15.7 CHRONIC LIVER DISEASE
TABLE 15.11: Clinical indicators of chronic liver disease
Chronic liver disease (CLD) denotes persistent hepatic dysfunction for gt;6 months, with or without clinical symptoms, often culminating into irreversible or endstage hepatic disease.
Etiology: HBV is the commonest cause of CLD in Indian children, followed by cholestatic syndromes and autoimmune liver disease (Table 15.10).
Pathologically, CLD may be classified as:
• Chronic persistent hepatitis, without jaundice and with mild/moderate elevation of liver enzymes. Hepatocellular inflammation in these cases is limited within portal triads.
• Chronic lobular hepatitis, more moderate disease with mixed intra-portal as well as centri-lobular inflammation. Mild jaundice is common.
• Chronic active hepatitis, with intra-portal and lobular inflammation as well as destruction of normal liver architecture. Definite signs of CLD and portal hypertension are present and most survivors progress to cirrhosis.
• Cirrhosis is the end-stage, characterized by—(a) shrunken liver, (b) extensive fibrosis, (c) destroyed liver architecture and (d) nodule formation.
Signs of impaired hepatic metabolism
• Icterus (s/o impaired bilirubin metabolism)
• Edema (s/o impaired protein metabolism)
• S/o fat malabsorption
- Growth failure, steatorrhea, phrynoderma
• S/o Fat-soluble vitamin deficiency
- Xerophthalmia (Vitanin A)
- Rickets (Vitamin D)
- Bleeding: epistaxis, GIT bleeds (Vitamin K)
• S/o impaired steroid metabolism
- Spider nevi, palmar erythema, gynecomastia
S/o Portal hypertension
• Splenomegaly
• Ascites (also due to hypoproteinemia)
• Others: Esophageal varices, caput medussae
S/o Cholestasis
• Clay-colored stools
• Pruritis
S/o Primary disease
• Autoimmune: Arthropathy, hemolytic anemia, rash
• Wilson disease: KF ring, CNS signs
S/o Impending liver failure
• Altered behavior and sleep pattern
• Fetor hepaticus
• Flapping tremors
S/o: Signs of.
Laboratory investigations aim to assess and monitor the extent of liver damage as well as to identify the etiology and include:
• To assess liver functions:
- Liver function tests
- Coagulation profile
- Radionuclide liver scan
- Ultrasonography
- Esophagoscopy for varices
• To identify etiology:
- Liver biopsy
- Serology, e.g. viral markers, autoantibodies
- Selective tests for specific metabolic defects Management of CLD includes specific therapy for primary cause, as well as supportive therapy to prevent and treat complications. Most cases can be managed at home after initial evaluation, though intermittent hospitalizations are often necessary to treat complications. Important supportive measures include:
• Nutritional management: Diet in CLD should provide 120-150% of caloric requirements with ~50% as carbohydrates, 25-30% as fats and rest as good-quality proteins. Medium chain triglycerides are preferred as fats, which do not require bile for absorption. Protein restriction (~1 gm/kg/d) is necessary only in cases with impending liver failure, while salt-restriction is advised in presence of ascites.
All cases should be supplemented with fat-soluble vitamins-vitamin A (5000-10000IU#8725;day), vitamin D (2000-5000 IU#8725;day), vitamin K (2-5 mg/week) and vitamin E (15-25 IU#8725;kg#8725;day).
• Management of ascites: Ascites in CLD is contributed by portal hypertension as well as hypoproteinemia and must be managed by:
- Dietary sodium restriction to maximum of 5 gm/ day. Fluid restriction is unnecessary, except in hyponatremia.
- Diuretic therapy, preferably with potassium-sparing spirolactone (PO 1-3 mg/kg/d). Loop diuretics or thiazides are used in severe cases.
- Abdominal paracentesis is required in large ascites with respiratory embarrassment. Amount of tapped fluid at one sitting should not exceed 10-15% of body weight, to prevent hypovolemia. Simultaneous administration of albumin or plasma expanders is advisable in large-volume paracentesis.
• Management of bleeding: Intermittent bleedings is common in CLD due to esophageal varices or vitamin K deficiency and should be managed according to the cause and severity, with blood transfusions, vitamin K therapy and endoscopic therapy, whenever indicated. (Ch 15.9).
• Management of hepatic failure: All cases should be periodically monitored for impending liver failure and managed accordingly (Ch 15.5).
• Specific management includes use of penicillamine in Wilson disease, Entecavir or Sofosbuvir/Velpatasvir in HBV or HCV respectively and steroids in autoimmune hepatitis, discussed later in this chapter.
• Liver transplant is last resort in cases with poor response to above measures and repeated hospitalizations. However, it is contraindicated in—(a) multisystemic metabolic disorders, (b) metastatic malignancies, and (c) during acute hepatic failure. Outcome of liver transplant depends on primary disease, though overall 5-year survival is gt;50-60%. Complications, e.g. graft-rejection, opportunistic infections and reappearance of disease are common.
Outcome of CLD depends on primary etiology and extent of liver damage. Most cases of chronic persistent or lobular hepatitis recover spontaneously. Chronic active hepatitis has poorer prognosis with eventual development of cirrhosis and occasionally, secondary carcinoma. Many patients may also develop hepatorenal syndrome.
Hepatopulmonary syndrome is a triad of: (a) chronic liver disease or portal hypertension, (b) wide alveolar- arteriolar gradient with/out hypoxemia, and (c) intrapulmonary vascular dilatations. It presents with progressive hypoxia, cyanosis and clubbing, with echocardiography suggestive of intrapulmonary shunting. Liver transplant is required in all cases.
Some important causes of CLD are discussed here in greater details:
Chronic hepatitis B infection (HBV), defined as persistence of HBsAg positivity for gt; 6 months, is the one of the commonest causes of CLD in Indian children, accounting for gt;40% cases.
About 3-7% of Indian population is HbsAg positive (carrier), of which ~35-40% are likely to develop CLD.Three different phases have been described in natural course of HBV infection:
Immune tolerance phase with active viral replication (high HBV-DNA levels in millions) but minimum liver damage (normal ALT). While HBsAg and HBeAg are positive, anti-HBeAg antibodies are absent.
Immune clearance phase after many years with clearance of infection (reduced HBV-DNA levels) but progressive liver injury with/without symptoms (elevated ALT). Serology continues to be same with positive HBsAg and HBeAg and negative Anti-HBeAg antibodies.
Inactive carrier phase with resolution of liver injury (normal ALT) and infection (very low HBV-DNA levels) as well as reversal of HBe serology, i.e. HBeAg negativity with presence of anti-HBeAg antibodies. Most of these cases remain HBsAG positive despite being asymptomatic carriers, before turning HBsAg negative after 15-20 years.
Diagnosis of chronic HBV infection depends on: (a) clinical evaluation with Liver function tests, (b) serology including quantitative HBV-DNA, and (c) liver biopsy in cases with elevated ALT levels, for staging of disease. All these cases should also be tested for HCV and HIV due to common mode of infection.
Management: As per recent guidelines, these cases are divided into two groups-those with chronic HBV infection (normal ALT) and those with chronic HBV hepatitis (raised ALT), second group needing liver biopsy.
All cases with chronic HBV Hepatitis having persistent elevation of liver enzymes and/or evidence of active disease on liver biopsy need treatment under expert guidance with:
• Subcutaneous interferon (5-10 million units/m2 thrice weekly) in children lt; 2 years or Pegylated interferon- 2a/b in older children of 2-18 years, for 6-10 months to inhibit viral protein synthesis.
• Oral antivirals, e.g. Entecavir (0.5-1 mg/day) or Lamivudine (3 mg/kg/day) in children aged -2 years and Tenofovir (300 mg OD) or Adefovir (10 mg OD) in adolescents gt;12 years, for 1-8 months.
Both groups of drugs may be used concurrently or sequentially in different regimens. Treatment should continue till normalization of liver function tests, undetectable HBV-DNA or HBeAg and resolution of histopathology. Success rate is ~ 40-60%.
Autoimmune hepatitis (AIH) is responsible for ~10% cases of CLD in children, characterized by:
• Chronic hepatocellular inflammation on biopsy,
• Presence of liver-specific autoantibodies, and
• Co-existing autoimmune disorders, e.g. arthropathy, rash, hemolytic anemia, thyroiditis, etc.
• Response to immunosuppressive therapy
Etiology: Although autoimmune in origin, exact triggers are unknown, probably related to genetic predisposition or preceding viral/drug exposure.
Pathologically, liver biopsy reveals distorted hepatic architecture of variable severity, including—(a) inflammatory infiltrates, (b) piecemeal and bridging hepatic necrosis, (c) bile duct epithelial injury, and (d) interface hepatitis.
Clinically, AIH predominantly presents in young females with three different presentations:
a. Acute hepatitis like presentation in 3-0%, rapidly progressing to AHF;
b. Insidious-onset liver disease with waxing and waning course in another 3-0%
c. Chronic liver disease with complications, e.g. ascites and portal hypertension in 1-0%
Extrahepatic manifestations, e.g. arthritis, vasculitis, nephritis, Coombs-positive anemia, and rash are not uncommon.
Diagnosis rests on liver biopsy and serological studies. According to the type of autoantibodies, AIH is divided into type I in 6-0% (ANA/SMA antibody positive), type lI in 2-0% (LKM1 antibody positive) and type III (SLA antibody positive, in young females). Hypergammaglobulinemia is common with IgG levels often exceeding 16 g/L. Other causes, e.g. viral hepatitis or Wilson disease must be excluded.
Treatment includes long-term immunosuppression with steroids and azathioprine. While gt;80% cases achieve remission with treatment, relapses are common after discontinuation of therapy.
Prednisolone is started as PO 1-2 mg/kg/day until serum ALT values normalize, followed by gradual tapering to a maintenance dose of 0.1-0.3 mg/kg/d till normal liver histology. In cases with poor response or side-effects, Azathioprine (PO 1.5-2.0 mg/kg/d) may be added. Mycophenolate, Tacrolimus and Rituximab are other options.
Wilson disease is a common disorder of copper metabolism (1:10000-00000 births), clinically characterised by a triad of—(a) chronic liver disease, (b) neurological signs, and (c) kayser-Fleischer (KF) ring over cornea.
Etiopathogenesis: It is an autosomal recessive disorder involving chromosome 13, with basic defect in mobilization of copper from hepatocytic lysosomes due to mutations in gene ATP7B.
In fetal life, high metallothionein (copper-binding protein in tissues) with low ceruloplasmin (copper-binding protein in plasma) activity facilitates deposition of copper in tissues. Normally, this pattern reverses to adult pattern of low-metallothionein/high-ceruloplasmin levels by 2 years of age. Failure of this switch-over in Wilson disease leads to accumulation of copper in hepatocytes and consequent destruction. Escaped copper from hepatic cells also leads to systemic copper deposition and toxicity in other tissues, e.g. brain, cornea, kidneys and joints.
Clinically, age and mode of presentation in Wilson disease usually follows a familial pattern. Most cases present between 5-10 years of age with:
• Hepatic involvement, as the earliest feature, presenting with hepatomegaly, jaundice, sub-acute hepatic failure and portal hypertension.
• Neurological manifestations usually after the first decade with intention tremors, dysarthria, dystonia, rigidity, chorea and behavioral changes. Preceding liver involvement is common but not mandatory.
• Ocular manifestation, i.e. development of a rusty-brown Kayser-Fleischer ring over cornea is usually present at the time of liver disease (Fig. 15.3).
• Systemic complications due to involvement of other tissues are seen in long survivors, as Fanconi syndrome, hemolytic anemia, chronic arthropathy and endocrinopathies.
Diagnosis: Low serum ceruloplasmin level (lt;20 mg/dl) is the best screening test for Wilson disease, supported by elevated
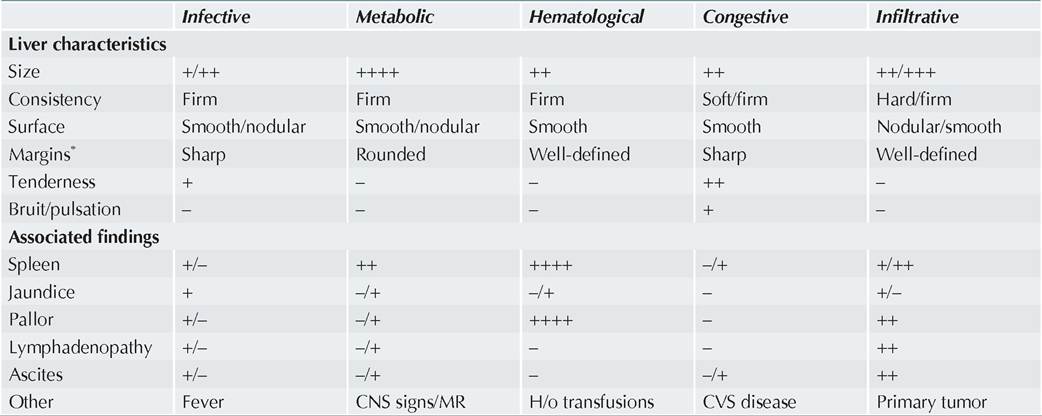
Fig. 15.3: Kayser-Fleischer ring in Wilson disease.
urinary copper levels (gt;100 #956;g#8725;day). Serum copper may be low, normal or elevated.
Diagnosis is conventionally confirmed by:
• Penicillamine challenge test, i.e. gt;5-10 fold rise in urinary copper excretion (gt;1000 #956;g#8725;day) after two doses of d-penicillamine (PO 500 mg/dose at 12-hr interval),
• Increased copper content in dry liver tissue (gt;250 #956;g#8725; gram of liver tissue).
However, combination of—(a) low serum ceruloplasmin, (b) presence of KF ring, and (c) elevated 24-hr urine copper may be used to confirm the diagnosis of Wilson's disease.
Penicillamine challenge test is not routinely recommended n due to high false-positivity and liver copper estimation is not easily available with quality issues. Uneven copper distribution in liver limits its usefulness. High liver copper may also be present in cholestatic liver disorders.
Family screening with serum ceruloplasmin and urinary copper levels is necessary.
Management revolves around the copper chelation therapy by PO Penicillamine (20 mg/kg/day q12hr) to increase urinary excretion. Uncommon but significant toxicities of penicillamine include SLE, aplastic anemia and nephrosis.
In cases with penicillamine intolerance or toxicity, alternative copper chelator Trientine (Triethylenetetra- mine-2-dihydrochloride) may be used.
Zinc may be added to decrease gut copper absorption (PO 25 mg/kg/day q8hr).
Outcome: Early chelation therapy is most important determinant for outcome, which leads to complete resolution of liver histology and disappearance of KF ring. Untreated cases die due to AHF or renal/ neurological complications. Chelation therapy is indicated even in asymptomatic siblings.
Indian childhood cirrhosis (ICC), was a unique disease limited to Indian subcontinent, extremely rare at present. Epidemiology: ICC was almost exclusively seen in children aged 6 months-3 years, more common in males, top-fed children and certain communities—North-Indian banias and south-Indian Brahmins.
Etiopathogenesis yet remains uncertain, proposed to be infective, immunological, toxic, metabolic or nutritional injury to hepatocytes. Most acceptable one is the role of increased copper deposition in liver either due to altered metabolism or increased dietary intake due to cooking/ water storage in copper/brass vessels.
Clinically ICC commonly presented as gradually progressive disease with 3 stages:
a. Pre-icteric stage (3-6 months), with abdominal distension, failure to thrive, anorexia, and altered behavior. Moderate hepatomegaly with typical firm consistency, sharp-leafy margins and finely nodular surface was pathognomonic..
b. Icteric stage with gradual increase in liver size, jaundice and portal hypertension with splenomegaly and ascites.
c. Terminal stage of liver failure with bleeding diathesis and encephalopathy.
Diagnosis rested onliver biopsy showing: (a) complete destruction of liver architecture with nodule formation,
(b) diffuse creeping fibrosis without regeneration,
(c) increased copper content on orcein staining, and
(d) presence of Mallory's hyaline bodies—clumps of eosinophilic hyaline material, in 15-20%.
Management: ICC was almost always fatal, though very few cases have recovered spontaneously. Apart from supportive measures attempts were made to treat ICC with immunomodulatory drugs, e.g. steroids, or copper chelators, e.g. d-penicillamine, with equivocal results.
Non-alcoholic fatty liver disease (NAFLD) or steato- hepatitis (NASH) is a common but benign cause of chronic liver disease, usually associated with obesity and insulin resistance.
NAFLD is a pathological diagnosis with macrovesicular steatosis, without inflammation or with inflammation, later termed as NASH.
Clinically, most children are obese and asymptomatic or present with vague abdominal pain and moderate hepatomegaly. Acanthosis nigricans (velvety brownblack pigmentation over nape of neck, axilla and skin folds) is common in 3-0% cases, often associated with hyperinsulinemia due to insulin resistance.
Diagnosis: Although radioimaging procedures can detect fatty liver, biopsy may be necessary in some
cases to exclude serious pathologies. Non-invasive measurements of fibrosis by transient elastography or acoustic radiation forced impulse may be useful to avoid biopsy. Liver enzymes may be elevated, along with hypertriglyceridemia and hyperglycemia despite hyperinsulinemia.
Management aims to reverse the liver disease by life styles changes to control obesity, e.g. dietary modifications and exercise. Most cases respond well to weight reduction and vitamin D or E supplementation. Progression to cirrhosis is very rare.
Congenital hepatic fibrosis, an autosomal recessive disorder, is an important cause of portal hypertension. These cases usually present in late childhood with hepatosplenomegaly and esophageal varices with intermittent hematemesis. Liver biopsy is diagnostic with diffuse periportal and perilobular fibrosis in broad bands, containing distorted duct-like structures or microcyst formation. Renal disease, e.g. polycystic kidney is present in ~ 3/4th cases.
Management includes control of esophageal bleeding/ varices and treatment of renal disease. Some cases may need shunting procedure.
Caroli disease, i.e. congenital saccular dilatations of intrahepatic cuboidal epithelium, may be an isolated defect or associated with congenital hepatic fibrosis and polycystic kidneys (Caroli syndrome). Both variants are autosomal recessive. Most cases present with recurrent acute cholangitis and gallstones, before development of portal hypertension.
15.8