Treatment principles for vulvodynia patients
The management approach to a patient with vulvodynia is similar to a patient with a chronic vulval skin disease with a focus on the same clinical outcomes. As vulvodynia is a chronic pain condition, the treatment options focus on pain modification through pain-modifying drugs, pelvic floor muscle rehabilitation, and psychological and psychosexual support.
Many gynaecologists lack the knowledge, skills, and competencies to provide chronic pain management so it is important to refer on to other health professionals if not confident. A gynaecologist should be expected, however, to assess the patients and start basic treatment. The evidence base for the optimal treatment is poor, but the British Society for the Study of Vulval Diseases, a society representing health professionals who have an interest in vulval disease, has produced national guidance on the management based on existing evidence (9). This guidance focuses on stratifying patient care depending on needs and the role of the multidisciplinary team. Box 50.1 summarizes the principles of managing of vulvodynia (Figure 50.7).Surgery for provoked pain
Surgical excision of the vestibule may be appropriate for a small subgroup of patients with localised provoked pain (vestibulodynia) where there is localised peripheral nerve proliferation. There is evidence to support this treatment (41). The modified vestibulectomy is the procedure of choice for patients with vestibulodynia. It involves excision of a horseshoe-s haped area of the vestibule followed by dissection of the posterior vaginal wall to cover the skin defect. In the largest series, the outcome was pain-free sex in 59%
Box 50.1 Vulvodynia (all types): an outline of treatment strategies which should be combined
Patient education
• An explanation of chronic pain pathways.
• Informal patient support and information through patient organizations such as the Vulval Pain Society (http:// www.vulvalpainsociety.org) and the National Vulvodynia Association (http://www.nva.org) can be helpful.
Pain modification treatments
• Pain-modifying drugs (amitriptyline and/or gabapentin) are useful for moderate to severe unprovoked pain. Titrating doses of amitriptyline should be considered (38). Side effects usually settle within 2 weeks.
• Patients who are intolerant of the drugs, have severe pain, or have a decline in function should be referred to a pain management service (nerve blocks, intralesional injections, transcutaneous electrical nerve stimulation, and acupuncture).
• Local anaesthetic gels/ointment prior to sex should be considered. Occasionally, contact dermatitis can develop so they should be used with caution.
Physical therapy
• Pelvic floor muscle hypertonicity may exacerbate the pain cycle (39). Treatment aims to relax and desensitize these muscles. Techniques evidenced in the literature include pelvic floor exercises, use of vaginal dilators, and digital pelvic floor trigger point therapy delivered by a physiotherapist.
Psychological and psychosexual therapy and support
• Basic level psychological support should be given by all health professionals which includes reassurance that there is no underlying medical problem, challenge abnormal beliefs about symptoms, and the role of stress and how it amplifies pain perception
• Some patients require mindfulness/cognitive behavioural therapy self-management or formal referral to a clinical psychologist (39, 40). Figure 50.7 outlines the ‘hot-cross bun' connection that can connects thoughts, emotions, physical sensations, and behaviour.
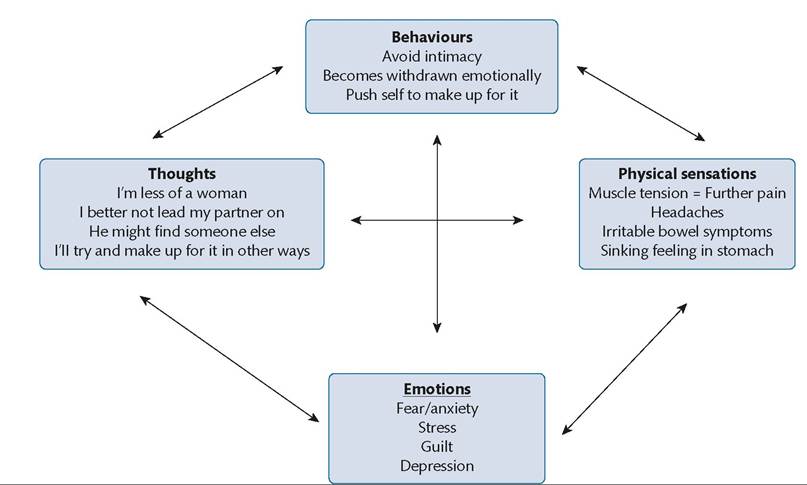
Figure 50.7 A 'hot-cross bun' diagram of how behaviours, thoughts, physical sensation, and emotions may be interlinked in patients with vulvodynia.
with favourable long-term follow-up (41). In a randomized controlled trial, 78 women with Vestibulodynia were randomized to one of three arms: group cognitive behavioural therapy (12 weeks’ duration), pelvic floor biofeedback therapy (12 weeks duration), and vestibulectomy (42). At 6 months, all patients reported significant improvements in pain scoring. Sexual functioning with surgery had the highest success rates; however, one concern was the high number of participants randomized to surgery who declined to be included in the study. The study supported both non-surgical treatments for vestibulodynia and suggested that patients prefer a behavioural approach to treatment than a surgical one. The clinical community remain divided on the value of surgery to treat this condition.