ACUTE BRONCHIOLITIS
Acute bronchiolitis is a common viral illness in infancy, characterized by acute, self-limiting inflammation and obstruction of smaller airways.
Etiology: Respiratory syncytial virus (RSV) is the commonest cause of bronchiolitis in gt;50% cases.
Other causes include parainfluenza type 3, mycoplasma, and adenoviruses.Epidemiology: Acute bronchiolitis is almost exclusively seen during first two years of life, most commonly from 3-6 months of age. Maximum cases occur in winter or early spring season. Male sex, top-feeding, overcrowding and passive smoking are other high-risk factors.
Etiopathogenesis: Infection is usually acquired from a family adult or older child, suffering from minor viral illness. Viral invasion leads to mucosal edema and collection of mucus and cellular debris in smaller bronchioles with consequent airway obstruction. As airway diameter is comparatively smaller during expiration, obstruction is predominantly expiratory and leads to distal air trapping with patchy emphysematous and atelectatic areas (after absorption of trapped air). Diminished ventilation produces hypoxemia, hypercarbia and respiratory acidosis.
Clinically, these cases present with:
• Preceding history of mild viral illness for 2-3 days, followed by:
• Acute onset of moderate fever with wheezy cough and feeding difficulties, and
• Rapidly progressive respiratory distress with overinflated chest (due to air trapping), diminished air entry and few rhonchi and fine crepitations. Auscultatory finding in bronchiolitis are disproportionately less than the severity of distress.
• Self-limiting course with gradual recovery in 2-3 days. Less than 1% cases progress to respiratory failure.
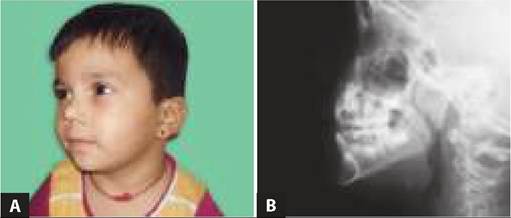
Diagnosis depends on: (a) clinical grounds, i.e. age and paucity of lung signs despite severe dyspnea, and (b) chest X-ray showing diffuse hyperinflation of lungs with pushed down diaphragm and patchy areas of atelectasis or consolidation (Fig.
16.8).Although rarely possible, virus may be demonstrated in nasopharyngeal secretions by ELISA, PCR or culture. D/D: Bacterial pneumonia and asthma are two important D/Ds for acute bronchiolitis.
Presence of high fever, significant auscultatory and radiological findings and polymorphonuclear leukocytosis indicates bacterial pneumonia.

Fig. 16.8: Acute bronchiolitis: Bilateral hyperinflated lung Aelds on X-ray chest.
*to Nebulized salbutamol
Initial attacks of asthma and bronchiolitis are almost indistinguishable though following features suggest possibility of asthma: (a) family history of atopy, (b) recurrent attacks, (c) eosinophilia, (d) absence of fever and (e) response to nebulized salbutamol (Table 16.17).
In general, first episode of wheeze following an upper respiratory tract infection in children less than 2 years of age is presumed to be bronchiolitis.
Management: Hospitalization is indicated in cases with (a) respiratory rate gt;60/minute, (b) severe chest indrawing, (c) presence of danger signs (inability to feed, vomiting, seizures or altered sensorium), (d) SpO2 lt;92% or (e) those staying away from hospitals. Treatment is largely supportive with:
• Humidified oxygen with regular oxygen saturation (SpO2) monitoring. Severe cases may require CPAP, assisted ventilation or even extracorporeal membrane oxygenation.
• Nursing in semi-sitting position with head and chest elevated at 30° and neck extended.
• Fluid and electrolyte correction, with additional fluids for insensible water loss.
• Nebulizations with hypertonic saline, salbutamol or adrenaline are of no consistent benefit but may be continued every 4-6 hours in cases, who respond to the first dose.
• Antibiotics, no value for viral disease, are commonly used to prevent superadded bacterial infection.
• Steroids, antihistamines, nasal decongestants, chest physiotherapy, steam inhalation etc. should be strictly avoided. Nose block may be cleared with saline nasal drops and gentle suctioning. Sedatives are contraindicated and may mask signs of respiratory failure.
• Ribavarin-a specific antiviral agent (given as aerosol), though not useful routinely, may be used in cases with pre-existing lung or heart disease or immunodeficiency.
Prevention: RSV-specific immunoglobulin or monoclonal antibodies (Palivizumab) may be given prior to RSV season in high-risk cases, e.g. those with chronic lung disease. However, hand hygiene is the best measure to prevent transmission of viruses responsible for bronchiolitis.
Acute bronchitis usually follows a viral upper respiratory tract infection, leading to protracted cough due to inflammation and hypersensitization of airways. Initial dry, hacking cough of acute illness may become productive after several days with purulent sputum. Chest pain and vomiting during or after a bout of cough are common. Mucus gradually thins and cough abates over next 2-3 weeks.
Chest examination and radiographs are usually normal, unlike in pneumonia. Treatment is nonspecific with no role of antibiotics. Cough syrups and antihistamines may provide temporary relief but dry-up the secretions and can mask serious disease, hence, not recommended.
Chronic bronchitis with productive cough of gt;3 months each year for gt;2 years, is not as well-defined entity in children as in adults. Rather than the environmental factors, it may be an indicator of serious underlying illness and must be investigated.
Bronchiolitis obliterans: Bronchiolitis obliterans is a chronic lung disease with progressive airway obstruction by nodular masses of granulation and fibrosis, presumably due to exaggerated reparative response after viral infections or exposure to drugs, e.g. penicillamine or chemical inhalants, etc.
These cases present with gradually progressive dyspnea, cough with expectoration and wheezing. Chest skiagram may reveal miliary mottling or unilateral hyperlucency (Swyer-James syndrome). Lung biopsy is diagnostic. There is no specific treatment, though prolonged steroid therapy may retard the progression of disease.
16.8