and the baby. If delivery of the anterior shoulder and baby cannot be accomplished, perform rotation of the posterior shoulder 180 degrees to the anterior position. If the fetus is facing the mother’s right side, rotation should be attempted in a counterclockwise direction as a first step. Some birth attendants prefer to attempt rotational maneuvers before attempting to deliver the posterior arm. Two types of rotational maneuvers are generally attempted.
3. Rotational Maneuvers: Woods Corkscrew and Rubin Maneuvers. The Woods corkscrew maneuver is rotating the fetal posterior shoulder by placing your index and middle fingers on the ventral surface (that facing the fetal face) and rotating the entire fetal body. If the fetus is facing the mother’s right side, this would be accomplished with your left hand and rotation would be in a counterclockwise direction. Often after a 90-degree rotation, it will be necessary to replace your left hand with your right hand to complete a 180-degree rotation.
The first Rubin maneuver is accomplished by rotating the anterior shoulder under the symphysis pubis. If the fetus is facing the mother’s right side, you would use your right hand to perform this maneuver. The second Rubin maneuver is rotating the posterior shoulder in a clockwise direction by placing pressure on the dorsal surface of the posterior shoulder.
If neither delivery of the arm nor rotational maneuver is possible, bilateral shoulder dystocia may be present, in which the anterior shoulder is lodged behind the symphysis pubis and the posterior shoulder is lodged high in the pelvis at or near the sacral promontory. In this case, "all-fours" position (Gaskin maneuver) could be attempted.
4. All-Fours Position (Gaskin Maneuver). The mother is now positioned on her hands and knees. This allows rotation of the maternal pelvis with disim- paction of the anterior shoulder under the symphysis. This position exploits the effects of gravity and increased space in the hollow of the sacrum to facilitate delivery of the posterior shoulder and arm. An attempt is now made to deliver the posterior shoulder by gentle downward traction followed by delivery of the anterior shoulder by gentle upward traction. If this is not successful, an attempt can be made to deliver the posterior arm as described above. If the mother cannot assume the “all-fours” position or delivery cannot be accomplished in this position, deliberate fracture of the clavicle, cephalic replacement and cesarean delivery, or abdominal rescue may be necessary in rare cases.
5. Deliberate Fracture of the Clavicle. The anterior clavicle is deliberately fractured by pressing against the ramus of the pubis so that the shoulder is freed of impaction. The fracture heals rapidly and is not nearly as serious as a brachial nerve injury, asphyxia, or death.
6. The Zavanelli Maneuver (Cephalic Replacement). The first part of this maneuver consists of returning the head to the occipitoanterior or occip- itoposterior position. If the head has rotated from either position, the second step is to flex the head and slowly push it back into the vagina. Once the fetal head is reintroduced into the vagina, emergency cesarean delivery should be performed. A fetal heart should be documented, if at all possible, before performing cesarean delivery.
7. Abdominal Rescue. If all maneuvers have been attempted and you are unable to replace the fetal head, low transverse uterine incision can be performed, the anterior shoulder manually rotated into the oblique diameter by the surgeon, and vaginal delivery performed by the birth attendant.
Maneuvers to Avoid
■ Avoid aggressive fundal pressure, because it may further worsen the impaction of the shoulder and also may result in uterine rupture.
■ Any nuchal cord, if unable to be reduced over the fetal head, should not be clamped and cut until delivery of the anterior shoulder, if at all possible.
Breech Presentation
Vaginal breech deliveries are associated with a morbidity rate three to four times greater than that of cephalad presentations. Risks to the fetus inherent in vaginal breech delivery include (i) prolapse of the umbilical cord, (ii) entrapment of the aftercoming head by the incompletely dilated cervix, and (iii) trauma resulting from extension of the head or nuchal position of the arms (6,7).
A major current dilemma is that of obtaining sufficient experience at vaginal breech delivery. Little or minimal experience is gained in many training programs. Thus, many recently trained obstetricians may have great difficulty when faced with imminent vaginal breech delivery at a facility unable to perform an emergency cesarean delivery.
Management
1. The patient who enters the ED with a breech presentation with buttocks crowning or legs showing through the introitus requires rapid mobilization of personnel for delivery.
2. Generally, there is time for transfer to the labor and delivery suite. Give 0.25 mg subcutaneous terbutaline to inhibit uterine activity before transfer of the patient.
3. Call for an obstetrician, a nurse assistant, a pediatrician, and anesthesia personnel. If possible, a quick ultrasound (portal) examination to determine the presence of fetal cardiac activity, fetal head, its attitude, and possible hydrocephaly would be ideal and helpful in the management decision. If the fetus is dead, there is no risk of further fetal trauma, and concern is totally for the mother.
4. If a leg is presenting at the vaginal introitus, it should not be pulled down because the patient may not be ready to deliver. This may be a footling presentation through a cervix that is not fully dilated. There is time to transfer the patient to the labor and delivery unit, preferably in the knee-chest position to avoid possible cord compression.
5. Avoid artificial rupture of membranes (AROM) in breech presentations. As the amniotic sac balloons into the birth canal, it helps to dilate the cervix completely. This facilitates descent of the baby, providing a lubricated smooth surface against which the body can freely move, and cushions the umbilical cord against compression in the birth canal.
6. If the fetus is already delivered to the umbilicus, the attendant should wrap the fetal trunk with a towel to provide support to the body while further descent results from expulsive forces from the mother only.
7. Delivery of the aftercoming head: The index and middle fingers of one hand are applied over the maxilla (not mandible) to flex the head, while the fetal body rests on the palm of the hand and forearm. The forearm is straddled by the fetal legs. Two fingers of the other hand then are hooked over the fetal neck, and grasping the shoulders, downward traction is applied until the suboccipital region appears under the symphysis. Gentle suprapubic pressure simultaneously applied by an assistant helps keep the head flexed (Fig. 12.4). The body then is elevated toward the maternal abdomen, and the mouth, nose, brow, and eventually the occiput emerge successively over the perineum.
8. Entrapment of the aftercoming head: Occasionally, especially with small preterm fetuses, the incompletely dilated cervix will not allow delivery of the aftercoming head. With gentle traction on the fetal body, the cervix, at times, may be manually slipped over the occiput. If this is not successful, then Duhrssen incisions (incisions of the cervix at 2 and 10 o’clock positions) are usually necessary. Another option is replacement of the fetus high into the vagina and uterus, followed by cesarean delivery.
Umbilical Cord Prolapse
The reported incidence of umbilical cord prolapse (UCP) varies between 0.2% and 0.6% of births. The major etiologic categories of UCP are (i) fetal malpresen- tation (50%), (ii) preterm labor (30% to 50%), and (iii) AROM (10% to 15%) (7).
Management
■ In the event that vaginal examination reveals palpable, pulsating cord alongside the presenting part or in the cervix or vagina, the examiner’s hand should not be removed but rather should be used to elevate the presenting fetal part to reduce compression on the cord. Call for obstetric, pediatric, and anesthesia personnel.
■ Cesarean delivery is the treatment of choice in almost all cases if there is fetal cardiac activity.
■ Fetal cardiac activity should be confirmed by portal ultrasound rather than cord palpation only.
■ Give terbutaline 0.25 mg subcutaneously to inhibit uterine activity.
■ Transfer the patient to the labor and delivery unit or operating room in Trendelenburg or the knee-chest position, and the presenting part should be manually elevated as far out of the pelvis as possible and held there until delivery is accomplished.

FIGURE 12.4 Delivery of the aftercoming head by flexion.
Neonatal Resuscitation
■ Dry the baby thoroughly, keep the baby warm, and clear the nose and mouth of excess fluid.
■ Assess the respiratory effort and heart rate (by auscultation or palpation at the base of the umbilical cord).
■ Keep the baby warm and observe if the baby is breathing spontaneously with a pulse rate >100 beats per minute.
■ Improve ventilation if the pulse falls below 100 beats per minute and the respiratory effort is poor.
■ Ventilatory support: If stimulation of the baby by rubbing with a towel or flicking the heels fails to elicit improvement in respiratory effort and pulse, apply positive-pressure ventilation with a neonatal mask and Ambu bag (preferably with oxygen).
■ Assess the infant for any bony (fracture of clavicle or humerus) and/or brachial plexus injury.
Postpartum Hemorrhage
Hemorrhage is one of the leading causes of maternal death in women delivering after 20 weeks’ gestation. Postpartum hemorrhage is caused by uterine atony, genital tract lacerations, or retained placenta. Uterine atony or genital tract lacerations may follow an emergency delivery and may lead to excessive vaginal bleeding (8,9).
Management
■ Transfer the patient to the labor and delivery unit for management of the third stage of labor.
■ Medical management pertains primarily to the treatment of uterine atony. Many clinicians utilize a prophylactic infusion of oxytocin consisting of 10 to 20 units of oxytocin in 1,000mL of normal saline or Ringer’s lactate administered at 10 to 20 mL per minute to prevent uterine atony (Table 12.2).
■ If the signs of placental separation have appeared, expression of the placenta should be attempted by manual pressure on the fundus of the uterus. If bleeding continues, manual removal of the placenta is mandatory.
■ In the presence of any external hemorrhage during the third stage, the uterus should be massaged if it is not firmly contracted.
■ Oxytocin is the first-line agent. Additional oxytocin may be administered, as well as methylergonovine 0.2 mg intramuscular (IM) (not IV), or misoprostol 800 to 1,000 μg per rectum. With significant postpartum hemorrhage, vigorous bimanual massage should be continued while administering contractile agents (Table 12.2).
■ The hour immediately following delivery of the placenta is critical. Even though oxytocics are administered, postpartum hemorrhage as the result of uterine relaxation is most likely to occur at this time. It is mandatory that the uterus be evaluated frequently throughout this period by a competent attendant who places a hand frequently on the fundus and massages it at the slightest sign of relaxation. At the same time, the vaginal and perineal regions are also inspected frequently to allow prompt identification of any excessive bleeding.
Lacerations of the Genital Tract
■ Lacerations to the perineum occur commonly following a rapid, uncontrolled expulsion of the fetal head. Perineal lacerations due to birth trauma are categorized into four groups. First-degree lacerations are limited to the mucosa, skin, and superficial subcutaneous and submucosal tissues. Second-degree lacerations penetrate deeper into the superficial fascia and transverse perineal musculature. In addition to these structures, a third-degree laceration disrupts the anal sphincter, whereas a fourth-degree laceration extends into the rectal lumen (2,3,9).
■ After delivery of the placenta, the cervix, vagina, and perineum should be carefully examined for evidence of lacerations. Perineal injuries, either spontaneous or with episiotomy, are the most common complications of spontaneous vaginal deliveries.
■ Perineal laceration repair fundamentally involves the sequential anatomic reapproximation, using absorbable suture material, of the rectal mucosa, anal sphincter, transverse perineal musculature, vaginal mucosa, and skin. In precipitate ED deliveries, the repair of the episiotomy and/or perineal lacerations can often be performed by the obstetric staff, the details of repair being beyond the scope of this book (3).
SUMMARY
Management of spontaneous vaginal delivery is an essential skill for EMS and ED personnel, particularly in settings where obstetric staff is not immediately available. Protocol or guidelines should therefore be in place and should include provisions for the availability of appropriate equipment, medications, trained support personnel, necessary forms for documentation, and universal precaution material (masks, gowns, gloves, goggles, wall suction, etc.) needed for the prevention of human immunodeficiency virus and hepatitis B virus transmission.
Key factors for successful management of emergent vaginal delivery and its complications include constant preparedness, a team approach, and appropriate documentation.
DOCUMENTATION
■ Clear documentation in the chart of the exact events that have taken place during delivery of an infant after shoulder dystocia, breech presentation, or cord prolapse is essential. If the infant has suffered permanent birth injury, there is a high likelihood of malpractice litigation. The best defense can be mounted if there is a clearly documented description of the efforts made to deliver thefetus.
■ The events of the delivery must be documented by all care-team members involved.
Postdelivery Note
■ Type of delivery
■ Position of the fetal head on restitution (e.g., facing the mother’s right or left thigh)
■ Description, sequence, and result of maneuvers used to relieve shoulder dystocia; delivery of the aftercoming head in breech presentation; and management of cord prolapse
■ Delivery date/time
■ Time elapsed from diagnosis to delivery
■ Complete umbilical cord blood gases
■ Condition of the infant with particular attention to Apgar scores and signs of bony and/or brachial plexus injury
■ Information provided to the patient/family members
References
1. Martin JA, Kung H-C, Mathewsa TJ, et al. Annual summary of vital statistics: 2006. Pediatrics. 2008;121:788-801.
2. Cunningham FG, Leveno KL, Bloom SL, Hauth JC, Gilstrap LC III, Wenstrom KD. Conduct of normal labor and delivery. In: Cunningham FG, Leveno KL, Bloom SL, Hauth JC, Gilstrap LC III, Wenstrom kD, eds. Williams Obstetrics. 22nd Ed. New York, NY: McGraw-Hill; 2005:429-434.
3. Kilpatrick S, Garrison E. Normal labor and delivery. In: Gabbe SG, Niebyl JR, Simpson JL, eds. Obstetrics: Normal and Problem Pregnancies. 5th Ed. New York, NY: Churchhill Livingstone Elsevier; 2007:317-319.
4. Benedetti TJ. Shoulder dystocia. In: Queenan JT, Hobbins JC, Spong CY, eds. Protocols for High-Risk Pregnancies. 4th Ed. Malden, MA: Blackwell Publishing; 2005:565-569.
5. Gottlieb AG, Galan HL. Shoulder dystocia: an update. Obstet Gynecol Clin North Am. 2007;34:501-531.
6. Lanni SM, SeedsJW. Malpresentations. In: Gabbe SG, NiebylJR, SimpsonJL, eds. Obstetrics: Normal and Problem Pregnancies. 5th Ed. New York, NY: Churchhill Livingstone Elsevier; 2007:436-446.
7. Klatt TE, Cruikshank DP. Breech, other malpresentations and umbilical cord complications. In: Gibbs RS, Karlan BY, Haney AF, Nygaard I, eds. Danforths Obstetrics and Gynecology. 10th Ed. Philadelphia, pA: Lippincott Williams & Wilkins; 2008: 413-414.
8. American College of Obstetricians and Gynecologists. Postpartum hemorrhage. Practice Bulletin No. 76. Obstet Gynecol. 2006;108:1039-1048.
9. Gilstrap LC, Yeomans ER. Complications of delivery. In: Gibbs RS, Karlan BY, Haney AF, Nygaard I, eds. Danforths Obstetrics and Gynecology. 10th Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:452-458.