Vulval examination
A full vulval examination requires good lighting and each part of the vulva should be examined systematically including the mons pubis, inguinal folds, outer and inner labia (majora and minora), clitoris (body and hood), perineum, vestibule, and anus (Figure 50.1).
Hart's line is the junction between the vestibule and the inner labia and marks a change in epithelium type from mucosal type to stratified squamous. Ideally, digital and speculum examinations should be performed to rule out erosions, mucosal thickening, adhesions, and scarring as these features can be seen in conditions such as erosive lichen planus and lichen sclerosus (8). Digital vaginal examination may be helpful to assess pelvic floor muscle hypertonicity (9).Dermatological problems of the vulva may be a manifestation of a general skin condition and therefore a complete skin examination should be considered to allow a more complete assessment of disease extent and diagnosis. For example, psoriasis may manifest in ‘hidden' sites such as the umbilicus and natal cleft and eczema is found in the skin flexures. Examination of other non-keratinized or mucosal surfaces, including the oral cavity, eyes, and mouth should also be performed as certain conditions such as pemphigus vulgaris, pemphigoid, and erosive lichen planus may affect these regions (10).
Terminology of examination findings
The terms used to describe the appearance of vulval disease are largely synonymous with dermatology terminology. For example:
• ‘Erythema refers to reddening of the skin, which may be poorly demarcated, as in eczema (Figure 50.2 demonstrates poorly defined erythema in the context of contact dermatitis) or well
Table 50.1 Vulval history taking
| Question | Reasoning |
| What are the key symptoms and how severe are they? What is the impact on the patient's function? | Important to be clear on the initial symptom. Itch can suggest skin disease or infection. Pain can be secondary to itching from skin damage. Pain as a primary symptom may indicate a pain syndrome. A reduction in symptoms and improvement in function (including sex) are important clinical outcomes |
| How long has the woman been experiencing symptoms? | Acute symptoms may indicate vulvovaginal thrush or contact dermatitis. Chronic symptoms (more than 6 months) may be due to lichen sclerosus or lichen planus |
| Are there any other vulval symptoms? | Helps making a diagnosis. For example, vaginal discharge may be caused by infection |
| What treatments have been tried before? | Inappropriate topical treatments can exacerbate symptoms and potentially cause an irritant reaction. The history should explore 'failed' treatments, e.g. topical steroid type, frequency, duration and amount (under usage with these treatments is common) |
| How is the patient cleaning the vulval area? | Many women feel unclean and can over-wash leading to skin damage and further irritation |
| Are there any possible contacts with irritants such as soaps, shampoos, urine, and scented vaginal wipes? | These are potential irritants and can damage the skin potentially causing inflammation. Urine is a potent skin irritant |
| Are there any other skin conditions present? | For example, eczema (seen elsewhere in the skin flexures) or psoriasis (sometimes hidden as cracking behind the ears, a scaly scalp, or umbilical erythema). |
| Is there any systemic disease? | Other systemic disease many contribute to treatment outcome, e.g. diabetes, renal failure, anaemia, autoimmune conditions (including family history of autoimmunity), other chronic pain syndromes |
| Are symptoms stress related? | With lichen simplex and vulvodynia, symptoms are worse at times of stress and acknowledging this can become a part of the treatment plan |
demarcated, as in psoriasis (Figure 50.3).
The presence of erythema usually indicates an underlying inflammatory process. If present in association with pain, infection should be considered.• Whitening of the skin may occur in the presence of a normal epidermis such as in vitiligo, or in conjunction with epidermal change such as in lichen sclerosus.
• Lichenification is the term used to describe a leathery thickening of the skin with increased skin markings which occurs in response to persistent rubbing.
• Scale is an increase in the dead cells on the surface of the skin. The vulval region is often moist and scale is a less reliable sign than on
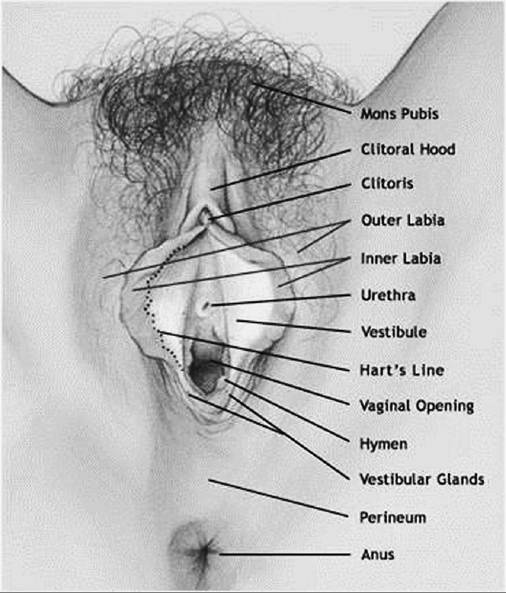

Figure 50.2 Contact dermatitis affecting the female genitalia. Note poorly defined erythema of the genitocrural skin, erosions due to excoriation in the inflamed skin, and white thickening (lichenification) of the labia majora due to scratching.
Figure 50.1 Schematic representation of the normal adult vulva.
Courtesy of Dawn Danby and Paul Waggone.

Figure 50.3 Psoriasis affecting the female genitalia. Well-demarcated erythema surrounding the anogenital area with typical psoriatic plaques in surrounding skin. The genital plaque has typical scale in the perianal area, but a lack of scale in the perineal and vulval areas.
Table 50.2 Terminology of lesions that may be seen in the vulval area
| Lesion terminology | Description | Example | |||||||||||||||||||||||
| Fissure | A thin 'hairline' crack in the skin surface. May be due to excessive dryness | Psoriasis and lichen sclerosus | |||||||||||||||||||||||
| Excoriation | Scratch mark, may be single or multiple | As seen in any itchy skin conditions, e.g. atopic eczema, lichen sclerosus | |||||||||||||||||||||||
| Erosion | A shallow denuded area due to loss of the epidermis (surface layer of skin) | Erosive lichen planus | |||||||||||||||||||||||
| Ulcer | Full thickness loss of the epidermis (top layer of skin) ± dermis | Aphthous ulceration | |||||||||||||||||||||||
| Macule | Flat area of colour change | Vulval melanosis Ecchymosis (subcutaneous purpura) seen in lichen sclerosus | |||||||||||||||||||||||
| Nodule | Large palpable lesion >0.5 cm in diameter | Squamous cell carcinoma Scabies | |||||||||||||||||||||||
| Papule | Small palpable lesion 0.5 cm in diameter. It may be elevated or may be a thickened area without being visibly raised above the skin surface | Vulval intraepithelial neoplasia Squamous cell carcinoma | |||||||||||||||||||||||
| Vesicle | Small fluid filled blister if topical steroids have been used prior to referral. Around 15% of patients have extragenital disease. The general management of lichen sclerosus is with superpotent topical steroids and emollients (18). An initial 3month course of superpotent topical corticosteroids (e.g. clobetasol propionate 0.05%), one finger-tip unit (from the tip of the finger to the first crease) nightly for 4 weeks, alternate nights for 4 weeks, and then twice a week for 4 weeks. A Cochrane review of the management of lichen sclerosus was published in 2011 (19, 20). Seven trials involving 249 patients covering six treatments were included; however, the evidence for optimal treatment was limited. Effective treatments included superpotent (clobetasol propionate 0.05%) and potent mometasone furoate 0.1%) topical steroids. Topical calcineurin inhibitors may have a place in the management of lichen sclerosus and these are usually prescribed under the supervision of a dermatologist. There was no benefit for topical testosterone or progesterone. Further trials are needed to determine the exact steroid potency, frequency, and duration of treatment. The regular usage of emollients should be used to provide a barrier to potential irritants (e.g. urine) and keep the skin hydrated. There is a high chance of symptom response following the 3month course, but lichen sclerosus remains a chronic skin disease and the symptoms are likely to recur if the treatment is stopped. Regular use of topical steroids in the long term has been shown to be safe and may reduce the underlying small risk of vulval cancer (see ‘The use of topical steroids') (21). Patients may develop symptomatic skin fissuring at the posterior fourchette. Treatment should involve digital massage of topical Table 50.3 Summary of the clinical features and treatment of specific skin diseases
Figure 50.5 Advanced vulval lichen sclerosus. Whiteness, loss of anatomy, ecchymosis seen on the left labia, and scarring over the clitoral hood. steroid into the fissure on a daily basis. The use of vaginal dilators and a good lubricant should be encouraged to help the scar reforming and help desensitize the area. If these measures do not help then consideration should be given to the use of surgical division or refashioning of the fissure or skin bridge. There is a small risk of cancer development in lichen sclerosus (with findings of typical eczema elsewhere. Patients rarely complain of vulval eczema when there is severe eczema elsewhere. However, in a patient who complains of vulval itching and who has a history of atopy, it is worth considering as a diagnosis. Vulval atopic eczema is often seen clinically as intralabial, perianal, and natal cleft erythema. The erythema is often mild. Signs of atopic eczema elsewhere include poorly defined, symmetrical, scaly erythematous areas on the skin creases (especially the antecubital fossae and behind the knees). Small fissures and erosions may be present. The skin is often noticeably dry. Severe eczema is more widespread over the trunk and limbs. Atopic vulvitis is the commonest cause of vulval itch in children. Contact dermatitis may be either ‘irritant' or ‘allergic contact'. Irritant contact dermatitis is particularly common and may be triggered by soaps, perfumes, medicaments, urine, faeces, and sweat. The barrier function of the skin becomes impaired by local irritants and can subsequently be made worse by continued application of the product. Clinical signs of vulval irritant dermatitis include poorly defined intralabial erythema that occurs anywhere where the irritant has been present. Small fissures and erosions may be present and lichenification may occur in longstanding disease (15). All of these clinical features are demonstrated in Figure 50.2. It is common that fissures become secondarily infected with skin pathogens or Candida. It is important to realize this when treatment strategies are implemented. Allergic contact dermatitis is less common and around one-fifth of patients with vulval skin conditions having a relevant positive patch test result (15). It can be difficult to distinguish from irritant contact dermatitis clinically, but affected skin usually extends outside of the genital area in ‘non-contact' areas. This is because it is an immune-mediated hypersensitivity reaction. The only way to confidently diagnose allergic contact dermatitis is through patch testing (see ‘Investigations'). Vulval seborrhoeic eczema is difficult to distinguish from psoriasis. It will often manifest as glazed skin in the interlabial sulci bilaterally. Fine scale and erythema at other affected body sites such as the nasolabial folds, scalp, and eyebrows can aid the diagnosis (26). Treatment principles for inflammatory vulval skin conditions There are no core clinical outcome measures for vulval skin disease (24) and suggested clinical outcomes include: • a reduction in symptoms (e.g. less itch, pain, and fewer flare- ups of symptoms) • an improvement in function (e.g. sexual function, mobility, and normalizing bladder and bowel function) • increased confidence in self-management (e.g. management of flare-ups and self-examination). General principles Initial principles of management are the same for all vulval skin conditions and a holistic approach is required. Good education, support, and counselling are important with extra time given to address the disease process, discussing general vulval care measures, and managing patient expectations (1). It is useful to provide information leaflets, direct patients to relevant patient-oriented websites, and write down instructions for applying topical agents (see ‘Additional resources' for sources of patient information). The use of a mirror or model in the clinic setting is helpful to show patients where to apply their topical treatments. Correct barrier function The goal of treatment is to correct barrier function and reduce inflammation. For washing, soap and other routine cleaning agents (e.g. wipes) should be avoided, as they are likely to act as irritants and sensitizing allergens. Irritation from urinary and faecal incontinence need to be addressed as these are a common cause of vulval inflammation and make underlying skin pathology worse. ‘Soap substitution' with a bland cream or ointment-based emollient is best for cleansing. The same agent can then be used as an emollient to both provide a barrier to the site and sooth inflamed skin. There is no preferred emollient to use and some can cause irritation. Emollient creams (not ointments) can be placed in the fridge. Patients find this soothing and lowering skin temperature is thought to reduce itch through central inhibitory pathways (27). The use of topical steroids Inflammation reduction associated with skin disease (such as in lichen planus, lichen sclerosus, and eczema) is achieved by the use of topical steroids. Topical steroids are often ineffectively used in the vulval area due to concerns from patients and non-specialists about side effects, particularly skin or mucosal atrophy. It is important therefore to use the correct strength of steroid for the necessary length of time on the appropriate body site. Mucosal surfaces such as the vulval vestibule are remarkably resistant to steroid atrophy. In contrast, keratinized surfaces such as the labiocrural folds, perineum, perianal area, and thighs can develop skin thinning and striae (stretch marks) with inappropriate use with potent topical steroids (1). Overuse of topical steroids appears as thinned skin which appears redder and is reversible in the early stages. In the later stages, permanent telangiectasia and striae can develop. Topical calcineurin inhibitors in the vulval region reduce inflammation and do not cause skin atrophy. However, their role is not fully understood and there is a theoretical risk of long-term localized immunosuppression from these agents causing skin cancers (28). Topical steroids should be used once a day. There is no evidence to suggest that twice-daily application is superior, although twice- daily application has greater potential to cause side effects (29). Ointments are preferable to creams as they contain fewer constituents and therefore have a lower chance of causing irritation/con- tact allergy. Once control of inflammation and symptoms has been achieved, topical steroids should be reduced to the minimum frequency required to maintain remission. The concept of ‘weekend therapy', that is, applying topical steroids on two consecutive days per week, is effective in atopic eczema patients (30) and can be extrapolated to chronic vulval diseases such as lichen sclerosus and lichen planus where long-t erm maintenance therapy is required. A patient with these conditions will use approximately 30-60 g of topical steroid per year as maintenance therapy (12). Topical steroids should only be used on affected areas to prevent side effects in adjacent skin and the use of a mirror is often helpful to aid application in the correct areas. Failure to respond to treatment If a patient fails to respond to appropriate treatment the following should be considered: 1. Poor adherence to prescribed treatment regimen: ‘steroid phobia' is a well-recognized problem when treating skin conditions. Many healthcare professionals, including pharmacists, will compound the issue by advising the patient to use sparingly and recommending not to use on ‘sensitive areas'. This cautious approach can be detrimental to the patient's treatment plan. The patient should be advised to apply the topical steroid in terms of the finger-tip unit (A finger-tip is from the very end of the finger to the first crease in the finger. It does not mean a blob on the fingertip). The number of finger-tip units required is usually one to two but is specifically tailored to the patient depending upon surface area affected by the condition. 2. Inaccurate placement of topical steroid: the patient may be applying the topical treatment to an unaffected area. This is especially common if the patient is elderly and unable to use a mirror to see what they are doing. In clinic the exact location of application should be explained, Diagrams, photographs, or models can be used as an aid. 3. Continued exposure to irritants: urine or faeces, external products such as wipes or non-prescribed topical treatments, and over-washing with water can all contribute towards irritation and ongoing symptoms. 4. An incorrect diagnosis. If adherence and skin care practices are adequate, the diagnosis may be incorrect. An allergic contact dermatitis to topical treatments may have occurred (see ‘Patch testing') or there may be premalignant or malignant change in the affected area. If there is any concern, a biopsy should be taken. The multidisciplinary team While many patients can respond well to topical treatments, there are many women who have complex needs that can be overlooked. These patients do not tend to follow any agreed clinical pathway, have unmet needs, and require adequate assessment and management (31). These women require the care of a gynaecologist with a special interest in the management of vulval disease within the context of an appropriate multidisciplinary vulval service. Indications for multidisciplinary input include: • ongoing symptoms despite appropriate use of topical steroids • for review of pathology results by a gynaecological pathologist • associated vulval intraepithelial neoplasia (usual or differentiated type) • need for patch testing • for consideration of surgery • for resolution of ongoing sexual problems. Other members of a vulval service might include dermatology, genitourinary medicine, physiotherapy, pain management, psycho- sexual therapy, pathology, and urogynaecology.
More medical literature on Medic.Studio
More on the topic Vulval examination:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|
