ABDOMINAL WALL DEFECTS
While not the intestinal malformations in true sense, abdominal wall defects are important causes of the herniation of intestines or other abdominal viscera in newborn or young infants.
Some important abdominal wall defects are as follows:Umbilical hernia due to incomplete closure of the fascia of umbilical ring, presents with herniated omentum or bowel, covered with skin. Umbilical hernia of lt;1.5 cm usually close spontaneously by 4 years of age and complications, e.g. intestinal incarceration are rare.
Surgical closure is advisable if defect exceeds 1.5 cm at 2 years of age. Manual reduction with strapping over the ring does not accelerate closure of defect and is no longer advised.
Omphalocele, i.e. herniation of abdominal viscera through umbilical and supraumbilical portions of abdominal wall at birth, denotes incomplete migration of bowel from the umbilical coelom. Herniated organs are covered with a peritoneal sac, which may rupture in utero or at birth. Associated anomalies are common, e.g. gut malformations, CHDs and Beckwith-Wiedemann syndrome. Primary closure is possible for small defects, while larger defects need two-stage repair.
Gastroschisis is the herniation of the variable length of intestines or other abdominal viscera, without a covering sac, through a para-umbilical defect. Eviscerated organs may be covered by a gelatinous matrix of greenish material at birth. Most of these cases are preterm and ~20% have other congenital anomalies. Gastroschisis is a surgical emergency, though single-stage repair is rarely possible.
Inguinal hernia denotes protrusion of a part of abdominal viscera, usually the intestine through inguinal canal.
Incidence of inguinal hernia in children is estimated to be ~1-3% live births, more common in males (4-8:1) and preterms. About 99% of inguinal hernias are indirect and more common on right side (60%).
Direct inguinal hernia or femoral hernia is rare in children.Etiologically, patency of processus vaginalis is the principle defect in inguinal hernia, seen in ~80-90% at birth and ~50% at 1 year. Calcitonin-gene related polypeptide (CGRP) plays an important role in its closure. Other contributing factors for hernia include: (a) chronic cough, (b) connective tissue disorders, e.g. Ehlers-Danlos syndrome, (c) undescended testis, and (d) ascites.
Clinically these cases present with inguinal swelling that increases on crying or straining. Silk glove sign, i.e. silky feeling of processus vaginalis on rubbing over the spermatic cord may be present. Hydrocele, due to patent processus vaginalis, usually co-exists as scrotal swelling. Complications of hernia include: (a) incarceration, (b) obstruction, (c) gangrene, and (d) testicular damage.
Management is essentially surgical with open or laparoscopic herniotomy and closure of hydrocele sac. As ~10-15% cases may later develop contralateral hernia, routine exploration on other side for patent processus vaginalis is advisable in boys lt;1 year and in all girls with left-sided hernia.
14.10 ACUTE DIARRHEA
TABLE 14.13: Common causes of acute diarrhea
Diarrheal disorders are second commonest cause of morbidity and mortality in preschool children, after acute respiratory infections. Since normal frequency of stools varies significantly in children, diarrhea is defined as 'a change in the usual frequency or consistency of stools'. Presence of blood or mucus in stools denotes dysentery (Ch 10.8).
Diarrheal disorders may be classified as:
• Acute diarrhea, lasting for lt;14 days; discussed in this chapter
• Persistent diarrhea, i.e. continuation of an acute diarrheal episode for gt;14 days (Ch 14.11)
• Chronic diarrhea of gt;14 days duration, due to disorders of malabsorption (Ch 14.12).
Incidence: Usually underreported, acute diarrhea accounts for ~30% of hospital admissions and ~15% of deaths in under-5 children.
NFHS-5 (2019-21) reveals that ~7% under-five children in India had diarrhea during preceding two weeks of survey visit.Epidemiology: Acute diarrhea is most common in 6 months-3 years age-group, specially in children with following risk factors—(a) top feeding, (b) contaminated water supply, (c) low socioeconomic status, (d) poor sanitation and excreta disposal, (e) unhygienic food habits, (f) malnutrition, and (g) vitamin A deficiency.
Diarrhea and malnutrition have a cause-effect relationship. While diarrhea is common in malnourished children due to—(a) gut mucosal atrophy, and (b) colonic overgrowth of bacteria due to impaired immune defence; each diarrheal episode worsens the nutritional status due to—(a) anorexia, (b) poor absorption, (c) increased nutritional requirements and sometimes, (d) misconceived starvation of child due to fear of increasing diarrhea after feeding.
Etiology: More than 90% of infantile diarrhea are infective in origin (Table 14.13).
Rotavirus is the commonest cause of acute diarrhea in infants and toddlers, responsible for gt;50% and ~25-30% episodes, respectively. Seven serotypes are known to cause human disease, the commonest in India being G1P8, responsible for ~60% cases.
Infection is acquired feco-orally, usually in 3-24 months age-group and during winter or spring season. Over half of the cases are asymptomatic. Symptomatic infection is self-limiting within 3-5 days but persistent diarrhea due to secondary lactose intolerance is not uncommon.
Bacterial diarrhea: E. coli, with its four sub-types, i.e. enterotoxigenic (ETEC), enteropathogenic (EPEC), enteroadherent (EAEC) and enteroinvasive (EIEC), is the second commonest (25%) cause of diarrhea in Indian children. Of these, ETEC is most common, with serotype
• Infective diarrhea
- Viral:
Rotavirus (25-50%) Others: Astroviruses, enteroviruses
- Bacterial:
E. coli, (25%)
V. cholerae (5-10%)
C. jejuni (5-10%)
Shigella/Salmonella (5-10%)
- Protozoal: Giardiasis, amebiasis
- Parasitic: Intestinal helminthes
- Opportunistic: Candida, spore-forming protozoa*
• Parenteral diarrhea: Non-GIT infections, e.g.
ARI, UTI, otitis media• Non-infective diarrhea
- Drug-induced: Antibiotics, laxatives, iron
- Toxins: Food poisoning**, heavy metals
- Food allergy
- Others: Overfeeding, psychogenic diarrhea
*Cryptosporidium, isospora bacilli, cyclospora, microsporidia **Due to pre-formed toxins, e.g. Staph. aureus, C. difficile
E-0159 emerging as an important cause of cholera-like outbreaks. EPEC is more common in urban children or as Traveller's diarrhea, while EAEC or EIEC usually present as bacillary dysentery.
Other bacterial pathogens, e.g. V.cholerae, Shigella and Salmonella infections accounts for 10-15% cases. Camplyobactor jejuni-a zoonotic infection, transmitted by excreta-contaminated food/water, is an emerging cause of acute infantile diarrhea.
Protozoal diarrhea: Amoebiasis is relatively less common in children than Giardiasis—a leading cause of diarrhea in malnourished children. Spore-forming protozoa, e.g. cryptosporidium, isospora, cyclospora and microsporidia are predominant causes of recurrent diarrhea in immunocompromised children, though small outbreaks of mild diarrhea are common even in normal children.
Parenteral diarrhea denotes increased gut motility in extraintestinal infections, e.g. otitis media, ARI or UTI, which usually disappears spontaneously or after treatment of primary infections.
Food poisoning is an important cause of acute diarrhea, when multiple children and/or adults are affected simultaneously after common food ingestion.
Pathogenesis-wise, diarrhea may be broadly divided into following categories:
• Secretory diarrhea by exotoxin-producing pathogens, e.g. cholera or ETEC, due to stimulated production of adenylyl cyclases and cyclic AMP/GMP leading to increased ATP activity and active secretion of sodium and water in gut lumen.
• Osmotic diarrhea, i.e. passive outflow of water, due to increased osmotic load in gut, e.g. in lactose intolerance.
• Invasive diarrhea (dysentery) due to actual mucosal invasion, e.g.
EIEC, EAEC and Shigella infections or adhesion of pathogens to mucosal cell walls without destruction, e.g. EPEC.• Hypermotility diarrhea, due to parenteral infections or non-infective causes, e.g. drugs, overfeeding, psychogenic causes, etc.
Pathophysiology: Dehydration and electrolyte disturbances are most important complications of diarrhea, due to excess loss of water and electrolytes (mainly sodium) in stools. While initial losses are mainly from extracellular fluid compartment (ECF), consequent changes in plasma osmolality lead to redistribution of body fluids, as follows:
• When water and sodium loss is nearly proportional as in osmotic diarrhea, serum osmolality is maintained, leading to isotonic dehydration (50% of total diarrhea).
• When sodium loss is disproportionately more than the water loss as in secretory diarrhea, serum osmolality falls leading to hypotonic dehydration (30-40%). In these cases, extracellular hypotonicity moves water from ECF to ICF, accentuating ECF dehydration and hypovolemia. Consequently, signs of dehydration are relatively more marked than the actual fluid loss in hypotonic dehydration.
• Rarely, and specially when dehydration is erroneously treated with concentrated ORS or hypertonic parenteral fluids, serum osmolality rises to cause hypertonic dehydration (5%). In these cases, extracellular hypertonicity withdraws water from ICF to ECF, leading to cellular dehydration. Signs of dehydration are relatively less prominent than actual fluid deficit in hypertonic dehydration.
Severe ECF depletion and hypovolemia leads to compensatory responses, e.g. peripheral vasoconstriction (cold skin, dry mucosa), hyperdynamic circulation (weak- thready pulse), oliguria, and finally, the hypotension/ shock. As considerable amount of potassium and bicarbonates (intestinal pH is alkaline) is also lost in stools, hypokalemia and acidosis is common in diarrhea- induced dehydration.
Diagnostic assessment of a child with diarrhea may be divided into: (a) clinical assessment of the severity of dehydration, (b) clinical assessment of the etiology, and (c) relevant laboratory investigations.
• Assessment of dehydration: Important indicators of the severity of dehydration (as mild, moderate) or severe are given in Table 14.14. However this assessment may be unreliable in:
- Malnourished children, due to overestimation of turgor loss in wasted marasmus and underestimation in edematous kwashiorkor.
- Chubby children, due to underestimation of turgor loss. Urine output is the most reliable indicator of dehydration in malnourished or obese children.
TABLE 14.14: Assessment of severity of dehydration
| Feature | #8739;#8739;M#8725;#8725;d | Moderate | Severe |
| Behavior | #8739;#8739;Alert | Drowsy* | Stupor/coma |
| Thirst | Thirsty | Marked | Absent |
| Eyeballs | Normal | Sunken | Sunken |
| Tears | Present | Absent | Absent |
| Tongue | l#8739;Dry | Dry | Parchmenty |
| Skin turgor | Normal | Lost* | Lost |
| Pulse | Normal | Rapid | Thready |
| Respiration | Normal | Rapid | Acidotic |
| BP | Normal | Normal | Hypotension |
| Urine output | Normal | Oliguria | Anuria |
| Weight loss** | #8739;#8739;3-5% | 6-10% | 9-15% |
*Irritability and doughy skin in hypernatremic dehydration. **Higher % of wt loss in infants.
- Hypernatremic dehydration, due to relative pre- servance of ECF that leads to underestimation of dehydration. Presence of hyperirritability and doughy skin are strong indicators in these cases.
- Hyponatremic children are at risk of developing early circulatory failure and shock despite lesser fluid and weight loss due to water movement from ECF to ICF.
According to IMNCI guidelines, dehydration in children with diarrhea is classified as (a) severe dehydration, (b) some dehydration, and (c) no dehydration, based on four indicators—(1) general condition; (2) eye balls, (3) ability to drink water and (4) skin turgor (Table 29.2).
“Severe dehydrationquot; is indicated by presence of any two of the following four signs: (a) lethargy/ unconsciousness, (b) sunken eyes, (c) inability to drink, and (d) very low skin turgor; While “Some dehydrationquot; is indicated by any two of following four signs: (a) restlessness and irritability, (b) sunken eyes, and (c) thirsty, drinks eagerly, and (d) low skin turgor. Absence of enough signs suggests “no dehydrationquot;.
• Clinical assessment of etiology: Viral, bacterial and protozoal diarrhea may be distinguished up to certain extent on the basis of age, nutritional and immune status, seasonal trends, clinical features and appearance of stools (Table 14.15). Some important indicators are as follows:
- Large-watery diarrhea in apparently healthy infant or toddler suggests rotavirus infection. Perianal excoriation is common.
- Rice-water stools indicate cholera and enterotoxigenic E.coli infection.
- Presence of blood / mucus in stools with high fever, toxic look and cramps suggest bacterial etiology.
- Watery, foul-smelling stools with/without blood, in school-going children may be amebic in origin.
- Watery or bulky diarrhea with fat globules, specially in malnourished children suggest giardiasis.
• Laboratory evaluation in diarrhea includes:
| TABLE 14.15: D/D viral, bacterial and protozoal diarrhea | |||
| Viral | Bacteria | Protozoal | |
| Epidemiology | |||
| Common Age | Infants | Pre-school | bgcolor=white>School-age|
| Nutrition | Normal | PEM | N/PEM |
| Immune status | Normal | n/4 | n/4 |
| Season | Winter | Monsoons | Monsoons |
| Clinical | |||
| Onset | Acute | Sub-acute | Sub-acute |
| Fever | +/- | ++ | - |
| Toxemia | - | ++ | - |
| Vomiting | ++ | +/- | - |
| Dehydration | ++ | +++ | + |
| P'anal redness | +++ | + | +/- |
| Stool findings | |||
| Volume | Large | Large | Variable |
| Consistency | Frothy | Curdy | Bulky |
| Odor | Odorless | +/- | ++ |
| Blood/mucus | Absent | + | +/- |
| Fat globules | -/+ | -/+ | ++ |
| Microscopy | |||
| Pus cells | -/+ | gt;10/hpf | +/- |
| Cysts | - | - | + |
| Common cause | Rotavirus | ETEC | Giardia |
ETEC: Enterotoxigenic E.coli, EH: Entamoeba histolytica
- Stool examination, specially for pH, reducing sugar, fecal leukocyte count, fat globules, parasitic cysts/ova. Hanging-drop preparation is essential in rice-water stools to exclude cholera.
- Stool cultures are of limited value due to poor specificity, but indicated in—(a) suspected cholera, (b) critically sick children to exclude nosocomial infection, and (c) immunocompromised states to exclude opportunistic pathogens.
- Specific investigations: Virological diagnosis of rotavirus by electron microscopy or ELISA test is possible, but rarely available. ELISA tests to detect ETEC or vibrio toxins are also available.
- Supportive investigations including serum electrolytes, blood gas analysis and renal functions, e.g., blood urea or serum creatinine, are necessary in severe dehydration.
Management of acute diarrhea includes—(I) fluid replacement therapy, (II) nutritional management, (III) specific antidiarrheal agents, and (IV) treatment of associated infections and other complications
I. Fluid replacement therapy is the cornerstone of management in acute diarrhea, to prevent and correct dehydration. The mode of fluid replacement (oral vs. parenteral) depends on severity of dehydration and child's willingness or tolerance (vomiting) for oral fluids.
WHO guidelines (2005) regarding fluid therapy in childhood diarrhea (Fig. 14.15), are based on three options:
• Plan A to prevent dehydration in children with “No dehydrationquot; providing oral rehydration solution (ORS) at home as follows—50-100 ml after each stool in children lt; 2 years, 100-200 ml after each stool in 2-10 years old and ad libitum in older children.
• Plan B, i.e. supervised ORS administration in the hospital for children with some dehydration. The amount of the ORS to be given during first 4 hours depends on the age of the child, as stated in Fig. 14.15.
• Plan C, i.e. parenteral rehydration in cases with severe dehydration (see Parenteral fuild therapy below).
Frequent re-evaluation and necessary modifications in fluid therapy is essential in all cases. Some important aspects of oral and parenteral fluid therapy are discussed here:
Oral rehydration therapy is the preferred mode of fluid replacement in diarrhea for—(a) prevention of dehydration, and (b) correction of mild to moderate dehydration. It may be safely used in all cases of diarrhea except those with—(a) paralytic ileus (when oral feeding needs to be withheld), and (b) altered sensorium (risk of aspiration). Children with vomiting may be given oral fluids after anti-emetic therapy.
Oral rehydration solution (ORS) is one of the most important medical advance in last century, which has reduced the diarrhea-related mortality by gt;80%.
Principle of ORS therapy in diarrhea is based on following facts:
• Large amount of fluids are lost in diarrhea, which needs to be replenished with fluids.
• Substantial amount of sodium and other electrolytes are also lost in diarrhea. As sodium is the principle determinant of ECF osmolality, its presence is a must in any ORS.
• Water absorption in gut is largely passive, dependent on active sodium absorption.
• Absorption of glucose and amino acids are carrierdependent and remain largely intact in most cases of diarrhea.
• Carrier mechanisms for sodium absorption are interlinked with glucose/ amino acid absorption and co-administration of glucose or amino acids in ORS facilitates sodium/water absorption.
• Since excess intake of glucose may cause osmotic diarrhea, 1:1 molar ratio of glucose and sodium concentration in ORS is most appropriate to maximize sodium reabsorption with minimal osmotic load.
• As potassium and bicarbonates losses are also common in GIT fluid loss, ORS should also contain minimum required concentration of these electrolytes.
WHO-ORS contains 75 mEq/L of sodium with osmolality of 245 mEq/L, in composition as given in Table 14.16. It

Fig. 14.15: WHO/National task force guidelines for management of diarrhea in children. *Teach mother about danger signs or dehydration and ask to report immediately
**Give 1 packet of ORS in plan A and 2 packets in plan B for home use, before sending home Source: WHO (2005): The treatment of diarrhea: A manual for physicians and other senior health workers.
is supplied free of charge by the government at health centers and is also available commercially.
Preparation and storage: WHO-ORS must be prepared hygienically, mixing one packet of ORS in one liter (~5 glass) of potable, clean water. Once prepared, it should be stored in a clean container and may be used till 24 hours. Pre-packed ORS has a shelf-life of 2 years. Smaller packs of ORS, to be dissolved in 200 ml are also available commercially, as also ready-to-use solutions.
Dosage and administration: It may be fed with spoon or a large cup ad libitum (as much as desired) for prevention of diarrhea, with minimum quantities as stated in Figure 14.15 for Plan A and B in children with dehydration.
TABLE 14.16: Composition of WHO-ORS
| Constituents | Weight (gm/dl) | Electrolytes | (mmol/L) |
| Sodium chloride | 2.6 | Na+ | 75 |
| Potassium chloride | 1.5 | K+ | 20 |
| Tri-sodium citrate | 2.9 | Citrate | 10 |
| Glucose | 13.5 | Cl- | 65 |
| Water | 1000 | Glucose | 75 |
| Osmolality | 245 |
Side-effects: WHO-ORS is extremely safe, except potential risk of hypernatremia due to use of wrongly concentrated ORS. In addition, mothers may erroneously perceive ORS as replacement for regular feeding, which should be continued in all cases.
Modified ORS: Various other ORS preparations with different composition have been developed to maximize sodium/water absorption or reduce the risk of hypernatremia/osmotic diarrhea in special situations. Some are as follows:
• Resomal (Rehydration solution for Malnourished children) with 45 mEq/L of sodium, is preferred in malnourished children due to higher risk of hypernatremia. Not commercially available in India, it may be prepared by diluting one pack of WHO-ORS in 2 liters of water and adding 50 gm of sucrose as well as 40 ml of mineral-mix solution (Ch 6.1).
• Enriched or super ORS is prepared by—(i) addition of certain amino acids, e.g. glycine, L-alanine or glutamine in standard ORS; or (ii) replacement of glucose with a starch preparation, e.g. pre-cooked or puffed rice powder (~ 50 gm/L). While amino acids enhance the sodium co-transport and reabsorption (independent of glucose-based transport), starchbased preparations reduce the risk of osmotic diarrhea
by slower release of glucose. While these variants might be marginally superior in cholera, no significant benefits over WHO-ORS have been observed in noncholeric diarrhea and tend to affect the palatability or cost of preparation.
• ORS in very young infants: Although WHO-ORS may be safely used in all children, a diluted preparation (1 pack in 1.5 liter of water) may be used in very young infants lt;2 months, to avoid osmotic load. However, breastfeeding is usually adequate in these cases and ORS is rarely required.
Home-based ORS substitutes: Following fluids may be used as temporary alternatives of ORS, in order of preference:
• Salt and sugar solution (SSS) by mixing a two-finger pinch common salt (~0.8 gm) and one heaped tsf of sugar (~8 gm) in one glass of water (~200 ml). However, sodium/sugar content in SSS is unreliable and it should be avoided as far as possible, unless WHO-ORS is not readily available.
• Food-based home fluids, e.g. salted-rice kanji, dalwater, butter-milk, lemon sherbat or coconut water may be used as adjuvant or temporary alternative for ORS. However, these fluids have no definite electrolyte concentrations and start fermenting after 6-8 hours in tropical climate.
Plain glucose water may cause osmotic diarrhea and should never be used as ORS, as also the sweet tea, coffee, canned fruit juices and carbonated drinks.
Parenteral fluid therapy is required in cases with—(a) severe dehydration, (b) persistent vomiting/abdominal distension, and (c) altered sensorium; and aims to correct fluid/electrolyte deficit till minimum safe limit, when ORS may be continued for further correction and maintenance. Some important aspects of parenteral fluid therapy in diarrrhea are as follows:
• Route: Although a secure IV access is must for parenteral fluid administration, intra-osseous infusion (Ch 32.3) may be used for rapid fluid correction in emergency, till IV access is obtained. Nasogastric infusion (20 ml/kg/hr) is also useful in this situation.
• Composition: Ringer lactate (Na+ 131 mEq/L) is preferred choice for parenteral fluid therapy in diarrhea, though normal saline (Na+ 154 mEq/L) may also be used as an alternative. Plain dextrose fluids are ineffective and may aggravate hyponatremia. Potassium (2 mEq/ kg; upto maximum 40 mEq/L) must be added in IV infusion, but only after baby has passed urine, to avoid hyperkalemia.
• Amount of fluid infusion depends on the severity of dehydration. WHO-Plan C provides necessary guidelines for routine IV fluid volumes (Table 14.17).
• Monitoring: All cases on IV fluids should be closely monitored to decide changing needs for fluids/ elec

trolytes, possibility of switch-over to ORS and complications, e.g. overhydration, electrolyte disturbances, infection, thrombophlebitis or local extravasation.
II. Specific anti-diarrheal therapy includes: (a) antimicrobial agents, (b) zinc supplements, (c) prebiotics or probiotics, and (d) antisecretory agents, e.g. racecadotril. Others antidiarrheal agents like adsorbents/binding agents (kaolin, pectin) are no longer used and antimotility agents (loparamide, diphenoxylate) are contraindicated in children due to risk of paralytic ileus.
• Antimicrobial therapy: Since most cases of acute diarrhea are viral and self-limiting, empirical antimicrobial therapy is of limited use and may lead to development of chronic carrier state or antibiotic- associated diarrhea. However, antimicrobials are indicated in: (a) suspected cholera or bacillary dysentery, (b) co-existing septicemia or systemic infections, and (c) toxic, malnourished or immunodeficient children.
Some commonly used antimicrobial agents in diarrhea, based on the standard treatment guidelines of IAP (2022) are given in Table 14.18.
• Zinc supplementation has been shown to promote mucosal healing and reduce the severity and duration of diarrhea. WHO/IAP/GOI strongly recommend elemental zinc supplements to all children with diarrhea as PO 20 mg/ day (10 mg/ day in infants lt;6 months of age) for 14 days.
• Probiotics and prebiotics have a potential role in treatment of childhood diarrhea, specially antibiotic-

mkd: mg/kg/day, ETEC: Enterotoxigenic E. coli
*Non-typhi, Only in high-risk children ** above 2 years of age
Source: Standard treatment guidelines for acute watery diarrhea, IAP 2022.
associated diarrhea. These agents inhibit the growth of pathogenic flora and promote re-colonization with normal non-pathogenic flora.
Probiotics are viable bacteria, e.g. lactobacilli or yeasts, e.g. saccharomyces, present in fermented dairy products, e.g. curd, yogurt, lassi, etc. or available commercially. These agents: (i) competitively inhibit the binding sites for pathogenic bacteria, (ii) acidify gut to inhibits pathogenic growth, (iii) restore non-pathogenic flora, (iv) stimulate secretory IgA production, and (v) modify toxin receptors in gut. Efficacy of probiotics depends on the dose and the strain/s used for therapy, which is not yet standardized.
Prebiotics are food ingredients, e.g. banana, sorghum, lactulose, bran, isabgol, etc., which largely remain undegraded in gut and: (a) stimulate growth of normal gut flora, (b) prevent growth of pathogenic organisms by acidification of gut, and (c) maintain epithelial integrity.
• Anti-secretory agents: Racecadotril (PO 1.5 mg/kg/ dose q8hr)-an oral encephalinase inhibitor, may be useful to reduce the stool volume in secretory diarrhea, though there is no uniform consensus regarding its use in children. It prevents inactivation of endogenous encephalins-cyclic AMP inhibitors in gut, thus reducing active fluid/electrolyte secretion from gut.
III. Nutritional management: Diarrhea is major precipitating factor for malnutrition in children. Hence, it is recommended that:
• Breastfeeding should be continued uninterrupted.
• Contrary to general perception, no dilution of animal/ formula milk is necessary in top-fed children during diarrheal episodes.
• Children on regular diet should be fed with small frequent meals of energy-dense foods.
• Post-recovery, oral intake should be enhanced to 125% of normal caloric requirements.
National Control Of Diarrheal Diseases
Programme (NCDDP)
NCDDP, started as a disease-specific program in 1978 is currently a component of Reproductive, Maternal, Newborn, Child and Adolescent Health strategy (RMNCH+A), delivered as per Integrated Management of Neonatal and Child Illnesses (IMNCI) guidelines.
Components: Important activities under this program include:
• Standard cases management guidelines for general use (Fig. 14.15).
• Promotion of preventive measures, e.g. breastfeeding, hygiene and ORS therapy.
• Free supply of WHO-ORS, with a printed logo for easy identification (Fig. 14.16).
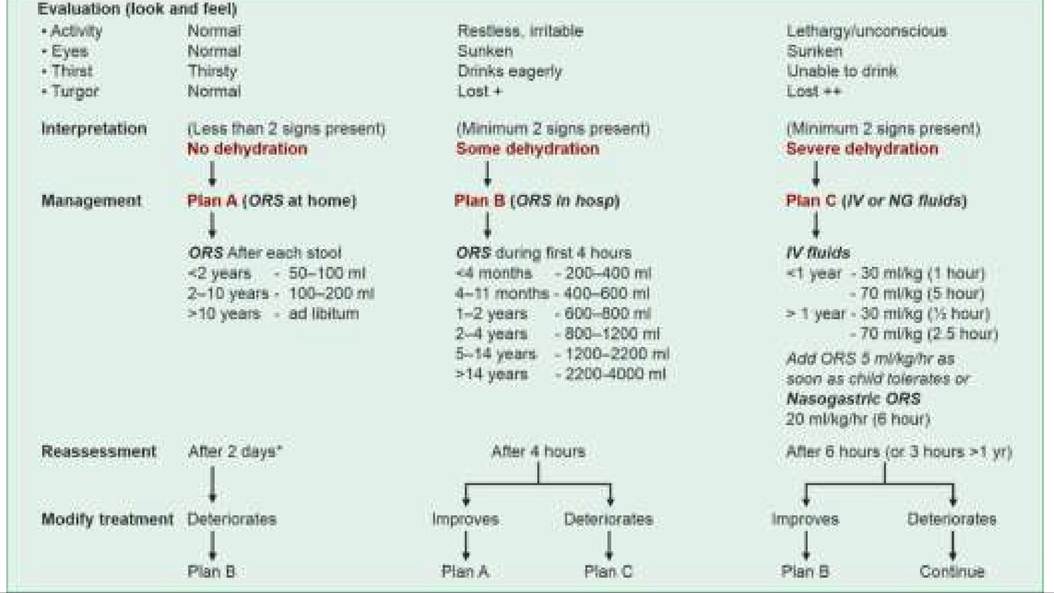
Fig. 14.16: ORS logo.
• Setting-up of diarrhea training and treatment units (DTTUs)
• Research, surveillance and manpower training
Diarrhea training and treatment units (DTTUs) have been established under this program at medical colleges and major hospitals to: (a) streamline practice of standard cases management guidelines on regular basis, (b) train faculty members, medical students and other health personnel, and (c) educate mother about home management of diarrhea, including demonstration of ORS making and administration.
Mini-DTUs and ORT corners have been established at smaller primary health centers to implement standard cases management guidelines and maternal education.
Despite these targeted efforts, NFHS-5 (2019-21) revealed that ORS and Zinc supplements were received by only 60% and 30% of under-five children respectively, who had diarrhea in preceding two weeks of survey.
14.11