Vulval cancer
Epidemiology and aetiology of vulval cancer
Vulval cancer is the fourth most common gynaecological cancer and accounts for 6- 7% of all gynaecological malignancies. The incidence is approximately 2-3/100,000 women per year (44).
Vulval cancer is more common in elderly women, with a median age at presentation of approximately 68 years. In the last decades, the incidence of vulval cancer has been slowly increasing (45, 46). This is thought to be related to the ageing of the population and the increasing incidence of VIN (46). Squamous cell carcinoma is the most common type, and accounts for 80-90% of all cases. Malignant melanomas, adenocarcinomas, and basal cell carcinomas are much less common. The initial route of spread is to the inguinofemoral lymph nodes. Haematogenous spread and spread by direct extension also occur, but are much less frequent.Vulval squamous cell cancer originates following two independent pathways (Figure 65.1) (47, 48). The first and most common type occurs in elderly women and is related to the presence of lichen sclerosus and/or differentiated VIN. This type accounts for approximately 80% of all vulval cancers. Studies in differentiated VIN lesions and vulval squamous cell carcinomas indicate that they share identical TP53 mutations, supporting a pathogenetic connection between them (49). The second type of vulval cancer primarily affects younger women. Persistent infection with high-risk HPV, predominantly HPV 16, is involved in the majority of these cases of vulval cancer. This type of carcinoma is associated with vHSIL. Risk factors include cigarette smoking and immunodeficiency syndromes. The reported proportion of vulval cancers associated with HPV varies widely, ranging from 15% to 79% (47).
Clinical features and diagnosis of vulval cancer
Most patients present with a vulval mass, and often there is a long history of vulval itching, associated with lichen sclerosus.
Some patients present with vulval bleeding, discharge, dysuria, or a metastatic mass in the groin. Unfortunately, there is often a delay in diagnosis; patients may feel too embarrassed to visit their general practitioner, which is especially the case in older women (patients' delay). Also doctors may contribute to the delay due to the resemblance of the complaints with more common diagnoses, such as candidal infections, vulval atrophy, or lichen sclerosus (doctors' delay). This delay especially occurs when doctors prescribe medication without proper visual inspection of the vulva.On physical examination there is a lesion on the vulva that may have a warty or ulcerating appearance (Figure 65.2). Several tumour characteristics are important to document, as they may influence primary treatment planning: size of the lesion, uni- or multifocality, and distance to the midline describing whether the tumour encroaches critical midline structures such as the clitoris, anus, or urethra. Distance of the medial margin of tumour to the midline determines whether ipsi- or bilateral lymph drainage to the groins is to be expected and thereby whether groin treatment should be ipsi- or bilateral. Involvement of clitoris, anus, and/or urethra often means
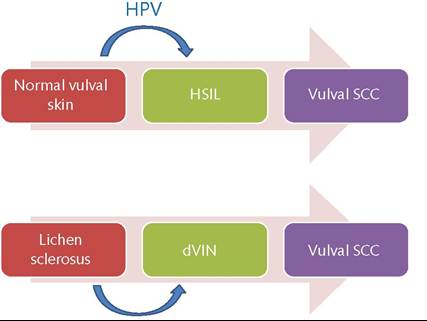
Figure 65.1 The two different pathways for development of vulval cancer. dVIN, differentiated type VIN; HPV, human papillomavirus; SCC, squamous cell cancer; uVIN, HSIL (High-grade squamous intraepithelial lesion).

Figure 65.2 Squamous cell carcinoma of the vulva.
that these structures will need to be radically excised together with the primary tumour. Such information is important for treatment planning and for accurate pretreatment counselling of the patient. Palpation of the groins should also be performed, as this is the first site of lymphogenic metastasis.
The diagnosis of vulval cancer is made by an incision biopsy or punch biopsy for histopathological examination. For accurate treatment planning the localization of the primary tumour is important. Excision biopsy should therefore be avoided. In patients with multiple vulval lesions, all lesions should be biopsied separately, with clear mapping of the vulva.
Because vulval cancer is such a rare disease, and outcome of treatment is related to experience of the treating physicians, treatment should be centralized in centres by a multidisciplinary team with adequate experience in the treatment of this disease. Members of the team should include urologists, colorectal surgeons, plastic surgeons, and radiation oncologists.
Staging of vulval cancer
The TNM classification and the International Federation of Gynecology and Obstetrics (FIGO) staging systems are relatively similar and classify vulval cancer on the basis of the size of the tumour (T), whether the cancer has spread to lymph nodes (N), and whether it has spread to distant sites (M). Vulval cancer was clinically staged until 1988. Considering that palpation of the groins is inaccurate in approximately 25% of the patients (50), the FIGO changed to surgicopathological staging of vulval cancer in 1988. This staging provided far better discrimination of survival between stages than the 1970 FIGO clinical staging system (51). In 1994, stage IA was added to the staging system, because of the negligible risk of groin node metastases in tumours with a depth of invasion smaller or equal to 1 mm (52). In 2009, FIGO staging and TNM classification were adjusted in order to allow for better prognostic discrimination between stages and less heterogeneity within stages. The number of lymph node metastases has been shown to have major impact on survival; a 5-year survival of greater than 90% for patients with negative nodes, 75% for patients with one or two positive nodes, 36% for patients with three or four positive nodes, 24% for patients with five or six positive nodes, and 0% for patients with seven or more positive nodes (53).
Also, the size of metastases has anTable 65.4 FIGO staging of vulval cancer
| Stage | Description | |
| Stage I | Tumour confined to the vulva or perineum No lymph node metastases IA: Lesions ≤2 cm in size, with depth of invasion ≤1 mm IB: Lesions >2 cm in size, with depth of invasion >1 mm | |
| Stage II | Tumour of any size with extension to adjacent perineal structures (1/3 lower urethra, 1/3 lower vagina, anus) with negative nodes | |
| Stage III | Tumour of any size with or without extension to adjacent perineal structures (1/3 lower urethra, 1/3 lower vagina, anus), with positive inguinofemoral lymph nodes: IIIA: 1 lymph node metastasis (≥5 mm) or 1-2 lymph node metastases (<5 mm) IIIB: ≥2 lymph node metastases (≥5 mm) or ≥3 lymph node metastases (<5 mm) IIIC: lymph node metastases with extracapsular spread | |
| Stage IV | Tumour invades other regional or distant structures IVA: tumour invades any of the following: • Upper urethral and/or vaginal mucosa, bladder mucosa, rectal mucosa, or fixed to the pelvic bone • Fixed or ulcerated inguinofemoral lymph nodes IVB: any distant metastases, including pelvic lymph nodes | |
| TNM | I Description | |
| T = Tumour | T1A | Tumour confined to vulva/perineum, ≤2 cm in size, and depth of invasion ≤1 mm |
| T1B | Tumour confined to vulva/perineum, >2 cm in size, or depth of invasion >1 mm | |
| T2 | Tumour involves lower urethra/vagina/anus | |
| T3 | Tumour involves upper urethra/vagina, bladder/rectal mucosa, or pelvic bone | |
| N = Nodes | N0 | No lymph nodes involved |
| N1a | Lymph node metastases: one or two nodes <5 mm | |
| N1b | Lymph node metastases: one node ≥5 mm | |
| N2a | Lymph node metastases: 3 or more nodes <5 mm | |
| N2b | Lymph node metastases: 2 or more nodes ≥5 mm | |
| N2c | Presence of extracapsular spread | |
| N3 | Fixed or ulcerated lymph node metastases | |
| M = Metastasis | M0 | No distant metastases |
| M1 | Any distant metastases | |
impact on survival; 5-year disease-specific survival rates are 90.9% for patients with metastases smaller than 5 mm, 41.6% for those with metastases between 5 and 15 mm, and 20.0% for those with metastases greater than 15 mm (54).
Extracapsular tumour growth also negatively influences survival (54, 55). These results led to the incorporation of the number and size of lymph node metastases in the most recent staging system (56). For an overview of the latest vulval cancer TNM and FIGO classifications see Tables 65.4 and 65.5.Management of early-stage vulval cancer
History of surgical treatment
The cornerstone of treatment of vulval cancer patients is surgery. A recent Canadian study on patterns of care in 978 vulval cancer patients showed that 85% had at least one surgical procedure, and approximately 25% received radiotherapy (57). Standard treatment for squamous cell cancer of the vulva has changed dramatically over the last decades. Early in the twentieth century, the ‘en bloc' dissection of the vulva and inguinofemoral lymph nodes was introduced (58-60). This radical approach drove out simple local excision in the second half of the last century and became the standard of care for a prolonged period of time. The rationale for this approach was the assumption that prognosis is better after elective inguinofemoral lymphadenectomy compared to surveillance of the groins, despite the fact that only about 30% of patients will have inguinofemoral lymph node metastases. Although highly effective, the morbidity of this treatment was very high. Wound breakdown, infections, and lymphoedema were of great concern and often resulted in prolonged hospitalization. Since then, many modifications of surgery have been proposed in the treatment of vulval cancer patients with the aim of all modifications to reduce morbidity of vulval cancer treatment without compromising survival rates. Steps forward were made with the introduction of inguinofemoral lymphadenectomy through separate groin incisions (61), replacement of radical vulvectomy by wide local excision (62), abandonment of bilateral lymphadenectomy in lateralized tumours less than 2 cm in size (63, 64), and abandonment of inguinofemoral lymphadenectomy in microinvasive tumours (<1 mm depth of invasion) (52).
Due to these modifications, treatment-related morbidity has decreased, but is still significant for patients undergoing inguinofemoral lymphadenectomy. In the short term, wound infections (of the groins 21-39%), lymphoceles (11-40%), and wound breakdown (12.5-39%) (65) cause significant morbidity and prolonged hospital stay and/or frequently cause readmission to the hospital. In the long term, lymphoedema is the most frequent complication, being described in 14-49% of the patients (65).Currently local excision with a tumour-free margin of 1-2 cm is advised for local treatment. The presence of groin node metastases in vulval cancer is the most important prognostic factor, therefore urging adequate evaluation of the groins. For patients with unifocal tumours smaller than 4 cm, the sentinel node procedure can be performed (see ‘Sentinel node biopsy'). In patients with multifocal tumours or tumours larger than 4 cm, elective ipsi- or bilateral inguinofemoral lymphadenectomy, depending on the location of the tumour with respect to the midline (Figure 65.3), remains the standard of care. Bilateral groin treatment is indicated in patients with a vulval tumour within 1 cm of the midline. In lateralized tumours (located >1 cm from the midline), only ipsilateral groin treatment is indicated. Until now, results of imaging, such as computed tomography (CT), magnetic resonance imaging (MRI), ultrasonography, and positron emission tomography were not good enough to exclude lymph node metastases with a high enough negative predictive value (66, 67).
Sentinel node biopsy
The sentinel node is defined as the first regional lymph node to which cancer cells are most likely to spread from a primary tumour (Figure 65.2). An important benefit of the procedure is that it enables pathological ultrastaging of the first tumour-draining lymph
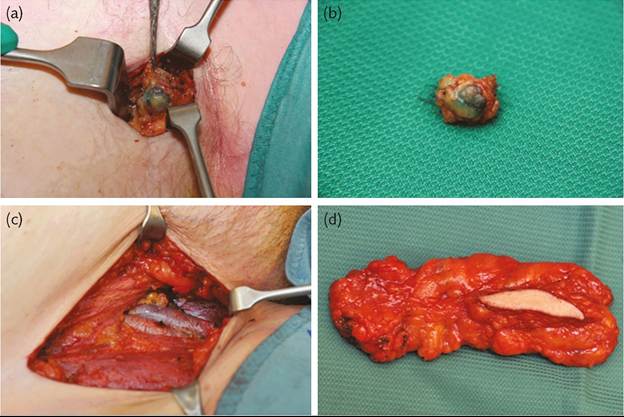
Figure 65.3 The sentinel node procedure versus inguinofemoral Iymphadenectomy: (a, b) sentinel node procedure with the removed sentinel lymph node; (c, d) inguinofemoral lymphadenectomy.
node. Pathological ultrastaging consists of multiple sectioning and immunohistochemistry, allowing more accurate examination of the lymph node. Accurate examination of the sentinel node is thought to be crucial since this determines further therapeutic planning. False-negative sentinel node assessment leads to omission of lymphadenectomy, which may lead to tumour outgrowth of metastatic lymph nodes that have been left behind. Especially in vulval cancer missing lymph node metastases is extremely harmful since tumour recurrences in the groin are very hard to treat and often fatal (68).
The first pilot study of the sentinel node procedure (Figure 65.4) in vulval cancer was reported in 1994 (69). Subsequently, larger studies (in which the sentinel node procedure always was followed by an inguinofemoral lymphadenectomy) were designed in order to investigate the diagnostic accuracy of the sentinel node
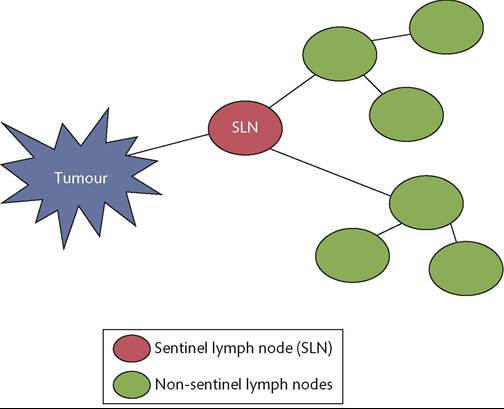
Figure 65.4 The concept of the sentinel node procedure.
procedure in patients with early-stage vulval cancer. Identification rates were high, especially with the combined procedure (radioactive tracer and blue dye), and false-negative rates were low (70). In 2008, the results of the first large prospective validation study were published. In this study, patients with squamous cell cancers of the vulva less than 4 cm in size and non-suspicious groin nodes at palpation were included. In these patients sentinel node detection was performed using a radioactive tracer and blue dye. When the sentinel node was negative, inguinofemoral lymphadenectomy was omitted. In the course of the study, groin recurrences occurred in a small proportion of vulval cancer patients with multifocal disease. It was hypothesized that lymph flow in these tumours is more complex and not accurately predictable by the sentinel node procedure. This led to a protocol amendment, in which multifocal disease became an exclusion criterion. The study showed that inguinofemoral lymphadenectomy can be safely omitted in patients with a negative sentinel node (2.3% groin recurrences in patients with unifocal vulval cancer) with a 3-year disease-specific survival of 97%. This study also showed a major decrease in treatment-r elated morbidity after sentinel node dissection compared with inguinofemoral lymphadenectomy (lymphoedema 1.9% vs 25.2%, and recurrent erysipelas 0.4% vs 16.2%) (71). Shortly thereafter, a large accuracy study on sentinel nodes and vulval cancer was published. This study showed similar results on diagnostic accuracy for patients with tumours smaller than 4 cm. Safety could not be evaluated, as all patients underwent sentinel node biopsy, followed by inguinofemoral lymphadenectomy (72). Based on these two large studies, the sentinel node procedure is nowadays recommended in the treatment of early-stage vulval cancer (70). In order to prevent fatal groin recurrences the following criteria should be met:
• Histologically proven primary squamous cell vulval cancer with a depth of invasion greater than 1 mm.
• Tumours less than 4 cm, not involving anus/vagina/urethra.
• Unifocal tumour.
• No clinically suspicious lymph nodes.
• Enlarged lymph nodes excluded by preoperative imaging (CT/ ultrasonography/MRI).
The size of sentinel node metastases has important prognostic value. Data suggest that 2 mm would be an appropriate cut-off for micrometastases, since prognosis was especially worse for those patients with sentinel node metastases larger than 2 mm. However, there is no cut-off beneath which the chance on additional metastases is that low that inguinofemoral lymphadenectomy can be safely omitted (73). Further data are needed to learn about the clinical significance of these small metastases, and to establish their possible role in clinical decision-making.
Centres that wish to offer the sentinel procedure to their patients should have high enough exposure to guarantee good quality at every step of this multidisciplinary procedure. Only then can fatal groin recurrences be avoided. An exposure of at least ten vulval cancer patients per year is advised to keep experience at a high enough level. Two recent studies showed that sentinel lymph node biopsy is the most cost-effective strategy for the management of patients with early-stage vulval cancer due to lower treatment costs and lower costs due to less long-term complications and its impact on quality of life (74, 75).
Adjuvant radiotherapy
Postoperatively, radiotherapy is indicated for vulval cancer patients with more than one lymph node metastasis, or in the presence of extranodal tumour growth. This policy is based on a study by Homesley et al. in which vulval cancer patients with lymph node metastases at inguinofemoral lymphadenectomy were randomized between pelvic lymph node dissection and postoperative radiotherapy. The results of survival were in favour of the radiation group, and the benefit was most pronounced in those patients who had clinically suspicious or fixed ulcerated groin nodes, or two or more metastatic lymph nodes (76, 77). It seems that adjuvant radiotherapy is not beneficial in patients with only one intranodal lymph node metastasis (78); however, data are conflicting on this subject (79). The addition of chemotherapy as a radiosensitizer might give better treatment outcomes compared to radiotherapy alone (80). Current treatment guidelines are based on data obtained in the ‘pre-sentinel node era’. While no one argues the rationale for postoperative radiotherapy in case of two lymph node metastases larger than 2 mm, the evidence for postoperative radiotherapy in case of two sentinel lymph nodes with only isolated tumour cells is at least questionable. Data on this subject in vulval cancer are until now not available.
Management of advanced vulval cancer
Although a formal definition does not exist, vulval cancer is considered to be locoregionally advanced in case of a vulval tumour without distant metastases that is beyond surgical resection with standard (radical) vulvectomy, irrespective of groin node involvement (81). Included in this category are patients with T2 or T3 tumours (Table 65.5). Management in these patients needs to be individualized and requires considerable pretreatment assessment, also taking comorbidity and/or frailty of the patients into account. Therefore, a multidisciplinary setting is needed to optimize treatment planning in this category of patients.
Surgery remains, when possible, the treatment of choice. However, definitive curative surgery in these patients generally is
Considering the often high morbidity associated with upfront surgery (primary or neoadjuvant), chemoradiation might be an alternative. Chemoradiation in patients with locoregionally advanced disease gives high complete clinical and pathological response rates with acceptable toxicity (82, 83). However, in elderly patients in whom comorbidity and frailty may be considerable, the side effects of both treatment options have to be weighed up.
Prognosis and follow-up of vulval cancer
Prognosis of early- stage vulval cancer patients with negative nodes is very good, with a 10-year disease-specific survival of 91%. For early- stage vulval cancer patients with positive nodes, 10-year diseasespecific survival is much worse at around 65% (84).
Prognosis is worse for higher FIGO stages. The pooled 5-year overall survival for vulval cancer patients is 65%. For FIGO stages I, II, III and IV, the 5-year overall survival is 84%, 75%, 48% and 9.4%, respectively (85).
The advised follow- up schedule after primary surgical treatment is:
• first visit: 6-8 weeks postoperatively
• first 2 years: every 3 months
• third and fourth year: biannually
• afterwards: annually lifelong.
There is no evidence for the best follow-up schedule. Since local recurrences may occur many years after primary treatment, lifelong follow-up is advised. Regular follow-up is thought to lead to earlier detection, and consequently more effective treatment of local recurrent disease (86). Follow-up visits should include clinical examination of vulva and groins. No standard imaging is advised.
Recurrent disease
Recurrences in vulval cancer can be subdivided according to site: local recurrences (recurrences on the vulva), groin recurrences, and distant recurrences (includes pelvic recurrences). Recurrences can also occur in multiple sites. Local recurrence is a frequent event after primary treatment, and local recurrences can occur many years after primary treatment (84). Local recurrences are treated with curative intent, with wide local excision of the vulval tumour when possible. When surgical excision is not an option due to the extent of disease or the condition of the patients, treatment with radio(chemo)therapy can be given. When local recurrences occur in patients with previously negative sentinel nodes, an elective inguinofemoral lymphadenectomy should be performed too. The sentinel node procedure seems to be feasible in locally recurrent disease; however, there are no data on the safety of this procedure in these patients (87). Despite the fact that local recurrences are treated with curative intent, the prognosis for these patients is significantly decreased when a local recurrence occurs (84).
Groin recurrences are extremely difficult to treat and occur mostly within the first 24 months after primary treatment. The incidence of groin recurrences is 1% after a negative inguinofemoral lymphadenectomy (based on retrospective data), 3% after a negative sentinel node (based on prospective data), and 7% after a negative superficial lymphadenectomy (prospective data) (70). In the case of groin lymph node metastases at the time of primary treatment, groin recurrences are observed in 8-25%, depending on the mode of primary treatment (73, 88). Groin recurrences are preferably treated by lymph node debulking by inguinofemoral lymphadenectomy, followed by radiotherapy. The addition of chemotherapy can be considered in these cases. When debulking surgery is not possible due to the extent of the disease, primary radio(chemo)therapy can be given. Groin recurrences are often fatal, as a very limited number of patients have long-term survival (68).
Patients with distant recurrences cannot be cured. Treatment in these cases should be individualized; treatment options are palliative chemotherapy and/or radiotherapy.
Rare vulval tumours
Vulval melanomas are the second most common vulval malignancy, and account for 5-10% of all vulval malignancies. The biological behaviour of vulval melanoma is similar to that of cutaneous melanoma and therefore it is thought that staging and treatment should follow the same guidelines as for cutaneous melanoma (89, 90). Therefore, surgical treatment consists of wide local excision with a 1 cm margin of normal skin in case of thickness of 1-2 mm or less and a 2 cm margin in case of a thickness of more than 12 mm (91). Inguinofemoral lymphadenectomy is not performed as an elective procedure in vulval melanoma, but only in case of suspicious groin nodes. The sentinel node biopsy can also be applied (92), following the same criteria as in cutaneous melanoma (depth of invasion >1 mm, or <1 mm with mitotic rate ≥1∕mm2 or ulceration). Prognosis of vulval melanoma is poor with an overall 5-year survival rate of 27-47% (93, 94). Patients with superficial lesions have an excellent prognosis; however, with increasing depth of invasion, the chances of metastases increase and the prognosis worsens.
Other, even more rare, vulval tumours are Bartholin’s gland carcinoma, other adenocarcinomas, basal cell carcinomas, and vulval sarcomas.