Zygosity, Chorionicity and Amnionicity
Waldo Sepulveda and Amy E. Wong
There is NO diagnosis of twins. There are only monochorionic twins or dichorionic twins. This diagnosis should be written in capital red letters across the top of the patient's chart.
Kypros H. Nicolaides1
Introduction
Spontaneous multiple pregnancy occurs with a frequency of approximately 1 in 90 for twins, 1 in 8,000 for triplets and 1 in 700,000 for quadruplets. With the development of assisted reproductive techniques, however, the incidence of multiple pregnancy has increased dramatically over the past several decades due to the use of ovulatory medications and the transfer of multiple embryos during in vitro fertilisation procedures.2 The increase in the rate of multiple pregnancies has tremendous clinical and logistic implications because these pregnancies are at risk for multiple perinatal complications, including pregnancy loss and severe prematurity. Indeed, although twin pregnancies account for about 1% of all pregnancies, they contribute disproportionally to more than 10% of all neonatal intensive care admissions, with considerable burden on the family, caregivers and society as a whole.2
To optimise perinatal care and outcomes, timely diagnosis of a twin pregnancy and tailoring management according to its chorionicity - that is, the number of implantation sites and therefore the number of placentas - and its amnionicity are essential.3 An integral part of antenatal management of twins includes the routine determination of chorionicity and amnio- nicity and knowledge of their clinical implications as one of the critical steps of prenatal care. With the widespread availability and use of prenatal ultrasound, most twin pregnancies are currently diagnosed sonographically early in pregnancy, providing the opportunity to accurately classify multiple pregnancies and to monitor them for specific complications depending on their chorionicity.
Because appropriate management depends so crucially on chorionicity, every professional performing obstetric ultrasound should be prepared to diagnose a twin gestation and be familiar with the sonographic signs to classify the pregnancy according to chorionicity.While chorionicity is sonographically identified based on the appearance of placentation, it does not always define the genetic composition of the pregnancy or zygosity. Twin pregnancies are classified into two groups, as dizygotic or monozygotic, based on the type of conception. Dizygotic twins result from two fertilised eggs, each one fertilised by different sperm, and are therefore associated with two different genotypes and invariably with dichorionic-diamniotic placentation. Monozygotic twins, on the other hand, develop from a single egg that is fertilised by a single sperm. The resulting morula, blastula or gastrula subsequently divides into two separate embryonic structures. Therefore these twins will have the same genotype, although placentation can vary depending on the timing of the division (Figure 3.1). If the splitting 18
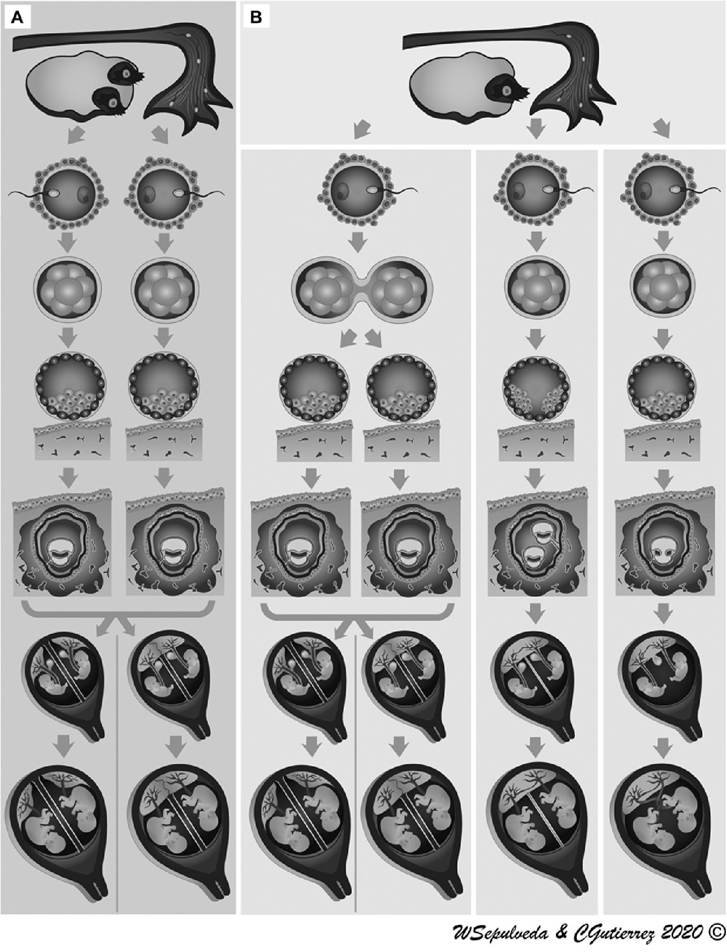
Figure 3.1 Classicalrepresentation of the three types of placentation in twin pregnancies according to zygosity. (A) Dizygotic twins develop from two separate eggs that are fertilised by two sperm; allhave dichorionic-diamniotic placentation. (B) Monozygotic twins develop from a single zygote that subsequently splits and forms two embryos. Depending on the timing of splitting, they can be dichorionic-diamniotic, monochorionic-diamniotic or monochorionic-monoamniotic. (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
process occurs within the first 3 days after conception while the morula is still in the fallopian tube and therefore before implantation, dichorionic-diamniotic twins will result. If the splitting process occurs at the blastocyst stage, between 4 and 8 days after conception and therefore during implantation, monochorionic-diamniotic twins will result.
If the division occurs during gastrulation between 9 and 12 days after conception and therefore after the amniotic cavity is formed, the twins will also share the amniotic cavity, leading to monochorionic-monoamniotic twins. Incomplete splitting of the trilaminar disk after 12 days will result in conjoined twins, which are all monochorionic-monoamniotic.2,4Before the advent of ultrasound, it was only possible to determine chorionicity by postpartum examination of the placenta(s). This was achieved by determining the number of placental masses and, in those cases with a single placental mass - which can represent a single placenta of a set of monochorionic twins or anatomically fused placentas of dichorionic twins - by assessing the characteristics of the dividing membrane. Although the pathogenesis of twinning in humans is poorly explained, basic human embryology is well understood. It is on this basis that prenatal determination of chorionicity and amnio- nicity and its relation to zygosity can be well explained. In this chapter, we review the main embryologic, clinical and sonographic factors to determine zygosity, chorionicity and amnionicity prenatally. Specific complications of twin pregnancies in both monochorionic and dichorionic twins are discussed in the other chapters of this book. We focus on chorionicity and amnionicity in twin pregnancies, as the same principles apply to higher- order multiple pregnancies.
Zygosity
Zygosity refers to the similarity of genetic material in specific loci or alleles (homozygotic or heterozygotic) and is specifically used to describe the genetic similarity or dissimilarity between twins (monozygotic or dizygotic). Monozygotic twins are genetically identical as they develop from a single zygote that subsequently splits and forms two embryos. However, they can have any of the three types of placentation: dichorionic-diamniotic, monochor- ionic-diamniotic or monochorionic-monoamniotic. Dizygotic twins, on the other hand, are genetically different as they develop from two separate eggs that are fertilised by two sperm; all are dichorionic-diamniotic (Figure 3.2).
The genome of these dizygotic conceptuses therefore will be different in the same way siblings are, theoretically sharing only 50% of the parental genes. Monozygotic twins are also known as ‘identical’ twins and dizygotic twins as ‘fraternal’ twins. It is generally accepted that approximately two-thirds of spontaneously conceived twins are dizygotic and one-third are monozygotic.Prenatal determination of zygosity has limited clinical application. Nevertheless, parental curiosity and future medical and social implications make the question of zygosity a relevant issue during prenatal counselling of multiple pregnancies.2 It is important to note that zygosity can only be determined prenatally by ultrasound under two conditions. Firstly, dizygosity can be established when the fetuses have different sexes (theoretically in 50% of the cases). We should mention, however, the exceptionally rare occurrence of opposite-sex twins in the context of a monochorionic twin pregnancy, known as hetero- karyotypic twins, which are thought to be due to either a discordant chromosomal abnormality or an unequal distribution of mosaic embryonic cells during twinning of the embryos.2,4 Secondly, when a monochorionic placenta is present, the twins are known to be monozygotic. In contrast, it is not possible to establish zygosity prenatally by ultrasound
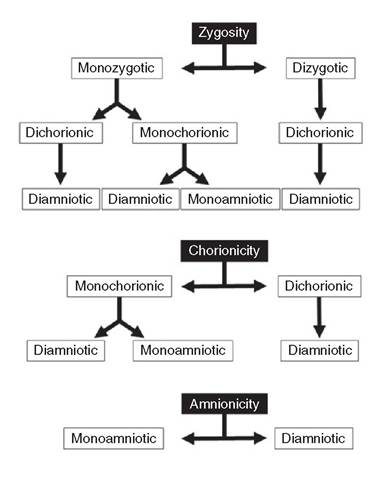
Figure 3.2 Flowchart diagrams illustrating the relationships between zygosity, chorionicity and amnionicity in twin pregnancies
in same-sex twins from dichorionic-diamniotic twin pregnancies; only DNA testing can determine if the twins are identical or fraternal. This can be done by analysing cells directly obtained from both twins, either chorionic villi or amniocytes, and comparing the genetic molecular profiles between them. This has the disadvantage of requiring an invasive procedure to obtain the fetal samples.
In recent years, the analysis of cell-free DNA and evaluation of single-nucleotide polymorphisms in maternal circulation has made it possible to examine the zygosity of twin pregnancies prenatally in a non-invasive manner.5 Nevertheless, the application of cell-free DNA for this sole purpose is not usually necessary because it is chorionicity, not zygosity, that guides proper obstetric management.3 However, with the increasing use of non-invasive prenatal screening for aneuploidy using molecular biology techniques in maternal plasma, many more twin pregnancies will undergo genetic analysis and antenatal knowledge of zygosity will be more common.Chorionicity
In multiple pregnancies, the term ‘chorionicity’ is used to refer to the number of implantation sites and therefore the number of chorionic cavities and placentas. This terminology comes from ‘chorion’ (Greek khorion, ‘membrane surrounding the fetus’), which is the tissue that is embryologically derived from the trophoblast and that forms the outermost fetal membrane that surrounds the embryo. During initial stages of embryogenesis, the fertilised ovum undergoes rapid cell division, forming the morula. At around four to five days after conception, the morula undergoes cavitation, forming the blastocyst and a fluid-filled cavity or blastocele. Simultaneously, two types of differentiated cells develop. One is an internal accumulation of cells forming a compact structure called the inner cell mass or embryoblast, from which the embryo and fetus originate. The other is the outer layer of cells that surrounds both the blastocele and embryoblast, called the trophoblast, from which the placenta and chorionic membrane originate. The trophoblast together with maternal decidua develops into the chorionic villi. Chorionic villi in contact with the decidua basalis proliferate quickly to form the chorion frondosum that fuses with the decidua basalis and becomes the placental plate and future placenta.
In contrast, growth of the chorionic villi in contact with the decidua capsularis arrests, forming the chorion leave, which then fuses with the decidua capsularis and becomes the chorionic membrane or chorion. The chorion forms the outer boundary of the entire conceptus that surrounds the amniotic sac and subsequently fuses with the amnion to form the chorio-amniotic membrane.Depending on the number of placentas, twin pregnancies are classified as dichorionic, if there are two chorionic cavities and therefore two placentas, or monochorionic, if there is only one chorionic cavity and the twins share a single placenta. Dichorionic twins therefore are independent anatomically as well as functionally in relation to each other, whereas twins with monochorionic placentation are hemodynamically connected through vascular anastomoses within the placenta (chorioangiopagus). Each dichorionic twin has its own placenta, chorionic cavity and amniotic cavity, similar to singleton pregnancies. Monochorionic twins, on the other hand, share a single placenta and may or may not share an amniotic sac.
In clinical practice, determination of chorionicity is relevant to all multiple pregnancies, as this is one of the most important factors that determines the prognosis of the pregnancy. Monochorionic twins are associated with higher rates of pregnancy loss, prematurity, congenital anomalies, intrauterine growth restriction and perinatal death compared to dichorionic twins.6 In addition, monochorionic placentation is associated with specific conditions including twin-twin transfusion syndrome, twin-reversed arterial perfusion sequence (acardiac twinning), abnormal placental sharing with selective intrauterine growth restriction, single intrauterine demise of one twin with cerebral hypoperfusion of the surviving twin and twin anemia-polycythemia sequence, which are all consequences of the shared circulation.3,6 In the setting of monoamnionicity, entanglement of the umbilical cords and conjoined twins are also well-recognised, although rare complications. Monochorionic twins also pose specific diagnostic and management challenges in cases of discordant malformation and selective termination of pregnancy or embryo reduction.2,3,6 Perinatal complications in pregnancies with monochorionic placentation and the corresponding management are discussed in the other chapters of this book.
Prenatal Determination of Chorionicity
In dichorionic pregnancies, chorionicity can be established by prenatal ultrasound as early as the twin pregnancy is identified sonographically by the presence of two or more gestational sacs. Monochorionic pregnancies, on the other hand, can only be diagnosed as such after more than one embryonic structure, such as multiple yolk sacs or embryos, are visualised within a single gestational sac. During each trimester of pregnancy, specific sonographic features are present that can be used to determine chorionicity.7 The first trimester, especially before the 11th week, is the optimal time to diagnose and classify twin pregnancies based on chorionicity and amnionicity. In a dichorionic pregnancy, two gestational sacs are clearly seen as distinct from each other with a thick interposing chorion and maternal decidua. However, as pregnancy progresses, this separation becomes less evident with the progressive increase in size of the gestational sacs and the corresponding compression of the dividing membrane between the sacs. Therefore, establishing chorionicity using this criterion becomes more difficult with advancing gestational age.
Early determination of chorionicity is especially relevant to pregnancies achieved by assisted reproductive techniques as they are at high risk for not only twin gestation but also for higher-order multiple pregnancies. Fortunately, these pregnancies are typically monitored with close serial sonographic evaluation beginning in the early first trimester by sonologists familiar with these types of pregnancies and accurate determination of chor- ionicity is successfully performed in most cases.7,8 In spontaneous pregnancies, on the other hand, the diagnosis of twins is often not made until the 11th to 13th week at the time of routine first-trimester ultrasound screening for chromosomal abnormalities and structural defects. These two periods have distinct ultrasound features based on their chorionicity and are analysed separately.
Early First Trimester
The first sonographic evidence of a gestational sac can be identified with transvaginal ultrasound at around the 4th to 5th week. It appears as a round, anechoic structure surrounded by a relatively thick echoic rim representing the developing chorion and maternal decidual reaction. At the 6th week, the first embryonic structures are visible within the sac, including the amnion and yolk sac. Later this week, the first evidence of an embryo appears as a small echoic pole in close relation to the wall of the yolk sac (the ‘engagement ring' sign). Definitive evidence of a viable embryo is the visualisation of cardiac activity within the fetal pole, which is detected using conventional real-time ultrasound with or without Doppler technology between the 6th and 7th week. In the 7th week, a living embryo can be clearly identified separate from the yolk sac and both the amniotic and chorionic cavities are visible.
Dichorionic twins: Dichorionicity can be detected using ultrasound from the moment the implanted gestational sacs are visualised. Using high-resolution transvaginal ultrasound, a dichorionic twin pregnancy is seen as the presence of two gestational sacs within the uterine cavity from the 4th to 5th week onwards. Each sac contains the same structures as the ones present in a developing singleton fetus. Rarely, heterotopic twins develop, the most frequent presentation being one intrauterine pregnancy and another ectopic pregnancy in the fallopian tube.2 During the 5th to 6th weeks, the yolk sac appears, and in the 6th to 7th weeks, an embryo can be visualised in each sac. Definite proof of chorionicity can be established at the time confident identification of live embryos is observed (Figure 3.3). All dichorionic twin pregnancies have two amniotic sacs and are by definition diamniotic. However, during the classification of twins, both descriptors (dichorionic and diamniotic) and also the number of fetuses should be used to clearly state the presence of two fetuses. As a dichorionic pregnancy can also occur in a triplet pregnancy, its placentation therefore should be classified as a dichorionic-triamniotic or dichorionic-diamniotic triplet pregnancy, indicating that one of the triplets has its own placenta and amniotic sac, whereas the other two are monochorionic and share a single placenta with two or one amniotic sacs, respectively.
Monochorionic twins: Monochorionic twins are frequently overlooked during the early first trimester. However, meticulous examination of the gestational sac can reveal the
https://doi.org/10.1017/9781108915038.003 Published online by Cambridge University Press
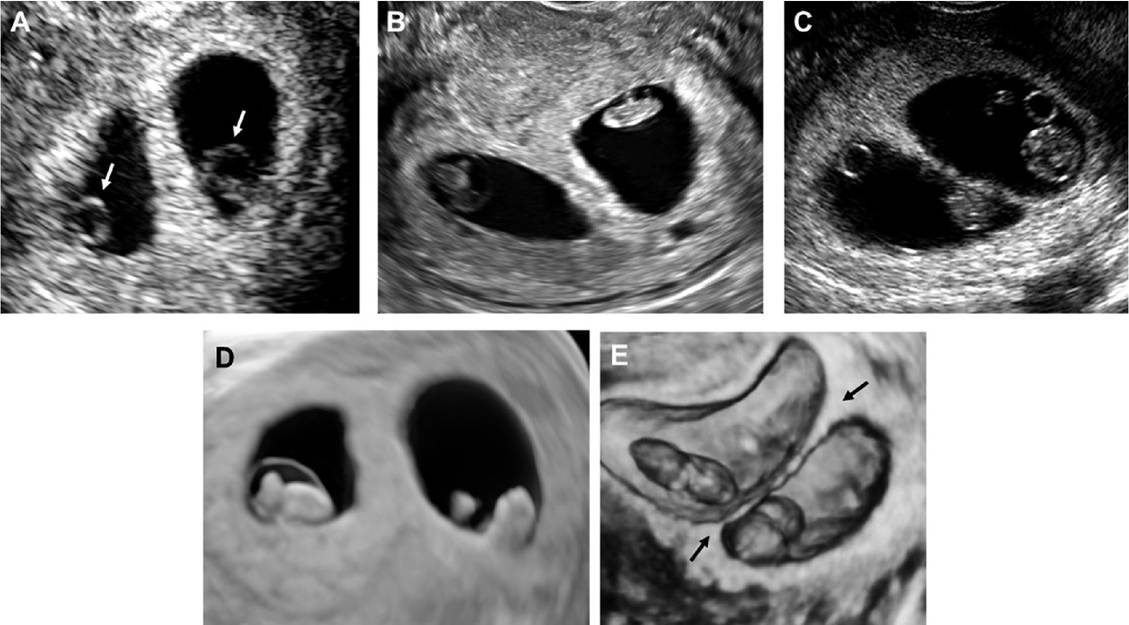
Figure 3.3 Representative early first-trimester ultrasound views of dichorionic-diamniotic twin pregnancies. (A) At 6 weeks 5 days, two gestationalsacs, each containing a yolk sac and an embryo (arrows), are clearly seen separated by thick echoic tissue representing the chorion and maternaldecidualreaction. (B) At 7 weeks 4 days, two embryos are seen in their own gestationalsacand separated by a thick septum. (C) At 8 weeks 6 days, each amniotic sac contains an embryo. The extra-amniotically located yolk sacs are also visualised. Note that the interposing chorion is getting thinner with advancing gestation, with the exception of the base of the membrane where the chorion remains thick, displaying the 'lambda' or 'twin peak' sign. (D) Three-dimensional ultrasound in the case shown in B. Two distinct gestationalsacs separated by a thick septum are seen. (E) Three- dimensionalultrasound in the case shown in C. Note that the 'lambda' sign is clearly seen at the two ends of the dividing membrane (arrows).
presence of a monochorionic twin pregnancy at the 6th to 7th week by detecting two different fetal poles within the same gestational sac. After the 7th week, the identification of two embryos sharing the same chorionic sac and having one or two amniotic cavities and yolk sacs becomes more evident (Figure 3.4). The criteria for the determination of amnio- nicity in these cases are described in the corresponding section that follows.
Late First Trimester
The period between the 11th and 13th weeks is an important window in which to diagnose twins and determine their chorionicity and amnionicity, especially in undiagnosed spontaneous twin pregnancies. If the diagnosis of twin pregnancy has been already made, this window also provides the opportunity to confirm the chorionicity assigned by previous examiners. The most predictive sonographic feature at this gestational age is the presence or absence of the chorionic tissue projection at the base of the dividing membrane (Figure 3.5). The presence of this projection, which is called the ‘lambda’ sign due to its close resemblance to the Greek letter λ, is particularly prominent at the site of contact between two fused placentas. Initially described in 1981 by Bessis and Papiernik,9 who should be credited as the first ones to determine chorionicity prenatally, it was subsequently also named the ‘twin peak’ sign by Finberg,10 who confirmed its reliability as pathognomonic of dichorionicity in the second- and third-trimester twin pregnancies. During the scan at the 11th to the 13th week, the lambda sign is easily identified in all dichorionic twin pregnancies regardless of the position of the placentas; at this gestational age, dichorionic placentas will display the lambda sign at the inter-twin membrane-placental junction whether they are fused or separate (Figure 3.6).11 The absence of the lambda sign, also known as the ‘T’ sign (Figure 3.7),7,8 means that there is no interposing chorion and that therefore the dividing membrane is formed only by the two amnions, indicating monochorionicity (Figure 3.8). Several studies have confirmed that the use of the lambda sign alone, classified subjectively as present or absent, is almost 100% accurate at determining chorionicity in twin pregnancies at this gestational age. Placental location is also an important factor that should be considered; if anatomically separate placentas are observed during the scan, dichorionicity can also be established. However, due to the size of the placentas and the relatively small uterine cavity at this gestational age, the vast majority of placentas are positioned close to each other, which can give dichorionic placentas the false appearance of a single placenta rather than fused placentas. Thickness of the dividing membrane is also another ultrasound feature, but this relies on subjective rather than objective assessment because a cut-off in the first trimester has not been established. Finally, although fetal sex can usually be determined in the first trimester, the accuracy of sex assignment is not sufficient to be used as a reliable factor in determining dichorionicity if presumably opposite-sex twins are suspected.
Second and Third Trimesters of Pregnancy
Determination of chorionicity in the second and third trimesters relies on several sonographic features, some of which are similar to the ones already present at the scan performed at the 11th to 13th week. These include determination of fetal sex, examination of the location and number of placentas, assessment of the inter-twin membrane- placental junction for the presence or absence of the lambda versus the T sign and evaluation of the thickness of the dividing membrane (Figure 3.9).7 As all of these
https://doi.org/10.1017/9781108915038.003 Published online by Cambridge University Press
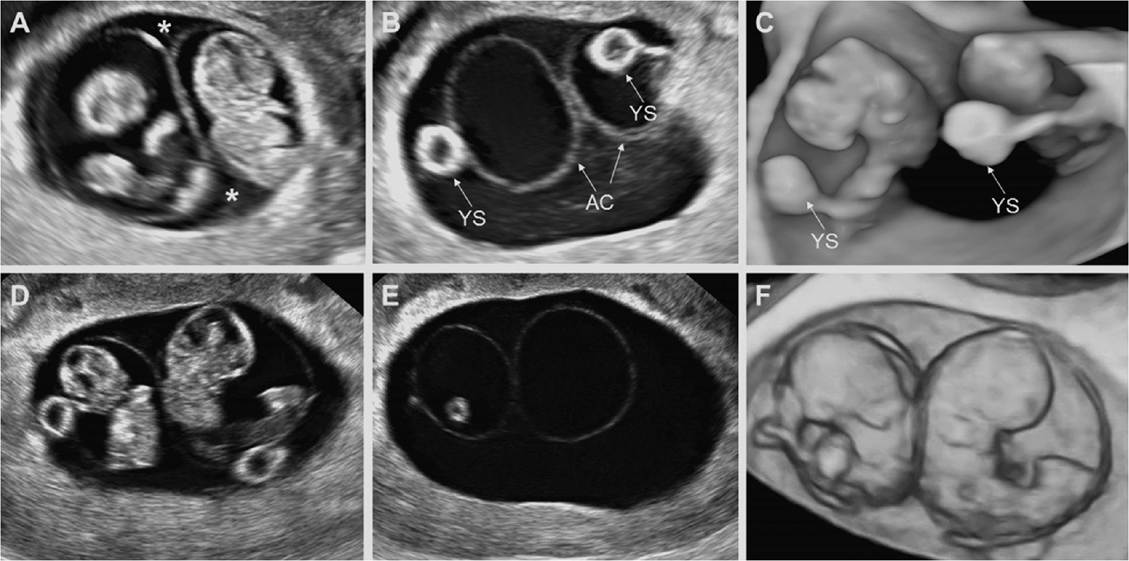
Figure 3.4 Representative early first-trimester ultrasound views of monochorionic-diamniotic twin pregnancies. (A) At 7 weeks 5 days, two embryos in separate amniotic cavities are seen sharing a single chorionic sac. The 'black lambda' sign is displayed at the corners of the chorionic sac (asterisks). (B) Two amniotic cavities (AC) and two yolk sacs (YS) are clearly seen. Note that there is no interposing chorion between the amnions. (C) Three-dimensionalultrasound shows the two embryos in two distinct amniotic sacs. Although the thin dividing membrane is hard to visualise with this technology, the presence of two yolk sacs (YS) is highly suggestive of diamnionicity. (D, E, and F) Similar sonographic findings at 9 weeks 3 days in a different monochorionic-diamniotic twin pregnancy. Note the dividing membrane with no interposing chorion.
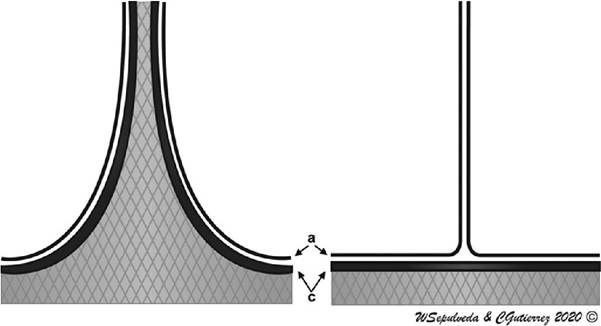
Figure 3.5 Schematic representation of the inter-twin membrane-placentaljunction in dichorionic-diamniotic (left panel) and monochorionic-diamniotic (right panel) twin pregnancies. In dichorionic-diamniotic twin pregnancy, there is a triangular projection of chorionic tissue into the base of the dividing membrane ('lambda' sign). In monochorionic-diamniotic twin pregnancy, the projection is absent as there is no interposing chorion between the amnions ('T' sign). a, amnion; c, chorion.
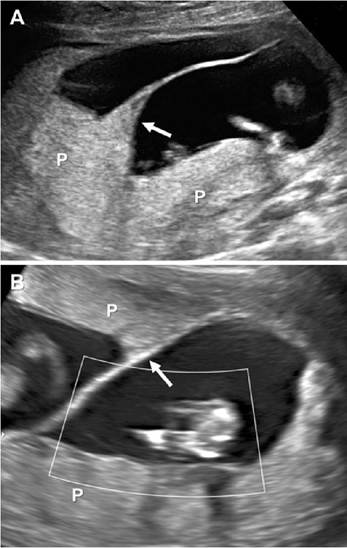
Figure 3.6 Late first-trimester ultrasound views of dichorionic-diamniotic twin pregnancies. At the intertwin membrane-placentaljunction, the chorion is thicker than in the rest of the dividing membrane, giving this area the appearance of the Greek letter λ ('lambda' sign, arrows). (A) Fused dichorionic placentas giving the appearance of a single placentalmass. (B) Separate dichorionic placentas. Note the thick dividing membrane between the twins. P, placenta.
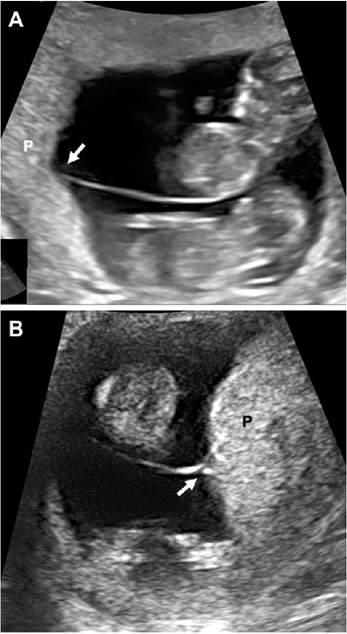
Figure 3.7 Late first-trimester ultrasound views of monochorionic-diamniotic twin pregnancies. At the inter-twin membrane-placentaljunction, the chorionic projection ('lambda' sign) is absent. The amnions arise perpendicularly from the fetalsurface of the placenta, giving this area the appearance of the letter T ('T' sign, arrows). (A) Single placenta with the'T' sign, indicative of monochorionicity. (B) 'T' sign at the base of the membrane. Note the thin dividing membrane between the twins P, placenta.
techniques have limitations, it is important to assess as many of these features as possible during the obstetric scan.
• Determination of fetal sex: Sonographic determination of fetal gender is almost 100% accurate after the 13th week. If the fetuses are of different sex, there is compelling evidence of dizygosity and therefore of a dichorionic twin pregnancy. Sex discordance in monochorionic twins is extremely rare, but it is possible in a heterokaryotypic twin pregnancy. Therefore, the detection of opposite-sex twins in the context of
a sonographically identified monochorionic placentation should prompt genetic testing of both twins to evaluate for heterokaryotypic twinning. When same-sex twins are detected, additional assessment is required as chorionicity cannot be determined; although 100% of monochorionic twins are of the same sex, so are theoretically 50% of dichorionic twins.
• Determination of the number of placentas: With careful examination of the location of the placenta(s), it is possible to identify those that are separate from those that conform a single placental mass. Separate placentas can be taken as strong evidence of
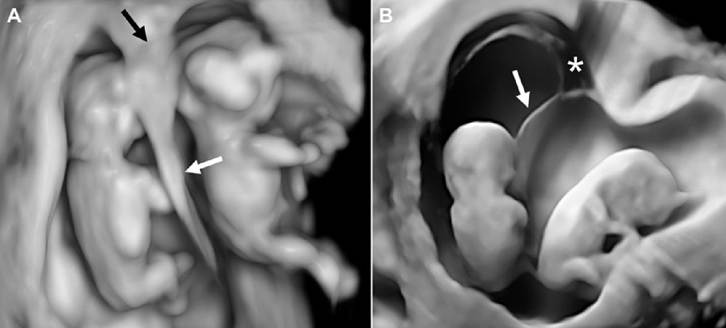
Figure 3.8 Surface-rendering three-dimensionalultrasound views of first-trimester twin pregnancies show the differences between dichorionic-diamniotic and monochorionic-diamniotic twins at the levelof the dividing membrane (white arrows). (A) In dichorionic twins, the dividing membrane is thicker than in monochorionic- diamniotic twins and the 'lambda' sign is clearly seen at the inter-twin membrane-placental junction (black arrow). (B) In monochorionic-diamniotic twins, the dividing membrane is thin and is devoid of interposing chorion, which is also reflected at the levelof the chorionic cavity (asterisk). (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
a dichorionic twin pregnancy. However, due to the large size of the placentas, many dichorionic placentas that are in close proximity fuse with growth and can be mistaken for a single monochorionic placenta. Dichorionic placentas may be so tightly fused that even the pathologist may be unable to separate them postnatally. Monochorionic placentation therefore cannot be necessarily diagnosed based on the identification of a single placental mass.
• Assessment of the inter-twin membrane-placental junction: Sonographic examination of the area where the dividing membrane arises from the fetal surface of the placenta provides important information about chorionicity, especially during the first and second trimesters of pregnancy.7’8’10’11 In dichorionic pregnancies, the interposing chorion is significantly thicker at this location immediately adjacent to the placenta compared to the rest of the dividing membrane (Figure 3.10). This prominence at the base of the membrane can be identified in almost all dichorionic twins as a sonographically echoic structure resembling a pyramid, known as the lambda or twin peak sign.7’8’10’11 However, the prominence of the lambda sign decreases as pregnancy progresses; a longitudinal study reported that after the 20th week, the sign was no longer seen in 26% of pregnancies with separate placentas and in 7% of pregnancies with fused placentas.12 Therefore, while the lambda sign is easily detected at the scan taken in the 11th to 13th week and can be confidently used to determine chorionicity in the first trimester, its absence should not be used in the second and third trimesters with the same predictive value.11’12 Monochorionic placentation, on the other hand, does not have an interposing chorion between the amnions, so the dividing membrane is thin starting from the point at which it arises from the placenta and has the same thickness through its entire length. In these cases, the inter-twin membrane-placental junction appears as a perpendicular angle resembling the shape of the letter T, hence the name of T sign to describe this feature.7’8
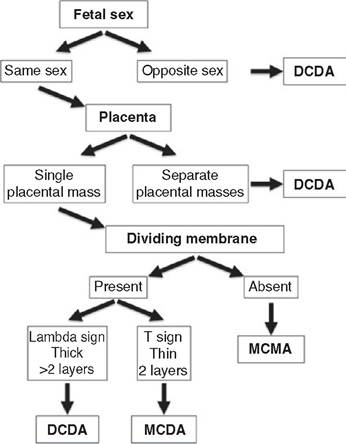
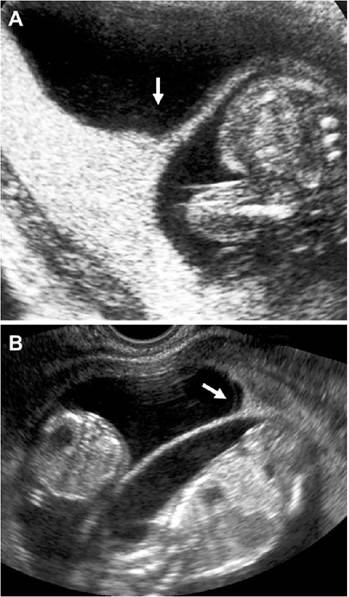
Figure 3.9 Flowchart diagram to determine chorionicity and amnionicity in the second and third trimesters. DCDA, dichorionic-diamniotic; MCDA, monochorionic-diamniotic; MCMA, monochorionic- monoamniotic
Figure 3.10 The 'lambda' sign in second-trimester dichorionic twin pregnancies (arrows). (A) The echoic projection of chorionic tissue at the levelof the intertwin membrane-placental junction is clearly seen. The dividing membrane is also thick due to the interposing chorion. (B) With advancing gestation, the thickness of the membrane as wellas the prominence of the 'lambda' sign decrease.
• Thickness of the dividing membrane: In dichorionic placentation, the dividing membrane has four layers, two amnions externally and two layers of interposing chorion, which may be fused. This composition makes the membrane thicker in dichorionic-diamniotic placentation than in cases of monochorionic-diamniotic placentation, in which there are only two amnions without interposing chorion (Figure 3.5). The dividing membrane thickness can be measured by ultrasound under adequate magnification and image settings, ideally in a parallel view in relation to the ultrasound beam.7 Although the dividing membrane is thinner in monochorionic- diamniotic placentation, the absence of a clearly defined cut-off thickness to differentiate between monochorionic versus dichorionic twins and lack of a standardised method to measure membrane thickness limit the usefulness of this technique. Although a cut-off thickness of 2 mm in the second and third trimesters has been proposed, measurements have a high inter- and intra-observer variability and the membrane thickness becomes difficult to assess as pregnancy progresses.7 An additional sonographic feature is the number of layers of the dividing membrane.7 Using high-resolution ultrasound, more than two membranes may be visible, but it is usually difficult to visualise the four layers of dichorionic placentation in clinical practice. Due to these limitations, this technique has not gained wide acceptance in the ultrasound community. Another simple sign, particularly useful in the third trimester, is the detection of splitting membranes, known as the ‘split membrane' sign. This represents local accumulation of fluid within the membranes and is a characteristic of dichorionic placentation, as it has not been described in monochorionic-diamniotic twin pregnancies. It was noted as a third- trimester sign of dichorionic-diamniotic twins, although it occasionally can be detected in second-trimester twins (Figure 3.11).
Amnionicity
The amniotic cavity is the space filled with amniotic fluid that surrounds the embryo and fetus during intrauterine development. This cavity is enclosed by the amnion, a thin membrane measuring less than 0.5 mm. In multiple pregnancies, the term ‘amnionicity' is used to refer to the number of amniotic cavities. This terminology comes from ‘amnion' (Greek amnos, ‘little lamb', ‘vase in which the blood of a sacrifice was caught', ‘membrane around a fetus'). In clinical practice, determination of amnionicity is only relevant to

Figure 3.11 The ‘split membrane' sign characteristic of a dichorionic-diamniotic placentation at 25 weeks (arrow). monochorionic twin pregnancies, as all dichorionic twin pregnancies have two amniotic sacs and are therefore diamniotic.
Based on the number of amniotic cavities, monochorionic twin pregnancies are classified into two groups: diamniotic and monoamniotic. In monochorionic-diamniotic twins, each twin has its own amniotic cavity whereas monochorionic-monoamniotic twins share a single amniotic cavity. In the latter condition, entanglement of the umbilical cords invariably occurs as the fetuses freely move within the amniotic cavity and the umbilical cord placental insertion sites remain fixed. Continuous fetal movement may result in entwining of the umbilical cords and a subsequent cord accident. A unique form of monochorionic-monoamniotic twin pregnancy is the development of conjoined twins, in which the inner cell mass only partially splits after 12 days after conception, resulting in different degrees of fusion at the level of head (cephalopagus), chest (thoracopagus), abdomen (omphalopagus) or pelvis (ischiopagus).2 The ultrasound diagnosis of conjoined twins relies on the context of fused body parts in the setting of a monochorionic- monoamniotic placentation. In the rostral type of conjoined twins, which accounts for around 50% of the cases, there is a single umbilical cord so cord entanglement is not possible. In the other types of conjoined twins, cord entanglement is possible but uncommon due to the restriction of movement of the two fetuses relative to each other.
Prenatal Determination OfAmnionicity
Diamniotic twins: In monochorionic twins, amnionicity can be determined by direct identification of the inter-twin amniotic membrane, which appears sonographically at around the 8th week. This inter-twin membrane is characteristically thin throughout pregnancy and is formed by the apposition of the two amnions, one from each twin, and lacks interposing chorion. As the amniotic cavities increase in size over time, a progressively smaller chorionic cavity develops, which is sonographically visualised as an anechoic pyramid-shaped space (the ‘black lambda' sign). Two yolk sacs located within the single chorionic cavity but outside the amniotic cavity can be visualised (Figure 3.12). Sometimes they are adjacent to each other and have a characteristic appearance known as the ‘eight' or ‘spectacles' sign (Figure 3.13). In the second and third trimesters, determination of dia- mnionicity is straightforward with visualisation of the inter-twin membrane separating the two fetuses in both dichorionic-diamniotic and monochorionic-diamniotic pregnancies, although the location of the membrane occasionally may be more difficult to identify with advancing gestation and in ases of severe oligohydramnios in one of the twins.
Monoamniotic twins: By definition, monochorionic-monoamniotic twins lack an intertwin dividing membrane. This type of twinning occurs in less than 1% of monochorionic twin pregnancies.2 As the dividing amniotic membrane is confidently visualised only after the 8th week, other sonographic landmarks have been suggested to determine amnionicity in very early gestation. There is evidence that counting the number of yolk sacs helps differentiate between monochorionic-diamniotic and monochorionic-monoamniotic twins when the dividing membrane is not visualised or difficult to ascertain. Bromley and Benacerraf13 were the first to suggest the use of the number of yolk sacs to determine amnionicity before the 8th week. In their review of 22 monochorionic twin pregnancies between the 6th and 9th week, they noted that in 19 of the 20 (95%) diamniotic twin pregnancies, two yolk sacs were seen. The remaining case was first examined at 6 weeks
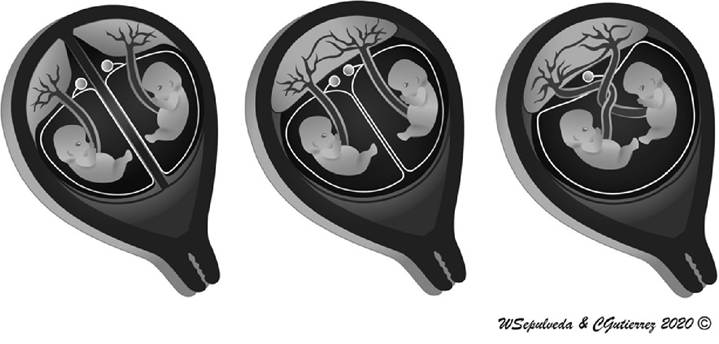
Figure 3.12 Schematic representation of the relation between yolk sac number and amnionicity in early pregnancy. In alldichorionic-diamniotic twin pregnancies, the yolk sacs are separated by chorionic tissue (left panel). In monochorionic-diamniotic twin pregnancies, two yolk sacs are present in the single chorionic cavity (middle panel). In monochorionic-monoamniotic twin pregnancies, only one yolk sac is usually identified (right panel). (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
when only one yolk sac was visualised; however, at re-examination at 8 weeks, two yolk sacs were clearly identified. In contrast, in the remaining two monoamniotic twin pregnancies examined, only one yolk sac was visualised (Figure 3.14). Although this observation was confirmed by the other authors, subsequent reports questioned the use of this technique; though mainly based on single case reports, two yolk sacs were documented in several pregnancies which ultimately proved to be monochorionic-monoamniotic. More recently, large series have shown compelling evidence that counting the number of yolk sacs is not a reliable technique for determining amnionicity in early monochorionic pregnancies. Fenton et al.14 reviewed the number of yolk sacs in 38 monochorionic-monoamniotic twin pregnancies and found only one yolk sac in 26 (68%) and two yolk sacs in 12 (32%) of the cases. In the review of their own experience as well as the literature, a total of 22 cases of monochorionic-monoamniotic twin pregnancies with two yolk sacs were documented in early pregnancy. Therefore, additional sonographic follow-up examinations are required to provide a confident diagnosis of monoamnionicity.
From the late first trimester onwards, the dividing membrane can be clearly visualised sonographically between the fetuses in most cases. This thin structure is better identified using transvaginal ultrasound in the first trimester and by abdominal sonography in the second and third trimesters. In order to enhance visibility, it is advised that the ultrasound beam should insonate the membrane perpendicularly, ideally as close to 90 degrees as possible. In advancing monochorionic pregnancies, the visualisation of the dividing membrane should be taken as a definitive proof of diamnionicity. If the dividing membrane is not identified, every effort should be made to visualise the umbilical cords for entanglement. Although this can be identified with conventional two-dimensional ultrasound, colour Doppler imaging can provide
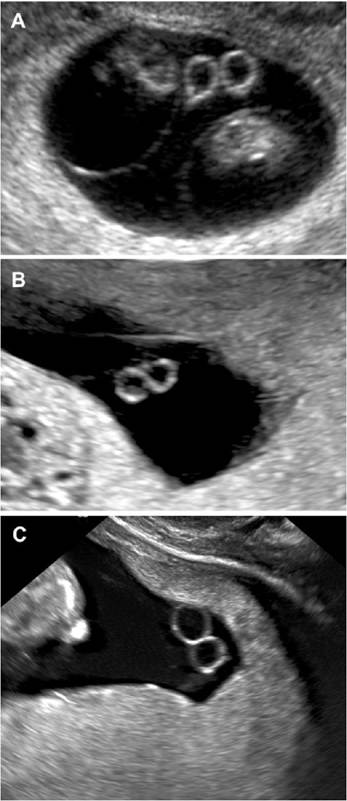
Figure 3.13 Amnionicity in first-trimester monochorionic-diamniotic twins. Two yolk sacs are seen in close proximity to each other within the single chorionic cavity (the 'spectacles' sign). (A) At 9 weeks. (B) At 11 weeks. (C) At 12 weeks.
compelling evidence of umbilical cord entanglement, especially later in pregnancy (Figure 3.15).
Pseudo-amnionicity: Spontaneous rupture of the dividing membranes in dichorionic- diamniotic or monochorionic-diamniotic twins is exceedingly rare. In contrast, iatrogenic amniotomy secondary to invasive procedures such as diagnostic or therapeutic amniocentesis and fetoscopic procedures is well documented in the literature.2 In all of these cases, the history of an invasive procedure and the identification of membranes floating freely within the amniotic cavity make the diagnosis straightforward. Umbilical cord entanglement and amniotic band syndrome are well-known complications occurring in the context of pseudo- amnionicity.
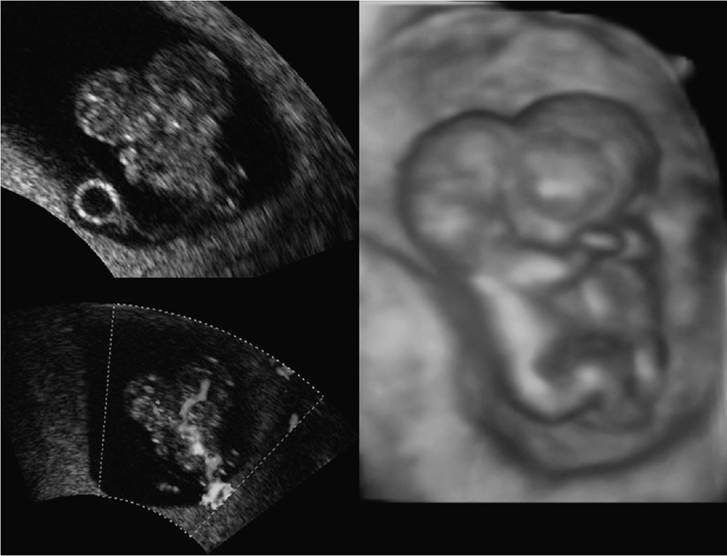
Figure 3.14 Amnionicity in early first-trimester monochorionic-monoamniotic twins. In this set of monochorionic- monoamniotic conjoined twins (thoracopagus type), there is only one yolk sac in the common chorionic cavity. (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
Triplets and Other Higher-Order Multiple Pregnancies
Higher-order multiple pregnancy is defined as a pregnancy with three or more fetuses. The number of fetuses is an independent prognostic factor for pregnancy outcome; the greater the number of fetuses, the higher the risk for the pregnancy. Spontaneous higher-order multiple pregnancies are rare. However, the transfer of multiple embryos in in vitro fertilisation patients resulted in an excessively high prevalence of higher- order multiple pregnancies until single embryo transfer became a more common standard of care in patients with infertility. Determination of chorionicity and amnio- nicity in higher-order multiple pregnancies has tremendous importance for the subsequent management of the pregnancy. If a set of monochorionic fetuses is present, the pregnancy risks are further increased from that based merely on the number of fetuses due to the unique risks associated with monochorionicity. When embryo reduction is being considered in this situation, the entire monochorionic set is often targeted to maximise the risk reduction conferred by the procedure particularly since reduction of only one monochorionic fetus must be avoided due to the associated risks for the surviving co-twin.2,8
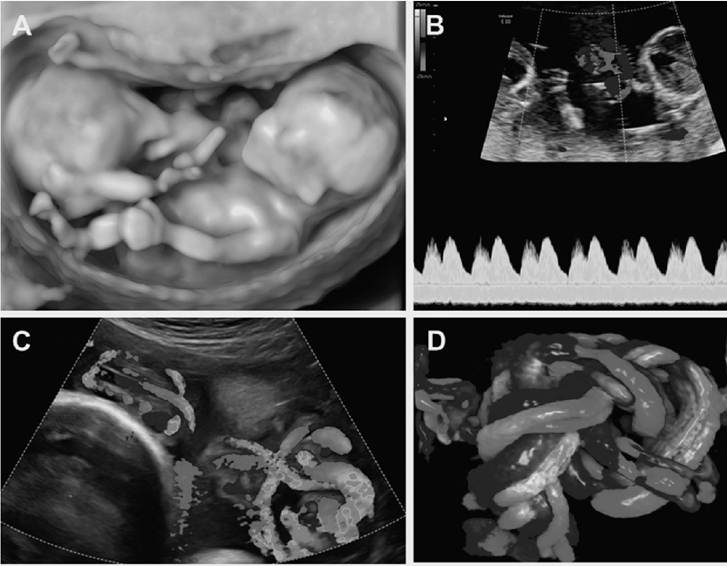
Figure 3.15 Monochorionic-monoamniotic twin pregnancy at 12 weeks 6 days. (A) Three-dimensionalultrasound shows two fetuses lying close together. The amniotic membrane was not identified. (B) Entanglement of the Umbilicalcords confirmed monoamnionicity. SpectralDoppler ultrasound demonstrates the two cardiac beats in the area of entanglement of the umbilicalcords. (C) At 30 weeks, entanglement of the umbilicalcords is evident as visualised with colour flow mapping. D, Three-dimensionalHD live flow mapping demonstrates entanglement of the umbilicalcords. (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
Determination of chorionicity and amnionicity in this setting is often performed early in pregnancy, at which time transvaginal and transabdominal imaging approaches are usually complementary. The first step is determining the number of fetuses. The second is establishing the placentation of each fetus in relation to the surrounding fetuses.2,8 The same criteria used in twin pregnancies apply to each fetus from a higher-order multiple pregnancy, with careful evaluation to determine if a monochorionic set is present. As determining the number of placentas can be technically challenging, chorionicity is most commonly assessed based on the thickness of the dividing membrane in conjunction with the assessment of the inter-twin membrane-placental junction. In triplet pregnancies, assessment of the area where the amniotic sacs converge provides information on chorionicity.15 This area, known as the ‘Ypsilon’ zone or ‘Mercedes' sign (Figure 3.16), has been shown to be a reliable criterion to differentiate trichorionic from dichorionic and monochorionic triplet pregnancies. Nevertheless, it is important that all of these higher-order multiple pregnancies be managed at tertiary referral centres.
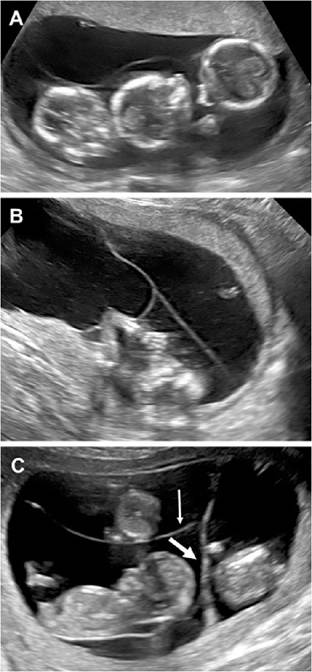
Figure 3.16 Assessment of the 'Ypsilon' zone to determine chorionicity and amnionicity in higher-order multiple pregnancies. (A) Threefetuses are seen at 14 weeks. There was a single placentalmass and the dividing membranes were subjectively thin. (B) Evaluation at the area where the three amniotic cavities joined demonstrates a thin membrane with similar thickness, suggesting monochorionicity. (C) For comparison, a dichorionic-triamniotic triplet pregnancy at 12 weeks is presented. Note that one membrane is thicker (thick arrow) in comparison with the other (thin arrow), suggesting the presence of a monochorionic set.
Acknowledgments
This work was supported by an unrestricted research grant from the ‘Sociedad Profesional de Medicina Fetal ‘Fetalmed’ Ltda., Chile.
Key Points
• Monozygotic twins are genetically identical but can be associated with dichorionic- diamniotic, monochorionic-diamniotic or monochorionic-monoamniotic placentation depending on the timing of embryonic splitting.
• Dizygotic twins are genetically different and are associated with only dichorionic- diamniotic placentation.
• The optimal time for accurate classification of multiple pregnancy is during the first trimester, ideally before the 11th week of gestation.
• Dichorionicity can be sonographically diagnosed in early pregnancy with the presence of two gestational sacs.
• The diagnosis of monochorionicity requires visualisation of multiple embryonic structures within a single gestational sac.
• Key features that should be assessed to determine chorionicity consist of: fetal sex, number of placentas, appearance of the inter-twin membrane-placental junction and thickness of the inter-twin dividing membrane.
• The ‘lambda’ or ‘twin peak' sign is characteristic of dichorionic placentation and the ‘T sign' is characteristic of monochorionic placentation.
• Monoamnionicity is rare and is often difficult to diagnose in the early first trimester due to the thinness of the amniotic membrane. If a dividing membrane cannot be confidently identified later in the pregnancy, evaluation for umbilical cord entanglement should be performed.
References
1. Moise KJ Jr, Johnson A. There is NO diagnosis of twins. Am J Obstet Gynecol 2010;203:1-2.
2. Blickstein I, Keith LG (eds.). Multiple Pregnancy: Epidemiology, Gestation & Perinatal Outcome. 2nd Edition. New York: Informa Healthcare, 2005.
3. Khalil A, Rodgers M, Baschat A, Bhide A, Gratacos E, Hecher K, et al. ISUOG Practice Guidelines: role of ultrasound in twin pregnancy. Ultrasound Obstet Gynecol 2016;47:247-63.
4. McNamara HC, Kane SC, Craig JM, Short RV, Umstad MP. A review of the mechanisms and evidence for typical and atypical twinning. Am J Obstet Gynecol 2016;214:172-91.
5. Norwitz ER, McNeill G, Kalyan A, Rivers E, Ahmed E, Meng L, et al. Validation of a single-nucleotide polymorphism-based non-invasive prenatal test in twin gestations: determination of zygosity, individual fetal sex, and fetal aneuploidy. J Clin Med 2019;8 (7).pii:E937.
6. Gratacos E, Ortiz JU, Martinez JM.
A systematic approach to the differential diagnosis and management of the complications of monochorionic twin pregnancies. Fetal Diagn Ther 2012;32:145-55.
7. Jha P, Morgan TA, Kennedy A. US evaluation of twin pregnancies: importance of chorionicity and amnionicity. RadioGraphics 2019;39:2146-66.
8. Monteagudo A, Timor-Tritsch IE, Sharma S. Early and simple determination of chorionic and amniotic type in multifetal gestations in the first fourteen weeks by high-frequency transvaginal
ultrasonography. Am J Obstet Gynecol 1994;170:824-9.
9. Bessis R, Papiernik E. Echographic imagery of amniotic membranes in twin pregnancies. In Twin Research 3: Twin Biology and Multiple Pregnancy, Gedda L, Parisi P, Nance WE (eds.). New York: Alan Liss, 1981;183-7.
10. Finberg HJ. The ‘twin peak’ sign: reliable evidence of dichorionic twinning.
J Ultrasound Med 1992;11:571-7.
11. Sepulveda W, Sebire NJ, Hughes K, Odibo A, Nicolaides KH. The lambda sign at 10-14 weeks of gestation as
a predictor of chorionicity in twin pregnancies. Ultrasound Obstet Gynecol 1996;7:421-3.
12. Sepulveda W, Sebire NJ, Hughes K, Kalogeropoulos A, Nicolaides KH. Evolution of the lambda or twin-chorionic peak sign in dichorionic twin pregnancies. Obstet Gynecol 1997;89:439-41.
13. Bromley B, Benacerraf B. Using the number of yolk sacs to determine amnionicity in early first trimester monochorionic twins. J Ultrasound Med 1995;14:415-19.
14. Fenton C, Reidy K, Demyanenko M, Palma-Dias R, Cole S, Umstad MP. The significance of yolk sac number in monoamniotic twins. Fetal Diagn Ther 2019;46:193-9.
15. Sepulveda W, Sebire NJ, Odibo A, Psarra A, Nicolaides KH. Prenatal determination of chorionicity in triplet pregnancy by ultrasonographic examination of the ipsilon zone. Obstet Gynecol 1996;88:855-8.