ANEMIA-GENERAL CONCEPTS
Anemia is defined as a reduction in haemoglobin concentration below the age-related norms (Table 19.3).
NFHS-5 shows that about two-third of Indian children aged 6-59 months (67.11%) are anemic with Hb lt;11 gm/dl.
Prevalence of anemia in pregnant mothers at similar Hb cut-off is 52.2%.Etiology: Anemia is a clinical manifestation of imbalance between production and loss of RBCs, due to any cause (Table 19.4).
Production may be impaired due to bone marrow failure (Aplastic/hypoplastic anemia) or deficiency of various substrates required for production of Hb (Nutritional anemia).
Similarly, increased loss of RBCs may be due to acute or chronic bleeding (hemorrhagic anemia) or accelerated destruction in reticuloendothelial system (hemolytic anemia).
Pathophysiology: Irrespective of etiology, the prime event in anemia is impaired oxygen carrying capacity of blood with consequent tissue hypoxia. However, clinical manifestations do not appear until Hb levels drop lt;7-8 gm%, due to various compensatory physiological adjustments as follows:
• Hemodynamic adjustments with tachycardia, increased cardiac output and hyperdynamic circulation to maintain adequate O2 supply despite lower carrying capacity.
TABLE 19.3: WHO cut-off points (Hb%) for anemia-2011
• Shift of O2 dissociation curve towards right, i.e. reduced Hb affinity for O2 due to increase in 2,3-DPG concentrations in RBCs, which permits release of more oxygen at cellular level.
• Stimulation of EPO activity with increased erythropoiesis, which may or may not be effective, depending on marrow response and availability of substrates. It also stimulates extramedullary erythropoiesis in chronic anemia, e.g. hemolytic anemia.
Clinical presentation depends on the severity of anemia and rapidity of its development.
Primary indicators of anemia, irrespective of its etiology include:• Pallor is first visible over conjunctiva and oral mucus membranes and distribution of pallor is used to classify severity of anemia as per WHO classification.
Severity of pallor over palms is used to classify anemia under IMNCI guidelines as—(a) severe anemia, with severe palmar pallor, (b) some anemia, with some palmar pallor, and (c) no anemia, without palmar pallor.
• Signs of cellular hypoxia, e.g., easy fatigability, growth failure, lack of attention span, dizziness, etc.
• Signs of cardiac decompensation, e.g., tachycardia, collapsing pulse, functional murmurs, cardiomegaly, congestive cardiac failure, etc. ECG changes of myocardial hypoxia may be present in severe anemia, including depressed ST segment with flat/inverted T waves.
• Signs of compensatory erythropoiesis, e.g., hepato- splenomegaly, hemolytic facies and skeletal changes are most prominent in hemolytic anemia.
TABLE 19.4: Etiological classification of anemia
• Inadequate bone-marrow production
- Aplastic anemia
- Pure red cell aplasia
- Transient erythroblastopenia
- Chronic infections/inflammation/renal disease
- Marrow infiltration: Malignancies, storage disorders
• Substrate deficiencies (Nutritional anemia)
- Iron deficiency anemia
- Megaloblastic anemia (Folic acid, Vitamin B12)
- Other nutrient deficiencies (PEM, Vitamin C, Zn)
- Malabsorption syndrome
• Increased destruction (Hemolytic anemia)
- Intra-corpuscular (congenital)
#9830; Membrane defects: Hereditary spherocytosis
#9830; Enzyme defects: G6PD deficiency
#9830; Hemoglobinopathies: Thalassemia, sickle cell anemia
- Extra-corpuscular (acquired)
#9830; Autoimmune hemolytic anemia
#9830; Isoimmune hemolytic anemia
- Mechanical injury: Malaria, hemangioma, HUS
• Increased blood loss
- Acute: Trauma, surgery, systemic disease
- Chronic: Hook-worm infestation
HUS: Hemolytic uremic syndrome
TABLE 19.5: Broad etiological D/D anemia
LSES: Low socioeconomic status; FTT: Failure to thrive; HSMegaly: Hepatosplenomegaly
*Features may vary according to individual cause.
*Microcytic hypochromic or megaloblastic **Marked anisocytosis poikilocytosis.
In addition, signs of excessive hemoglobin breakdown, e.g., icterus and gall stones, are common in chronic hemolytic anemia; while signs of pancytopenia, e.g. bleeding or recurrent infections indicate aplastic anemia.
Clinical evaluation of anemia aims to classify probable etiology in four major groups—(a) nutritional anemia, (b) hemolytic anemia, (c) aplastic anemia, and (d) hemorrhagic anemia, to limit the diagnostic workup (Table 19.5).
• Important history in evaluation of anemia includes -
(a) age of presentation, (b) family history, (c) dietary intake including early infant feeding, (d) chronic infection, diarrhea or worm infestation, (e) chronic systemic illnesses, e.g. renal or liver disease, (f) recent or recurrent bleeding including minor mucocutaneous bleeds, (g) blood transfusions, and (h) others, e.g. limb pains, hematuria, jaundice, etc. History of perinatal events is important in newborns and early infancy.
• Important examination findings in these cases include severity of anemia and presence of failure to thrive, hepatosplenomegaly, jaundice, bleeding, etc.
Anemia due to hemorrhagic causes is usually obvious, though concealed internal organ bleeding or occult blood loss, e.g. helminthiasis must be excluded by relevant investigations.
Chronic infections, e.g. malaria or tuberculosis are important causes of anemia in Indian children due to multiple causative factors, e.g. nutritional deficiency, hemolysis and bone marrow suppression.
Figure 19.2 provides a simplified algorithm for clinical differential diagnosis of anemia in children, as a starting point for investigations.
Fig. 19.2: Clinical approach to anemia.
Laboratory investigations in anemia may be divided into two broad groups—(a) baseline investigations to screen for possible etiology, and (b) confirmatory tests, depending on the suspected cause.
Some baseline investigations are as follows:• Complete blood counts to assess the severity of anemia (Hb%) and identify possible etiology, e.g. bone marrow depression or chronic infections/ inflammatory disorders.
Assessment of RBC indices, i.e. mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular Hb concentration (MCHC) and red cell width (RDW) is very useful to limit diagnostic possibilities (Table 19.6).
± MCV (PCV/TRBC* ? 10), normally ranges between 80-90 femtoliters (fl), except in early infancy (~108 fl at birth). According to MCV, anemia is classified as microcytic, normocytic or macrocytic.
*(PCV: Packed cell volume, TRBC: Total RBC count).
TABLE 19.6: Morphological classification of anemia
• Microcytic hypochromic
- Iron deficiency anemia*
- Lead poisoning
- Thalassemia trait
- Pyridoxine deficient/dependent anemia
- SideroblasticZdyserythropoietic anemia*
- Othersquot; Copper deficiency,
• Normocytic normochromic
- Aplastic hypoplastic anemia
- Minor hemoglobinopathies or traits*
- Acute/chronic blood loss
- Chronic infections/Inflammations/renal disease
- Auto-immune hemolytic anemia*
• Megaloblastic
- Vitamin B12 deficiency*
- Folic acid deficiency*
- Myelodysplasia
- Others: Liver disease, orotic aciduria
• with anisocytosis, i.e. increased RDW
- MCH (Hb/TRBC) normally range between 28-34 picograms/cell. According to MCH, anemia is classified as normochromic or hypochromic.
- MCHC (Hb/PCV ? 100) normally ranges between 32-36 gm/dl. Hereditary spherocytosis is the commonest cause of elevated MCHC, but may also be seen in autoimmune haemolytic anemia or some hemoglobinopathies. It is reduced in iron deficiency.
- RDW: Major hemolytic and nutritional anemia are also associated with marked anisocytosis quantified by RBC distribution width (RDW)-a coefficient of variation in RBC size on electronic counters. Normal RDW is ~12-14%, which is increased in iron deficiency anemia (Low MCV), Hemoglobinopathies (normal/low MCV) or megaloblastic anemia (high MCV).
Mentzer index (PCV/TRBC) is also interpreted similarly.• Peripheral smear (PS) is an extremely valuable screening test in etiological diagnosis of anemia. A freshly prepared and stained (hematoxylin- eosin) smear should be examined not only for RBC morphology, e.g. shape, size, color and inclusion bodies, but also for leukocyte or platelet abnormalities to exclude leukemia and aplastic states.
Normal RBC is a non-nucleated cell, which is biconcave in shape with central pallor. Common RBC abnormalities on smear include (Fig. 19.3):
- Abnormal size, e.g. microcytosis, macrocytosis or anisocytosis, which should be confirmed by MCV and RDW values.
- Abnormal shape, e.g. poikilocytosis (variable shape) or irregular-shaped RBCs (Schistocytes or Burr cells) usually indicate hemolytic anemia due to any cause. Specific diagnosis of many hemolytic disorders, e.g. sickle cell anemia and RBC membrane defects, e.g. hereditary spherocytosis/elliptocytosis is possible on abnormal cell morphology.
- Abnormal color, e.g. hypochromia (increased central pallor, occupying gt;1/3rd area) indicates iron deficiency while presence of polychromasia (irregular staining) or target cells (central pink area, surrounded by colorless zone and then rimmed by a pink border) suggests hemolysis. Hyperchromia, i.e. absence of central pallor, is caused by altered shape or thickness of RBC membranes and not due to higher Hb content.
- Abnormal inclusion bodies within RBCs usually include parasites, e.g. malaria or kala-azar, basophilic stippling, i.e. small blue/black granules signs of lead poisoning and Howell-Jolly bodies, i.e. small round dark-blue remnant nucleus near the periphery of cell signs of asplenia, hyposplenism or splenectomy.
- Presence of nucleated RBCs, i.e. normoblasts indicate hemolytic anemia.
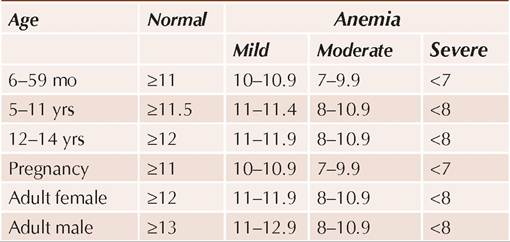
Fig. 19.3: Common peripheral smear abnormalities of RBCs.
Reticulocyte count: Reticulocytes are immature RBCs, with spoked-wheel appearance on special cresyl blue staining of peripheral smear (Fig.
19.4). Normal reticulocyte count does not exceed 2%, except at birth. Reticulocyte production index (RPI) or corrected reticulocyte count {Retic count ? observed Hb/normal Hb ? 0.5} is a better indicator of bone marrow activity. RPI of gt;3 is an indicator of rapid RBC turnover in hemolytic anemia, blood loss or iron therapy, while RPI of lt;2 indicates intrinsic bone marrow failure, e.g. aplastic anemia.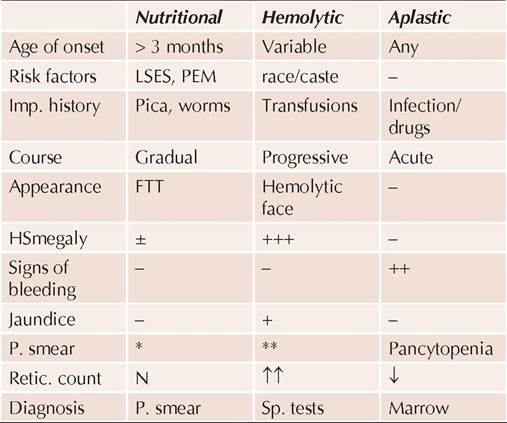
Fig. 19.4: Reticulocytes.
• Biochemical tests, e.g. iron studies or vitamin B12/ folate levels are indicated in assessment of nutritional anemia, while hemoglobin electrophoresis is required for suspected hemolytic anemia or unexplained anemia refractory to treatment. Other laboratory investigations are also required based on clinical suspicion, discussed in relevant chapters.
• Bone marrow examination is indicated in cases of suspected aplastic anemia or myeloinfiltrative disorders, e.g. leukemia, which should be examined for—(a) cellularity, (b) myeloid:erythroid ratio (N: 2-3:1), (c) parasites, and (d) abnormal stainings, specially for hemosiderin (for procedure see Ch 29.6). Hypocellular marrow with reduced M:E ratio indicates aplastic anemia while reverse indicates hyperactive marrow in hemolytic anemia.
19.3
More on the topic ANEMIA-GENERAL CONCEPTS:
- Drug-Induced Hemolytic Anemia
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Polyarteritis Nodosa
- REFERENCES
- Chapter 8 Maternal medicine and infections
- Scaling Worker Cooperatives as an Economic Justice Tool for Communities in Crises