Mosquito-Borne Illnesses: Western Nile Virus
Carlos Torres, Allison H. Luper, and C. David Adair
West Nile virus (WNV) is a mosquito borne single-stranded RNA flavivirus, which targets the human nervous system, and can generate viral infections ranging in severity from a mild flu-like presentation known as West Nile fever (WNF) up to an acute neuroinvasive form of illness known as West Nile meningoencephalitis (WNME).
For those infected, cases of WNV generally remain clinically unapparent or present mild flu-like symptoms subsiding before treatment is ever sought. For patients who do require treatment, options are limited, as neither a vaccine nor direct treatment has been fully devised to combat human cases of WNV; the only means of decreasing the morbidity and the mortality of the disease remains mosquito management and avoidance. For this reason, careful planning is necessary especially in the case of immunocompromised individuals, who are at greater risk of contracting more severe forms of the disease.
The immunosuppressive accommodations made by a mother’s body on the behalf of a fetus during pregnancy may leave expectant mothers more susceptible to WNV than people with full immunocompetence (1,2). There are data from animal models that support this concept (3). There have also been several documented cases of the virus being capable of maternal fetal transmission but not automatic (1,4-6).
EXPOSURE
Less than 1% of the people bitten by mosquitoes will ever be exposed to WNV and only approximately 20% of WNV-exposed individuals will ever develop the symptoms associated with WNF according to the Center for Disease Control’s (CDC) records (7). Of those people infected who become symptomatic, it is estimated that 10% will seek medical attention for their illness.
The more severe neuroinvasive expression is far less common than 1 in 10 exposed and occurs in only 1 in 150 exposed individuals (infections occurring during 2008 with number of human cases if any, by state.
If WNV infection is reported to CDC from any area of a state, that entire state is shaded.Data Table
Avian, animal or mosquito WNV infections have been reported to CDC ArboNET from the following states in 2008: Alabama, Arizona, Arkansas, California, Colorado, Connecticut, Delaware, District of Columbia, Florida, Georgia, Idaho, Illinois, Indiana, Iowa, Kentucky, Louisiana, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Jersey, New Mexico, New York, North Dakota, Ohio, Oklahoma, Oregon, Pennsylvania, Puerto Rico, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, Virginia, Washington, West Virginia, Wisconsin, and Wyoming.
Human cases have been reported in Alabama, Arizona, Arkansas, California, Colorado, Connecticut, Delaware, District of Columbia, Florida, Georgia, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Jersey, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Oregon, Pennsylvania, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, Washington, West Virginia, Wisconsin, and Wyoming.
USGS: http://diseasemaps.usgs.gov/
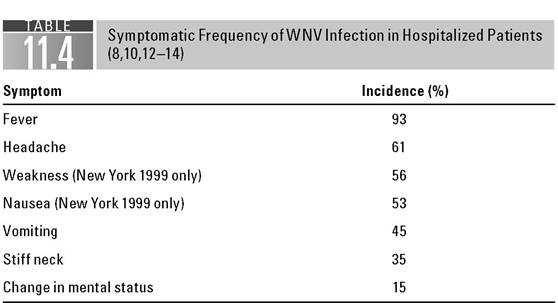
Mild forms of the infection, which are referred to as WNF, generally set in within 3 to 14 days of being exposed to an infected mosquito. Symptoms can include nausea, vomiting, anorexia, backache, neck ache, malaise, rash, myalgia, and lymphadenopathy (7).
Signs of confusion, muscle weakness, arthralgias, paresis, and abnormal sensory or reflex responses are elements that may be found in the more severe neuroinvasive expression ofWNME. 'The full neurological presentation ofWNV's
severe form including those documented by the CDC may include ataxia and extrapyramidal signs, abnormalities of the cranial nerve, optic neuritis, polyradiculitis, myelitis, seizures, or coma.
Meningitis, encephalitis, and flaccid paralysis are also possible with meningoencephalitis more common than meningitis alone (7).Patients presenting with several of the aforementioned symptoms
■ In a highly mosquito active region
■ With inexplicable meningitis or encephalitis especially from May to September (Summer and early Fall months)
■ With a recent history of mosquito bites
■ Who have recently traveled to mosquito-prone areas of the world including jungle and/or tropical environments, where mosquitoes are more prevalent
■ Who have a relative (particularly over the age of50) with a newly acquired case of meningitis or encephalitis
should arouse additional suspicion of a possible WNV infection.
DIAGNOSIS-LABORATORY
As signs and symptoms of WNV cannot be reliably distinguished from either arbo- viral infections or many of the tick-borne encephalitides, identification is made by the detection of IgM antibody in acute-phase serum or cerebrospinal fluid (CSF) through serologic analysis (20). Rapid testing is available through usage of a TaqMan® reverse transcriptase-PCR assay, yet detection of IgM antibody to WNV in serum or CSF using MAC-ELISA is the most efficient method for verifying the presence of WNV (7, 27). Since IgM antibodies do not cross the blood-brain barrier, IgM antibody in CSF strongly suggests CNS infection (7).
TREATMENT
Although treatments and vaccines are currently under development, there is no recognized treatment or cure for WNV in either adults or children (28). Generally, treatment consists of supportive care tailored to address particular symptoms and the risk of secondary infection with severe cases commonly requiring respiratory support as well as IV fluids. Antipyretics and analgesics may help in symptomatic treatment. The rest of the knowledge currently available on potential treatments deals principally with the use of ribavirin, interferon a-2b, and intravenous WNV antibodies, which have all yet to be examined in controlled studies (29).
Of the experimental treatments currently under development—including a killed whole virus vaccination, a live attenuated chimeric virus vaccination, and passive immunization—attenuated chimeric virus offers perhaps the most promising results (30,31).
The use of intravenous immunoglobulin (IVIG) with a high titer of WNV antibodies has yet to be studied in pregnant women but has been successfully used in a case of an immunosupressed lung transplant patient (32). IVIG has also been studied along with pooled human plasma (PP) for treatment of WNV-infected mice demonstrating prophylactic and therapeutic efficacy (33).
While unfortunately adults and children to this point have no comprehensive treatment, a treatment for in vitro WNV infections may have two very promising options, including the use of nucleoside analogue ribavirin or interferon α-2b.
Insofar as an infected mother is concerned, high does ribavirin nor interferon α-2b has shown effectiveness in combating WNV in adults (34). Ribavirin and interferon have however been linked to a variety of hematologic complications including anemia, bone-marrow suppression, neutropenia, and thrombocytopenia under different combinations of circumstances.
CONCLUSION
Obstetricians as well as other doctors should remain mindful of the potential hazard that WNV may pose to pregnant women as well as their unborn children, particularly in mosquito-endemic areas. As there is no established treatment, preventative measures involving mosquito avoidance and management remain the best measure for combating the morbidity and the mortality associated with WNV until vaccinations and direct cures become available for wide scale usage. Health care providers should be highly suspicious of cases which present with a number of symptoms consistent with West Nile viral infections during the mosquito season, summer months (35,36).
References
1. Chappa J, Ahn J, DiGiovanni L, Ismail M. West Nile virus encephalitis during pregnancy.
Obstet Gynecol. 2003;102:229-230.2. Bruno J, Rabito FJ, Dildy GA. West Nile virus meningoencephalitis during pregnancy. JLa StateMedSoc. 2004;156(4):204-205.
3. Cordoba L, Escribano-Romero E, Garmendia A, Saiz JC. Pregnancy increases the risk of mortality in West Nile virus-infected mice. JGen Virol. 2007;88(pt 2):476-480.
4. Carles G, Peiffer H, Talarmin A. Effects of dengue fever during pregnancy in French Guiana. Clin Infect Dis. 1999;28:637-640.
5. O'Leary DR, Kuhn S, Kniss KL, et al. Birth outcomes following West Nile virus infection of pregnant women in the United States: 2003-2004. Pediatrics. 2006;117: e537-e545.
6. Skupski DW, Eglinton GS, Fine AD, Hayes EB, O'Lery DR. West Nile virus during pregnancy: a case study of early second trimester maternal infection. Fetal Diag n Ther. 2006;21(3):293-295.
7. CDC. EpidemicJEpizootic West Nile Virus in the United States: Guidelines for Surveillance, Prevention, and Control. 3rd Revision 2003.
8. Petersen L, Marfin A. West Nile virus: a primer for the clinician [Review]. Ann Intern Med. 2002;137:173-179.
9. CDC. Virology: classification of West Nile virus. Available at: www.cdc.gov/ncidod/ dvbid/westnile/virus.htm (accessed May 23, 2009).
10. CDC. Background: virus history and distribution. Available at: www.cdc.gov/ncidod/ dvbid/westnile/background.htm (accessed May 27, 2009).
11. Petersen L, Roehrig J. West Nile virus: a reemerging global pathogen. Emerg Infect Dis. 2001;7:611-614.
12. Tsai T, Popovici F, Cernescu C, et al. West Nile encephalitis epidemic in southeastern Romania. Lancet. 1998;352:767-771.
13. Platonov A, Shipulin G, Shipulina O, et al. Outbreak of West Nile virus infection, Volgograd Region, Russia, 1999. Emerg Infect Dis. 2001;7:675-678.
14. Weinberger M, Pitlik S, Gandacu D, et al. West Nile fever outbreak, Israel, 2000: epidemiologic aspects. Emerg Infect Dis. 2001;7(4):686-691.
15. CDC. 2008. West Nile virus activity in the United States. Available at: www.cdc.gov/ ncidod/dvbid/westnile/Mapsactivity (accessed May 27, 2009).
16. CDC. 2003. West Nile virus activity in the United States. Available at: www.cdc.gov/ ncibod/dvbid/westnile/activity.htm (accessed May 27, 2009)
17. CDC. Statistics, surveillance and control: West Nile virus disease 2003 human cases by clinical syndromes as of May 25, 2009. Available at: www.cdc.gov/ncidod/dvbid/ westnile/prevention_info.html (accessed July 15, 2004).
18. Asnis DS, Conetta R, Teixeira AA, et al. Thie West Nile virus outbreak of 1999 in New York: the Flushing Hospital experience. Clin Infect Dis. 2000;30(3):413-418.
19. CDC. Interim guidelines for the evaluation of infants born to mothers infected with West Nile virus during pregnancy. MMWR. 2004;53:154-157.
20. Surveillance and reporting guidelines for West Nile virus. Washington: Department of Health; 2004. Available at: www.doh.wa.gov/Notify/giudelines/wnv.html (accessed May 18, 2009).
21. CDC. Vertebrate ecology. Available at: www.cdc.gov/ncidod/dvbid/westnile/ birds&mammals.htm (accessed May 26, 2009).
22. Solomon T, Ooi M, Beasley D, et al. West Nile encephalitis. Br Med J. 2003;326: 865-869.
23. CDC. Possible West Nile virus transmission to an infant through breast feeding- Michigan, 2002. MMWR. 2002;51:877-878.
24. CDC. Update: investigations of West Nile virus infections in recipients of organ transplantation and blood transfusion. MMWR. 2002;51:879.
25. CDC. Update: West Nile virus screening of blood donations and transfusion- associated transmission—United States, 2003. MMWR. 2004;53:281-284.
26. CDC. Detection of West Nile virus in blood donations—United States, 2003. MMWR. 2003;52;769-772.
27. Halstead S, Jacobson J. Japanese encephalitis. Adv Virus Res. 2003;61:103 138.
28. Monath TP. Prospects for the development of a vaccine against the West Nile virus. Ann N Y Acad Sci. 2001;951:1-12.
29. http://www.turner-white.com/memberfile.php7PubCode = hp_may04_nile.pdf
30. Monath T, Arroyo J, Miller C, et al. West Nile virus vaccine. Curr Drug Targets Infect Disord. 2001;1:37-50.
31. Jordan I, Briese T, Fischer N, Lau JYN, Lipkin WI. Ribavirin inhibits West Nile virus replication and cytopathic effect in neural cells. J Infect Dis. 2000;182:1214-1217.
32. Hamdan A, Green P, Mendelson E, et al. Possible benefit of intravernous immunoglobulin therapy in a lung transplant recipient with West Nile virus encephalitis. Transpl Infect Dis. 2002; 4:160-162.
33. Ben-Nathan D, Lustig S, Tam G, et al. Prophylactic and therapeutic efficacy of human intravenous immunoglobulin in treating West Nile virus infection in mice. J Infect Dis. 2003;18:5.
34. Chowers MY, Lang R, Nassar F, et al. Clinical characteriscs of the West Nile fever outbreaks, Israel, 2000.Emerg Infect Dis. 2001;344:1807-1814.
35. CDC. Intrauterine West Nile Virus infection—New York, 2002. MMWR. 2002;51: 1135-1136.
36. Hinckley AF, O'Lery DR, Hayes EB. Transmission of West Nile virus through human breast milk seems to be rare. Pediatrics. 2007;119(3):666-671.
More on the topic Mosquito-Borne Illnesses: Western Nile Virus:
- Mosquito-Borne Illnesses: Western Nile Virus
- CONTENTS
- Benrubi Guy I. (ed.). Handbook of Obstetric and Gynecologic Emergencies. 4th edition. — Lippincott Williams & Wilkins,2010. — 424 p., 2010
- INDEX
- Macrovascular Complications of Diabetes Mellitus