BRONCHIAL ASTHMA
Bronchial asthma, the commonest chronic respiratory disease in childhood, is characterized by recurrent paroxysmal wheeze, dyspnea and cough; due to reversible and dynamic narrowing of airways associated with bronchial hyperreactivity.
Global initiative against asthma (GINA) guidelines 2023 define asthma as quot;a heterogeneous disease, usually characterized by chronic airway inflammation with history of respiratory symptoms, e.g. wheeze, cough, breathlessness and chest tightness, which vary over time and intensity, together with variable expiratory airflow limitation.quot;
Incidence of asthma in Indian school children is estimated to be ~10-15% and seems to be rising. In addition, a larger population demonstrates bronchial hyperreactivity on exercise (exercise-induced asthma) or at potential risk for asthma due to family history of atopy. Etiopathogenesis of asthma is complex, involving three major components: (a) hyperreactivity of airways, (b) allergen-induced sensitization, and (c) triggering factors.
a. Hyperreactivity of airways may be genetically determined (inherent) or acquired after non-specific inflammation of these airways due to preceding viral infections.
Maintenance of airway diameter is a function of balance between bonchodilatory adrenergic and Bronchoconstrictory cholineregic activity. Airway hyperreactivity indicates either—(a) impaired #946;-adrenergic activity due to abnormal adenylate cyclase function, and/or (b) increased cholenergic activity due to lower threshold of cholinergic receptors.
Role of inherent hyperreactivity is supported by following facts: (a) family history of atopy is present in ~50% cases, (b) a child with one affected parent has ~25% risk of developing asthma, while it rises to ~50%, if both parents are affected, and (c) bronchial lability on exercise-testing has been demonstrated in otherwise healthy relatives of asthmatic children.
b. Atopy, i.e. IgE mediated hypersensitivity to external allergens is perhaps the most important cause of airway obstruction during acute asthmatic exacerbations. Common allergens include:
• Inhalant allergens, e.g. pollens, dust and mites, danders (suspended allergens from household pets or insects), fungi, etc., and
• Ingested allergens, e.g. food allergy, though frequently implicated in asthma, true relationship between in vitro reactivity to food items on skin testing and actual in vivo precipitation of bronchospasm is rarely strong.
To recapitulate, important events in IgE mediated hypersensitivity reactions (Ch 8.4.1) include:
• Sensitization to an allergen during initial exposure, with formation of specific IgE antibodies, which attach themselves to the surface of mast cells and basophils;
• Re-exposure to the same allergen, leading to antigenantibody interaction on the surface of sensitized mast cells gt; degranulation gt; release of chemical mediators. Consequently, two types of reactions are seen
- Early phase reactions (within 20 minutes) due to release of pre-formed mediators, e.g. histamine and eosinophil-chemotactic factors (ECF), etc., presenting with acute bronchospasm and preventable by mast-cell stabilizing agents, e.g. cromolyn sodium.
- Late-phase reactions (after 4-12 hours), due to influx of inflammatory cells at the site of exposure and release of other chemical mediators, e.g. leukotrienes and prostaglandins. These mediators amplify allergic inflammation (reappearance of symptoms), facilitate further IgE production (accentuated hyperreactivity on repeated attacks) and produce more persistent airway obstruction (chronic disease). Late-phase reactions do not respond well to bronchodilators, but may be reduced by steroids.
• Trigger factors: Many non-immunological trigger agents are known to precipitate or aggravate the attacks in asthmatic children with or without atopy. A preceding mild viral infection is the commonest trigger for asthma in children, while others include- air pollutants, (e.g.
smoke), exercise, weather changes, emotional disturbances, drugs, (e.g. aspirin) and endocrinal disturbances (as seen during premenstrual period). These factors probably act by inducing nonspecific inflammatory reaction on exposure.Exercise is known to trigger asthma in susceptible children due to loss of water and heat from airways, leading to mucosal hyperosmolarity and release of inflammatory mediators from mast cells. Similar reason is proposed for asthma triggered by weather changes, i.e. dryness of airways along with changes in airborne allergens.
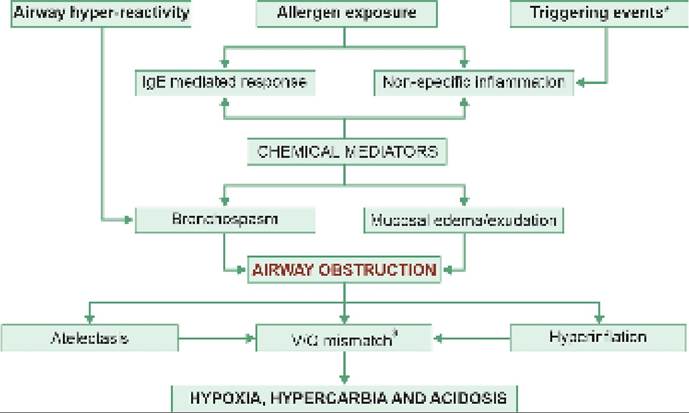
Pathophysiology: Bronchial asthma is present considered as primarily a chronic inflammatory disease, predominantly involving medium and smaller airways with:
• Persistent partial airway obstruction due to mucosal inflammation and increased mucus production, leading to air trapping in distal air passages;
• Paroxysmal, dynamic and reversible obstruction due to bronchospasm, temporarily aggravating pre-existing airway obstruction
• Airway obstruction due to above reasons, leading to air trapping in distal air passages. Obstruction is more severe during expiration due to rise in intrathoracic pressure and may lead to distal hyperinflation/ emphysema (partial obstruction/ball-valve mechanism) or atelectasis (complete obstruction).
• Mismatched ventilation-perfusion in different parts of lung with alveolar hypoventilation, leading to progressive hypoxia, hypercapnia and acidosis; culminating to respiratory failure in severe/ untreated attacks (Fig. 16.9).
Clinical manifestations of asthma are interspersed with paroxysmal exacerbations and depend on the severity of bronchoconstriction during attacks as well as in interattack period. Important attributes of these attacks are: • Age of onset: Nearly 80% of asthmatics manifest by 5 years. Asthma is more severe in younger children, due to smaller airways size. However, only minority of them continue to have persistent asthma in late childhood.
Seasonal variation: Acute attacks are more frequent in spring or rainy season, though many children have perennial disease.
Diurnal variations: Most acute attacks begin during night or early morning, when the normal airway diameter is lowest in 24 hours.
Fig. 16.9: Pathophysiology of asthma.
‘Triggering events, e.g. viral infection, exercise, emotional disturbances, air pollutants. sVentilation: perfusion mismatch, leading to alveolar hypoventilation.
• Preceding events: Although triggered by many factors, a mild viral respiratory infection is the commonest preceding event for acute attacks.
Acute asthmatic exacerbation may be paroxysmal or gradual in onset and presents with—(a) non-productive cough, (b) wheezing, and (c) dyspnea. Other symptoms, e.g. abdominal pain or vomiting due to strenuous diaphragmatic contractions, or altered sensorium due to cerebral hypoxia is common in severe attacks.
Examination reveals—(a) hyperinflation of chest, (b) diminished air entry, and (c) presence of rhonchi all over the lungs. Severe cases may also develop, (d) cyanosis, and (e) pulsus paradoxus.
Status asthmaticus denotes an acute exacerbation, refractory to usual therapy and with potential risk for respiratory failure. Development of drowsiness or confusion, bradycardia, and disappearance of wheeze and pulsus paradoxus despite progressive dyspnea, indicates imminent respiratory failure.
In between the attacks, child may be asymptomatic or has evidence of chronic airway obstruction, e.g. (a) barrel shaped chest, (b) persistent irritating cough, (c) poor exercise tolerance, and (d) growth failure.
Clinical asthma variants: Many children with hyperreactive airways present with more non-specific manifestations, termed as asthma variants, rather than classic paroxysmal attacks. Common asthma variants include-chronic noctural cough, infection-associated wheeze, exercise intolerance (exercise-induced asthma), postural asthma (related to gastroesophageal reflux), Obesity- associated asthma, etc.
Diagnosis of asthma depends on:
• Clinical presentation:
- Combination of wheeze, dyspnea and cough,
- Recurrent and paroxysmal nature of attacks,
- History of triggers, e.g. preceding viral infection,
- Family history of atopic disorders in most cases.
• Pulmonary function tests suggestive of:
- Obstructive airway disease (low FEV1 or PEFR, usually lt;80%),
- Reversibility, i.e. gt;12% rise in FEV1 or PEFR after salbutamol nebulisation,
- Diurnal variability, i.e. average gt;13% difference in morning vs evening PEFR over two weeks,
• Laboratory evaluation to identify:
- Allergic etiology-eosinophilia and IgE levels,
- Specific allergens by*:
#9632; In vivo skin or bronchial challenge tests,
#9632; In vitro RAST test for specific IgE antibodies,
- Co-pathologies: Chest X-ray, mantoux test, etc.
- Severity of the attack by blood gas analysis.
*See Ch 8.4.1 for details. Bronchial challenge tests are risky and rarely used in practice.
Peak expiratory flow rate (PEFR), defined as the measure of greatest flow rate on forced expiration after complete inspiration, is a simple and reliable indicator of the degree of airway obstruction in asthma. It may be easily measured in cooperative school-age children by Mini-Wright peak flow meter, recording the best of three efforts (Ch 32.5).
PEFR is widely used in clinical practice to:
• Monitor the course of disease using personal-best PEFR, i.e. highest PEFR record in absence of acute attack, as an individual benchmark. Personal best PEFR changes with therapy and should be revised frequently.
• Assess the severity of acute attack, by percentage change from personal-best PEFR, as mild (PEFR gt;80%), moderate (50-80%) and severe (lt;50%).
• Evaluate the therapeutic response during acute attack.
• PEFR should not be used to confirm the diagnosis of asthma, though-(a) PEFR lt; 80% for height during attack, and (b) gt;15-20% rise over basal values after salbutamol nebulisation, suggest a strong possibility.
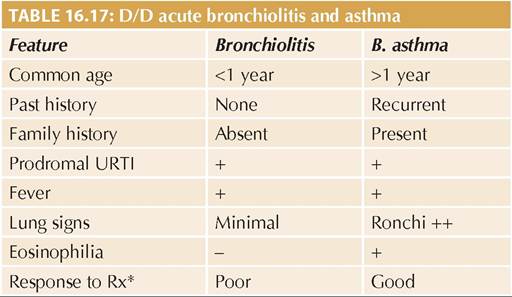
D/D of asthma includes other causes of recurrent wheeze (Ch 16.4.4) specially—(a) acute bronchiolitis (Table 16.17),
(b) infection-associated wheeze in pneumonia (d/d X-ray chest), and (c) tropical pulmonary eosinophilia (d/d AEC gt;2000, response to Diethylcarbamazine).
Conventionally, childhood wheezers have been classified on the basis of: (a) triggers, i.e. episodic whizzers or multi-triggered wheezers, or (b) time-trends of onset and course of symptoms, as follows:
• Early-onset transient wheezers, who begin wheezing in infancy, often triggered by viral respiratory infections and usually overgrow wheeze by 3 years of age.
• Late-onset intermittent wheezers, who present from 1-3 years of age and may continue wheezing till 5-6 years, before improvement.
• Late-onset persistent wheezers, who start wheezing after 3 years and generally continue to suffer till adolescence. Family history of atopy is common in them.
Late-onset persistent wheezers usually represent typical phenotype of asthma, while early-onset transient wheezing is usually due to non-asthmatic causes. However, clinical usefulness of such phenotype classifications is uncertain in predicting the risk of asthma.
Management of asthma aims to (a) control the acute attacks and their complications, and (b) improve quality of life with long-term control.
For simplicity, it has been discussed into following sections—(a) anti-asthmatic drugs, (b) management of acute attacks, and (c) long-term control of asthma.
I. Anti-asthmatic Medications
Anti-asthma drugs are broadly classified as: (a) Relievers for quick relief of symptoms, e.g. rapid-acting bronchodilators, (b) Maintenance drugs for use every day even in absence of symptoms (previously termed as controllers) including inhaled corticosteroids (ICS) and long-acting bronchodilators, and (c) Anti-inflammatory relievers (AIR), which contain combinations of both a low-dose ICS and a rapid-acting bronchodilator. Some commonly used drugs in bronchial asthma are as follows (Table 16.18).
• #946;-agonists act by increasing #946;-adrenergic activity via adenylate cyclase activation and include short-acting (SABA), e.g. salbutamol or terbutaline, and long-acting (LABA), e.g. salmeterol or formometerol. SABA are preferred as relievers for acute exacerbations while LABA are used for maintenance in children gt;4 years. LABA should never be used alone, always as inhalers in combination with ICS. Non-selective adrenergics, e.g. adrenaline or isoprenaline are rarely used due to cardiovascular side effects.
• Anticholinergic agents, e.g. ipratropium bromide, inhibit vagus-mediated bronchoconstriction and potentiate bronchodilatory action of #946;-agonists, mainly used as second-line reliever in refractory acute attacks. Another anticholinergic-Tiotropium bromide inhaler, may be used for maintenance in severe uncontrolled asthma above the age of 6 years.
• Corticosteroids, as potent anti-inflammatory agents, are cornerstone of maintenance therapy in asthma, generally used in inhaled form (ICS) including shortacting beclomethasone or long-acting budesonide or fluticasone. However, systemic steroids, e.g. hydrocortisone or prednisolone are also used as rescue therapy in severe acute exacerbations to minimize the need for hospitalization and suppress late reactions.
• Leukotriene inhibitors (LTRA), e.g. montelukast or zafirlukast antagonize late-phase reactions and thus have synergistic effect with steroids. These drugs are used either alone or along with steroids in—(a) long-term management of mild/moderate persistent asthma, or (b) prevention of exercise-induced asthma.
• Xanthine derivatives, e.g. aminophylline (85% theophylline) inhibit phosphodiesterase - a cyclic AMP degrader enzyme to raise cyclic AMP activity and inhibit release of inflammatory mediators. These drugs are generally avoided in children except as: (a) second-line drug for acute exacerbations in children gt; 5 years, and (b) adjunct therapy for control of nocturnal symptoms in moderate to severe persistent asthma.
Being a drug with thin safety margin, IV Aminophylline therapy should be use cautiously, closely monitored with serum drug levels (lt;10 pg/ml). Loading dose should not be used in cases, who had received aminophylline in last 72 hours.
• Mast cell stabilizers, e.g. cromolyn sodium, nedo- chromil sodium, ketotifen, etc. prevent release of chemical mediators from sensitized mast cells on allergen exposure. These drugs are rarely used to prevent acute exacerbations but have no role in treatment of established attacks.
• Other drugs used in asthma include IV magnesium sulphate-a smooth muscle relaxant, used in acute exacerbations, and IV Omalizumab - an anti-IGE antibody, used for maintenance therapy in severe refractory asthma.
Aerosol therapy is a novel drug-delivery system, which has revolutionized the management of asthma. An aerosol is a suspension of the drug in gaseous medium, which is directly deposited in lower airways on inhalation via special devices
| TABLE 16.18: Common Anti-asthmatic medications in children | ||
| Drugs | Doses | Side effects |
| A. Selective #946; agonists | ||
| Salbutamol Terbutaline Salmeterol Formoterol | MDI/DPI 1—2 puff 4-6 hrly Neb: 0.15 mg/kg/dose PO 0.1 -0.2 mg/kg/d q8hr MDI 1-2 puffs 4-6 hrly PO 0.15 mg/kg/d q8hr MDI/DPI 1-2 puffs 12-24 hrly MDI/DPI 1-2 puffs 12-24 hrly | Tremors, tachycardia Hypokalemia, hyperglycemia, Freon effect Long - acting salmeterol or Formometerol should never be used alone, always as inhalers in combination with ICS |
| B. Anticholinergics | ||
| Ipratropium bromide | MDI 1-2 puffs 8 hrly Neb: 0.5 mg/dose | Dry mouth, tachycardia |
| Tiotropium bromide | MDI 1-2 puffs 12 hrly | Only in children gt; 6 years |
| C. Steroids | ||
| Beclomethasone* Budesonide* Fluticasone* | LD 100-200, MD 200-400, HD gt;400 pg/day q12hr LD 100-200, MD 200-400, HD gt;400 pg/day q12hr LD 50-100, MD 100-200, HD gt;200 pg/day q 12-24hr | Oral thrush, cough, dysphonia Growth failure ? |
| Hydrocortisone Prednisolone | IV 25-100 mg stat dose PO 1-2 mg/kg/day q12-24hr | None, short-term use |
| D. Xanthine derivatives | ||
| Aminophylline | IV 5 mg/kg (L) gt; 1 mg/kg/dose q6hr** PO 5-15 mg/kg/d q12hr | Tremors, seizures, tachycardia Toxic level gt; 20 pg/ml |
| E. Leukotriene receptor antagonists | ||
| Monteleukast | PO 4 mg/day (2-5 yr) 5 mg/day (5-12yr) 10 mg/day (gt;12 yr) | Well tolerated except rare risk of quot;Churg-Strauss syndromequot; |
| F. Mast cell stabilizers | ||
| Sodium cromoglycate Ketotifen | 1-2 puffs q 6-8hr 1 mg q12hr | Reflex cough, bitter taste Sedation, weight gain |
*For children 6-11 yrs, Higher (Double) doses for adolescents gt; 12 years
LD: Low dose; MD: Medium dose; HD: High dose
**diluted 10 times in NS, infused over 15-30 minutes slowly. No loading dose, if received aminophylline in preceding 24 hours.
As only a particle size of lt;5 mm can cross mechanical airway barriers, lt;10-15% of inhaled drug reaches the lower airways by these devices. However, major benefits of this delivery system accrue from the fact that the drug is directly delivered at the target site with: (a) rapid onset of action, and (b) minimum side effects.
Aerosol devices may be: (i) propellent driven, e.g. metered dose inhalers (MDI), and (ii) inspiration driven, e.g. nebulizers or dry powder inhalers (DPI) (see Ch 32.5 for details). Choice of the aerosol device depends on the age and cooperation from patient, as follows:
• Nebulizer, for acutely sick, breathless child, when large doses are to be delivered and child cannot cooperate.
• MDI, for domicilliary treatment in children gt;6 years, who can coordinate press-breathe act.
• MDI with a spacer, for domicilliary treatment in children between 3-6 years, who cannot co-ordinate, but can breath through a mouthpiece.
• MDI with spacer and face-mask, for children lt;3 years, who cannot breathe through a mouthpiece.
• DPI for children gt;3 years, who cannot coordinate, but can breath through a mouthpiece.
II. Management of Acute Exacerbation
Asthmatic exacerbations denote an acute or sub-acute deterioration in symptoms and airway obstruction from the baseline, usually following exposure to an external trigger, (e.g. upper respiratory infection, pollution) or poor adherence to controller medications. Most of these attacks can be managed at home and hospitalization is required only in severe/non-responding cases.
A. Home treatment should be based on a written individualized protocol and includes:
• Recognition of impending attack and assessment of its severity by PEFR. A PEFR of lt;80% of personalbest PEFR indicates acute attack (lt; 50% in moderate to severe attack).
• Use of inhaled SABA, i.e. salbutamol via MDI (100 mg/puff 4-10 puffs), every 20 minutes till response (max 3 doses).
Single maintenance and reliever therapy (SMART) with combined inhaler of high-dose budesonide- formoterol (400/12 #956;g) with 2 puffs and repeat after 5 minutes) is preferred choice for acute exacerbation of asthma in children gt; 5 years, adolescents and adults.
• Reassessment for clinical response and PEFR improvement at the end of one hour:
± Good responders (PEFR gt;80%, sustained for 4 hours) should continue SMART or inhaled SABA 4-hourly for next 2 days and double the dose of ICS, if taking.
± Partial responders or non-responders should visit the hospital as early as possible.
B. Emergency hospital visit is needed for all children with unsatisfactory response to home treatment, though many of them can be sent back after 4-6 hours of observation after initial treatment, if response is satisfactory. Important steps in the management of acute asthmatic exacerbations in hospital are as follows (Fig. 16.10):
Step I. Assessment of severity on admission on the basis of clinical features, PEFR and SaO2. As per GINA guidelines 2023, asthmatic exacerbations in older children (5-12 years) are classified as mild to moderate or severe (Table 16.19).
In younger children lt; 5 years, an exacerbation is considered as severe in presence of any of the following:
(a) altered sensorium, i.e. agitated, confused or drowsy,
(b) SaO2 lt;92%, (c) inability to speak in phrases, (d) pulse rate gt;150-180 bpm, (e) RR gt; 4#952;#8725;minute, (f) cyanosis, and (g) silent chest (No wheezing).
Step II. First-hour management depends on the severity of attack and includes:
• Oxygen therapy with nasal prongs/mask to achieve a target SaO2 of gt;94-98%. Immediate intubation and mechanical ventilation is needed in cases of impending respiratory failure.
• Nebulized SABA, e.g. Salbutamol (0.15 mg/kg diluted in 2 ml NS), every 20 minutes during first hour and then hourly till response. Inhaled Salbutamol delivered by MDI with spacer (4-10 puffs/20 minutes) is equally, if not more, effective alternative to nebulization. However, Spacer must be primed with at least 20 puffs before first use, to prevent sticking of the drug on the plastic body due to static charge.
• Nebulized Ipratropium bromide (250-500 #956;g#8725;dose), every 20 minutes in first hour and than 2-4 hourly, in severe attacks on admission, though may be considered in mild to moderate attacks with poor response to SABA nebulizations in first hour.
• First dose of systemic corticosteroids (rescue therapy) as PO Prednisolone (1-2 mg/kg/day q8h) or IV. Hydrocortisone (50-100 mg/dose), irrespective of the severity of exacerbation.

Fig. 16.10: Emergency management of acute asthmatic exacerbation.
Based on GINA Guidelines 2023
| TABLE 16.19: Severity of acute asthmatic attack in children gt; 5 years of age* | ||
| Parameter | Mild or moderate | Severe |
| Talks in.. | Phrases | #8739;#8739;Words |
| Preferred posture | #8739;#8739;Sitting | Sits hunch forward |
| Sensorium | Not agitated | Agitated |
| Respiratory rate | Increased | ||gt;30/min |
| Accessory muscles | Not in use | In use |
| Pulse rate (bpm) | #8739;#8739;#8804;120 | #8739;#8739;gt;120 |
| SaO2 | #8739;#8739;#8805;90% | #8739;#8739;lt;90% |
| PEFR (% Personal best) | #8739;#8739;#8805;50% | #8739;#8739;lt;50% |
| Presence of drowsiness, confusion and silent chest indicate life-threatening attack | ||
Source: GINA guidelines 2023.
*See text for assessment of severity in younger children lt; 5 years
• IV magnesium sulphate as a single infusion or high- dose ICS may be considered in selected severe exacerbations.
Step III. Reassessment of all patients at the end of one hour for clinical response and PEFR to decide further course of action. Response at this point is broadly classified as Good (PEFR gt;60%) and Poor (PEFR lt; 60%).
Step IVa. Management of good responders: Cases with good response at the end of one hour must be managed as follows:
• Observe for next 3-4 hours to exclude relapse of symptoms before discharge.
• Continue PO Prednisolone (1-2 mg/kg/d q8h), at home, for next 3-5 days.
• Continue SABA via MDI with spacer, at home, as required, along with ICS appropriate to the severity. SABA-only treatment at discharge is no longer recommended since the occurrence of exacerbation is a risk factor for future exacerbations.
SMART with severity-appropriate ICS-Formoterol is preferred on discharge to reduce the risk of further exacerbations.
• Counsel regarding adherence to therapy, avoidance of exacerbations and early recognition of the attack.
Step IV b. Management of poor responders: Cases with poor response at the end of first hour are in status asthmaticus and need to be hospitalized, if necessary in intensive care. Hospitalization is also recommended to all children with—(a) severe or life-threatening attack, (b) past history of multiple exacerbations requiring oral steroids or emergency room visits, and
(c) unreliable management at home. Important steps in the management of poor responders to first-hour management include:
• Continuous oxygen support and mechanical ventilation, if respiratory failure supervenes. Role of helium oxygen therapy or non-invasive ventilation is unclear.
• Continue nebulized SABA, e.g. Salbutamol 1-hourly (or as continuous nebulization) along with Nebulized Ipratropium bromide 2-4 hourly. If necessary, both drugs can be mixed together (Duolin®) in same solution.
• Continue systemic steroids as IV hydrocortisone (50-100 mg every 6-hourly) till switch-over to oral steroids is possible.
• IV magnesium sulfate may be used in refractory cases as single infusion of 40-50 mg/kg, over 20 minutes.
• IV aminophylline is not recommended in routine management of asthma exacerbations due to poor efficacy and safety profile. However, it may be used in very refractory cases as IV aminophylline 5 mg/ kg (loading dose), dissolved 10 times in normal saline and infused slowly over 10-15 minutes, followed by 1 mg/kg 6-hourly. Loading dose should not be given in cases who have received aminophylline in last 72 hours.
• Antibiotics are not routinely indicated, unless there is definite evidence of infection. LTRA and LABA have no role in management of acute asthma and sedatives are contraindicated.
Patients, who improved with these measures, must be stepped down to step II of management before considering the discharge as per step IVa.
III. Step-wise Long-term Management of Asthma
Long-term control of asthma aims to-(a) achieve good control of symptoms, and (b) minimize future risk of asthmatic exacerbations and involves:
• Initial assessment of the level of symptom control and risk of future exacerbations;
• Initiation of appropriate pharmacotherapy based on the initial assessment;
• Regular monitoring at home and periodic assessment at hospital, for the level of symptom control, adherence to the treatment and adverse effects of medications.
• Step-wise modifications in pharmacotherapy, according to the level of control.
• Preventive interventions, e.g. avoidance of triggering agents, immunotherapy and non-pharmacological methods.
A. Initial assessment: While acute exacerbation may be the first presentation of asthma in children, many cases present without current symptoms but with suggestive past history. Once the diagnosis of asthma has been made and the acute exacerbation has been controlled, all cases must be classified according to:
• Level of asthma symptom control as—(a) well- controlled, (b) partly-controlled, and (c) uncontrolled (Table 16.20).
• Presence or absence of risk factors for future exacerbations as follows:
- Uncontrolled asthma symptoms,
- One or more severe exacerbations in previous year,
- Start of the child's usual flare-up season
- Exposure to potential allergens/triggering agents, e.g. smoke, allergens, etc. and
Modified from GINA Guidelines 2023.
- Major psychological or socioeconomic problems
- Poor adherence with controller medications
- Co-morbidities, e.g. obesity, sinusitis
B. Initiation of appropriate pharmacotherapy involves use of maintenance medications at appropriate level of severity based on initial assessment regarding level of asthma symptom control and future risk of exacerbations. Table 16.21 provides preferred choices and alternative options for maintenance therapy, which differs in children above 6 years and in younger children In addition, intermittent use of SABA, e.g. MDI Salbutamol (100 #956;g) is necessary during acute exacerbations.
C. Regular assessment and monitoring must include daily home monitoring and periodic asthma-clinic follow-ups. All asthmatic children or their parents should keep a daily record of symptoms and PEFR at home and must be trained to: (a) recognize an acute exacerbation and its home management, and (b) to make minor modifications in controller therapy. All patients must also be followed up at least every 3 months in asthma clinic to assess the level of control and modify therapy. Follow-up after 7 days of acute exacerbation is advised in cases visiting emergency room or needed hospitalization.
D. Stepping-up and stepping-down of controller therapy depends on the periodic assessment with following general principles:
• Stepping-up of therapy is required any time, after observation of clinical response and inter-attack PEFR. As a thumb rule, need for reliever SABA on daily basis indicates poor long-term control and need for step-up therapy. Short-term step-up for 1-2 weeks may be required in otherwise controlled cases following during viral infections or potential allergen exposure.
• Stepping-down of therapy to a lower step is advised only after minimum 3 months of control.
E. Preventive interventions include avoidance of triggering agents, immunotherapy and non-pharmacological methods.
• Avoidance of allergens/triggering agents is often difficult and impractical in children, though following precautions may be helpful:
- Early recognition of viral infections, e.g. URTI and stepping-up of inhaled steroids or short-term use of oral steroids, to prevent exacerbation.
- Avoidance of allergens, as discussed in Chapter 8.4.1. Avoidance of many dietary items is often overemphasized, without scientific basis. However, a proven cause-effect observation with particular
Reliever therapy
SABA as required
LD-ICS: Low-dose inhaled corticosteroids (100-200 #956;g#8725;dose); MD-ICS: Medium-dose inhaled corticosteroids (200-400 #956;g#8725;dose); HD-ICS: High-dose inhaled corticosteroids (gt;400 #956;g^ose); LD-OCS: Low-dose Oral Corticosteroids; LTRA: Leukotriene receptor antagonist; LABA: Long-acting #946;-agonist, e.g. Formometerol or Salmeterol; SABA: Short acting #946;-agonist, e.g. Salbutamol; SMART: Single maintenance and reliever therapy; Very LD-ICS+F (Budesonide+Formoterol100/6 #956;g) or LD-ICS+F (Budesonide+Formoterol 200/6 #956;g)
*Add-on treatment includes anti-IgE antibody, very rarely used in children.
foodstuff may be an indication to avoid it. Canned foods with preservatives, coloring agents, etc. Should be avoided.
- Avoidance of triggering factors, e.g. passive smoking, strenuous exercise or drugs, e.g. aspirin.
- Diagnosis and treatment of co-existing illnesses, e.g. gastro-esophageal reflux, sinusitis, tuberculosis, etc.
• Immunotherapy, i.e. desensitization of the child to identified allergen (Chapter 8.4.1) is often unrewarding, though may be tried in selected cases of severe persistent asthma, where avoidance of identified allergen is not possible.
• Non-pharmacological approaches in long-term control of asthma include yoga therapy in older children, behavioral modification and patient education.
Outcome: While the natural course of asthma is unpredictable, most cases (gt;60%) become relatively symptom- free by the end of puberty due to growth of airways, less incidence of precipitating viral infections, better awareness about trigger factors and, probably autodesensitization. However, many cases recur in later life, especially those with following risk factors: (a) family history of atopy, (b) late onset disease, i.e. after 3 years of age, (c) severe disease with poor lung functions in childhood.
Difficult to control asthma is a term is used to denote cases, who do not respond well despite appropriate controller therapy, usually due to presence of comorbidities, poor adherence to treatment and constant allergen exposure. All these cases must be reviewed for these factors with appropriate remedial measures. However, some cases do not respond even after that and referred as “Refractory asthmaquot;. Management of them is best left to the experts.
16.9