BRAIN ABSCESS
Brain abscess is a serious and focal CNS infection, mainly seen in cerebral cortex, though 20% of them may develop in cerebellum or brain stem.
Etiopathogenesis: Brain abscesses may be caused by: (a) Infected embolization from extracranial sites, e.g.
infective endocarditis, cyanotic heart diseases, orodental infections, (b) Direct spread from neighboring infections, e.g. mastoiditis and otitis, orbital cellulitis, CSF shunts and penetrating head injuries, and rarely as (c) Residual lesions following meningitis. Multiple abscesses are seen in ~ 30% cases.Causative organisms in India generally include: (a) Gram-positive cocci, e.g. Staph. aureus, S. viridans, S. pneumoniae, (b) Anaerobic infections, e.g. bacteroides, (c) Gram-negative bacilli, e.g. H. influenzae, Pseudomonas, etc., and (d) Fungal infections in immunocompromised children. Nearly 30% brain abscesses are polymicrobial in etiology.
Clinical features of brain abscess depend on its location, though general features include:
• Constitutional features, e.g. fever and toxemia.
• Signs of raised ICP, e.g. headache, vomiting, papilledema.
• Focal signs, e.g. seizures, ataxia, etc.
• Altered sensorium, e.g. irritability, drowsiness, etc. However, coma is uncommon till terminal stages.
Diagnosis depends on presence of cerebritis or abscess on CT/MRI (Fig. 18.14). Cerebritis appears as a parenchymal low-density lesion, while abscess appears as ring-enhancing lesion on contrast CT, with/without mass effect. CSF exam is rarely useful and should be avoided, due to potential risk of brain herniation in presence of raised ICP.
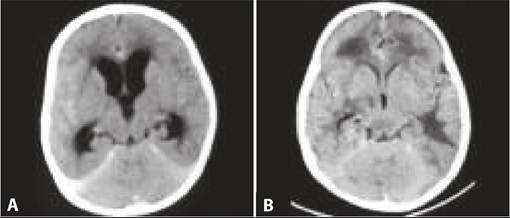
Fig. 18.14: Brain abscess.
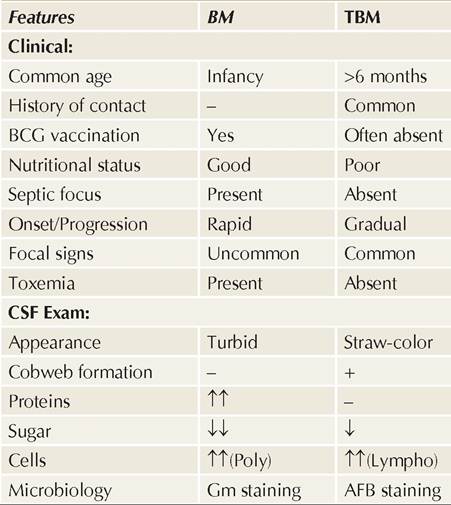
Fig.
18.15A and B: Tuberculoma.(A) Plain CT; (B) Contrast CT
granuloma, formed during hematogenous spread of pulmonary lesion.
Clinically these cases may be asymptomatic for many years or present like other ICSOLs, with recurrent seizures, hydrocephalus with raised ICP or focal neuro-
logical deficits.
TABLE 18.33: Intracranial space occupying lesions
• Infective:
- Tuberculoma
- Brain abscess
- Parasitic: Neurocysticercosis, toxoplasmosis*
• Neoplastic: Brain tumors, secondaries
• Vascular: Sturge-Weber syndrome, vein of Galen malformation
• Traumatic: Subdural hematoma
• Developmental: Hydranencephaly, porencephaly
• specially in immuno-compromised host, e.g. HIV.
D/D includes other causes of ICSOL (Table 18.33), though presence of constitutional signs, e.g. high fever with chills and toxemia are highly suggestive of brain abscess in a case with focal neurological deficit.
Management includes IV antibiotic therapy with a third generation cephalosporin and metronidazole for 4-6 weeks. Vancomycin must be added in abscesses following head trauma, surgery or CSF shunts (suspected staphylococcal etiology). Follow-up neuroimaging is necessary to ensure that abscess is decreasing in size.
Surgical drainage is risky due to neurological morbidity, but indicated in cases with—(a) size more than 2.5 cm or evidence of mass-effect, (b) presence of gas or septations in the cavity, (c) suspected fungal etiology, or (d) poor response to antibiotics after 4-6 weeks.
18.12.7
More on the topic BRAIN ABSCESS:
- INTRACRANIAL INFECTIONS
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Cerebellum and Hindbrain
- Focal Segmental Glomerulosclerosis
- Etiopathogenesis
- Dental
- Macrovascular Complications of Diabetes Mellitus