BREASTFEEDING
Breast milk (BM) is the only food that a baby needs unto first 4-6 months of life and gives the best possible nutritional start to the neonate. Exclusive breastfeeding (BF) means that the neonate gets only breast milk and nothing else like honey, water, juices, tonic and medicines (unless prescribed) or any other animal milk.
5.2.1 COMPOSITION OF BREAST MILK______________
Volume output and composition of BM changes throughout lactation period to meet changing needs of growing infants.
Daily milk output in Indian mothers is ~30-60 ml during first 3 days of life (colostrum) that gradually peaks at ~2 months (600-700 ml) followed by gradual decline from 6-7 months onwards to lt;500 ml by one year and lt;300 ml by two years.
Colostrum is the thick yellow and sticky milk, produced during first 72 hours of life. Although secreted in small quantities, it is enough to meet the newborn's requirement during this period. Colostrum is not only rich in proteins and anti-infective factors, but also facilitates maturation of gastro-intestinal tract.
Transition milk is secreted between 3rd and 14th day. It has lesser protein and immunoglobulin content than colostrum, but relatively higher fat and sugar content to meet increasing energy requirements.
Mature milk, secreted from 15th day onwards, has further less proteins than the transitional milk, but more volume, fat and caloric content. Composition of mature milk also varies according to maternal diet as well as even during the course of a single breastfeed, as follows: Fore milk flows at the start of each feed and is relatively watery to satisfy the baby's thirst, with lesser fat content, but rich in sugars, vitamins and minerals.
Hind milk, secreted in later part of feeding, is thicker than the fore milk with higher fat content to satisfy the baby's hunger and caloric needs.
Preterm milk from mothers of a preterm baby during first few days is qualitatively different from milk of term-mothers, with higher energy density, proteins and sodium content to meet their higher requirements. Preterm milk also contains less lactose and solutes, to adjust for maturational lactase deficiency and relative renal insufficiency in them. It achieves composition of term milk by 4-6 weeks.
5.2.2 ADVANTAGES OF BREASTFEEDING
Breast milk is species-specific, i.e. quantitatively and qualitatively most appropriate for human baby. Apart from nutritional superiority, breastfeeding also offers many other advantages to baby, mother, family and even to the community, as follows:
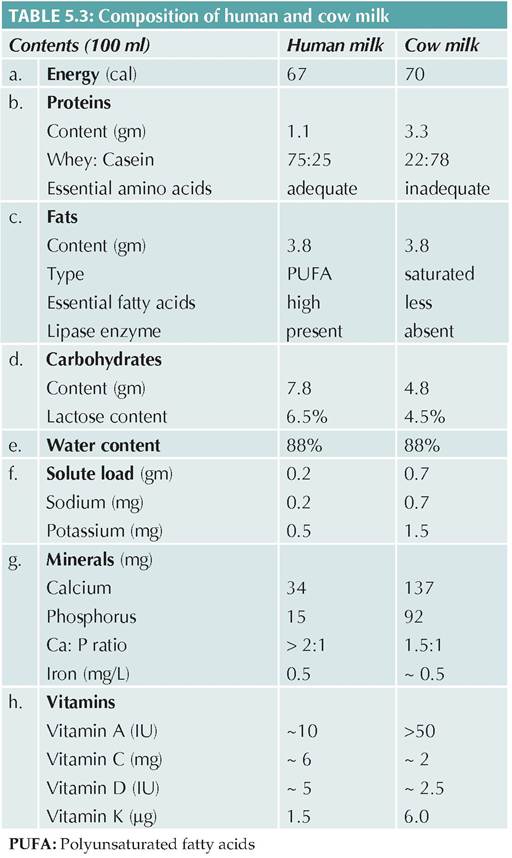
A. Nutritional superiority: BM is easily digestible and contains all essential nutrients in the right quantity and quality, as per baby's requirements (Table 5.3). Major nutritional advantages of BM are as follows:
• Energy from BM is mainly derived from easily digestible carbohydrates, e.g. lactose.
• Protein content in BM, though less than in cow milk, is qualitatively superior due to:
- Better whey-casein ratio: 75% of human milk proteins are easily digestible whey proteins or lactalbumin, unlike casein-rich cow milk, which is difficult to digest due to curd formation.
- Essential amino acids (EAA): BM contains all EAAs in appropriate concentrations to facilitate proper cognitive development, (e.g. taurine and cysteine), which are lacking in cow milk.
- High protein content in animal milk increases risk of allergic disorders, due to absorption of macromolecules through immature gut mucosa.
• Fat content in BM is quantitatively comparable to cow milk, but with better quality, i.e. higher PUFA and EFA content. Cow milk is richer in saturated fats, which are difficult to digest and increases the risk of hypertension or heart disease in adult life. Human milk also contains lipase enzyme, essential for fat absorption.
• Vitamin contents in BM is adequate (except vitamin K), while cow milk is deficient in vitamins C and D. While low vitamin K content in BM is responsible for higher risk of hemorrhagic disease of newborn in breast-fed babies, it may be easily prevented by single dose prophylactic vitamin K supplement at birth.
• Mineral (ash) content of BM is much lower (1.5%) than in cow milk (gt;7.0%). High ash content in cow milk poses additional solute burden over developing kidney with limited concentration capability.
- Iron content in BM is comparable to cow milk, but BM iron is better absorbed (~50%) than cow milk iron (10%), due to lesser phosphate load.
- Calcium content is lesser in BM, though BM calcium is better absorbed and utilized due to appropriate Ca: P ratio. Consequently, tetany is less common in breastfed children.
• Water: BM contains adequate water (88%) and hence, no additional water is required in exclusively breastfed babies, with less risk of infections.
B. Anti-infective properties: BM is essentially sterile, except in presence of systemic or local (breast) maternal infection. Further, presence of various anti-infective substances in BM is responsible for lower incidence of gut and respiratory infections in breastfed infants. These factors include:
• Humoral factors, e.g.
- Non-specific and specific IgG antibodies
- Secretory IgA, for local immunity
• Cellular factors, e.g.
- Phagocytic cells, e.g. macrophages
- Cellular-release factors, e.g. lysozymes
• High complement activity
• Organism-specific protective factors, e.g.
- Para amino benzoic acid (PABA) against malaria
- Anti-staphylococcal factor
• Others, e.g.
- Bifidus factor, to facilitates the growth of Lactobacillus bifidus in gut and prevents pathogenic colonization,
- Lactoferrin, to binds the iron in gut and inhibit growth of pathogenic bacteria, e.g. E. coli, which need iron for their metabolism.
- Lower pH of BM prevents bacterial overgrowth.
C. Emotional bonding: Breastfeeding creates an emotional bond between baby and mother, necessary for future growth, development, and parent-child adjustment.
D. Advantages to mother include:
• Enhanced oxytocin secretion to facilitate placental expulsion and uterine involution with less risk of post-partum hemorrhage.
• Convenience and less workload, obviating the need for boiling/mixing the top-milk. She also does not have to worry about the milk supply and spoilage.
• Natural contraception: Lactational amenorrhoea due to high prolactin levels is common during first 6 months, with ~98% protection.
• Lower incidence of breast and ovarian cancers.
• Cosmetic recovery with faster regaining of figure, due to more caloric consumption.
E. Advantages to family: Breastfeeding is a good economic practice for family as well, due to:
• Negligible cost, except the hidden expenses for additional nutrition to mother.
• Less health care expenses, due to lesser morbidity.
• Natural family spacing.
F. Advantages to the community include:
• Ecological benefits due to less consumption of natural resources for animal-milk production (fodder), boiling (fuel) and washing the utensils (water).
• Lesser morbidity in infants with less public health expenses.
• Population control, due lactational amenorrhoea.
5.2.3 PHYSIOLOGY OF LACTATION
Anatomically, the breast is made up of glandular tissue, supporting tissue and fat (Fig. 5.1). There are ~20-25 alveoli in each breast, each lined by epithelial cells and surrounded by myoepithelial cells. Milk is secreted in alveoli by epithelial cells and pushed forward by contraction of myoepithelial cells. Each alveoli drains its output via lactiferous tubules and ducts into ~ 10-15 lactiferous sinuses, which lie below the areola and open out onto the nipple. The size of the breast depends on the amount of fat and supporting tissue and does not reflect on the milk-producing capacity.
Physiologically, lactation depends on two interdependent processes in mother: (a) production of milk (prolactin reflex), (b) secretion or ejection of milk (oxytocin reflex), as well as (c) actual sucking by the baby, dependent on neonatal reflexes.
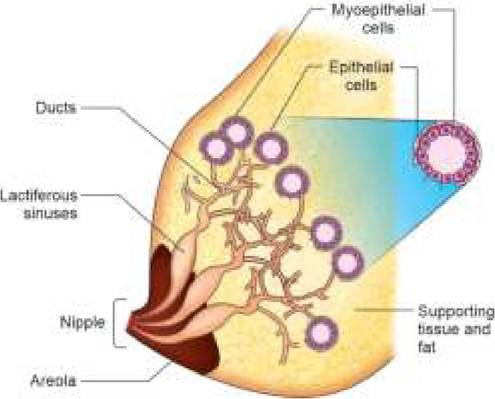
Fig.
5.1: Normal breast anatomy.- Rooting reflex helps the baby to latch onto the nipple. When the breast or nipple touches the baby's chin, philtrum, upper lip or cheek, the baby opens his/ her mouth to search for the nipple.
- Suckling reflex helps the baby to draw milk by converting the nipple and areola into a teat pressed between the lower jaw and hard palate. Wavelike movements of tongue facilitate sucking. For successful lactation the baby must be well attached to the breast, with the nipple and most of the areola in his mouth.
- Swallowing reflex: After every 2-3 sucks, collected milk is swallowed by baby, followed by deep breath. Each suck-swallow-breathe cycle lasts for ~2-3 second.
5.2.4 CORRECT BREASTFEEDING TECHNIQUES AND PRACTICES
• Production of milk (Prolactin reflex): When a baby sucks, afferent impulses from nipple stimulate prolactin secretion from anterior pituitary. Prolactin acts on the milk-producing alveolar epithelial cells to stimulate milk secretion. Thus, the prolactin reflex depends on how early, how often and how strongly the baby sucks.
- Prolactin activity and milk production is facilitated by: (a) adequate emptying of breasts after each feed, (b) early onset of lactation, (c) frequent suckling, (d) expression of breast milk, and (d) night feeds.
- Prolactin secretion is inhibited by: (a) pre-lacteal feeds, (b) incorrect positioning, and (c) painful breast conditions, (d) physical or mental stress to mother.
• Milk ejection/let down (Oxytocin reflex) is also initiated during suckling when afferent impulses from nipple reach the posterior pituitary to stimulate oxytocin production. Oxytocin contracts the myo-epithelial cells surrounding the alveoli and lactiferous sinuses, to push the milk forward towards the nipple. The squeezing sensation in the breast during breastfeeding is a sign of a good “let-down reflexquot;. Oxytocin secretion is affected by the physical and mental state of the mother.
- Oxytocin activity and milk ejection is enhanced by: (a) sight and sound of baby, (b) pleasant thoughts of baby, and (c) maternal confidence in her ability to breastfeed.
- Oxytocin secretion and milk ejection is reduced by:
(a) mother's anxiety or low-confidence, (b) mental stress or worry, and (c) pain or discomfort during breastfeeding.
• Actual sucking by baby (Neonatal reflexes): Three neonatal reflexes, i.e. sucking, swallowing and rooting reflex, participate in milk extraction during breastfeeding.

Fig. 5.2: Breast crawl.

Fig. 5.3: Good attachment (latching) on breast.
• Rooming in, i.e. keeping the baby with the mother in the same room and on the bed helps to maintain the baby's temperature, initiate and maintain breastfeeding and develop emotional bonding.
• Schedule/ frequency of feeding: Baby should be fed as and when required, i.e. demand feeding, rather than to fix-up a scheduled feeding. In fact, a normal baby itself develops a flexible schedule by the end of 2 weeks, when she/he demands the feeds ~2-3 hourly.
If a baby demands more frequently, it is possible that either: (a) the duration of feeding is too short or
(b)she/he is getting only foremilk.
• Hygiene: There is no need to wash breasts before feeding, though general hygiene by daily bath should be maintained.
• Environment: Baby should be breastfed in a peaceful and tension-free environment, without hurry and worry of domestic chorus, to avoid forcible interruptions during breastfeeding and consequent problems.
• Breastfeeding position: Any BF position is acceptable, provided mother is comfortable and baby is well- attached to the breast. Some commonly used positions are:
± Indian position, i.e. mother sitting cross-legged, with a back support.
± Cradle position, i.e. mother cradling the baby in her arms with the forearm supporting his/her head.
± Football-hold position is useful to feed the twins. In this, the baby is held under the arm of mother with feet pointing backward, abdomen touching mother's chest and body supported by mother's arm.
± Side-lying position is useful for night feeds, BF in immediate post-cesarean period and in sick mother. Mother and baby lie down facing each other with mother's hand supporting baby's back.
± Supine position is helpful in post-cesarean period or when milk-flow from the breast is in excess to the baby's speed of sucking. In this, mother feeds in supine position with baby held onto her abdomen.
Signs of a good breastfeeding position are:
1. Baby's whole body is supported, not just the neck or shoulders,
2. Baby's head, neck and body are in straight line, without any twist or bending. Head can be slightly extended to bring chin closer to the breast,
3. Baby is held close, with body turned toward mother and abdomens touching each other,
4. Baby should be facing the breast, with nose at the level of mother's nipple.
• Proper attachment of the baby at the breast is essential to prevent painful nipple problems in mother as well as to ensure adequate intake by baby.
Signs of good attachment include (Fig. 5.3):
1. Baby's mouth is wide open,
2. His/her lower lip is everted,
3. His/her chin is touching the mother's breast,
4. Most of the mother's nipple and areola is inside his/her mouth, except a small of upper areola. No part of lower areola should be visible.
• Effective sucking: Normally baby suckles 2-3 times by pressing the areola with the tongue against the hard palate to squeeze-out the milk, before pausing to swallow the collected milk.
Signs of effective sucking include:
1. Baby's cheeks are full and not hollow,
2. Baby is calm and relaxed,
3. Mother does not feel any pain.
• Duration of each feed should be decided by the baby (some are fast-feeders while others are slow-feeders) and she/he should be allowed to release the breast on its own. As a baby needs both-the watery foremilk to satisfy the thirst as well as the fatty hind-milk to satisfy the hunger, one breast should be emptied first before the other is offered. In case, baby is unable to empty

Fig. 5.4: Burping.
both breasts at one time, other breast should be offered first during subsequent feeding.
• Burping: Babies swallow lot of air during BF, especially if not properly attached to the breast. This aerophagia, may lead to abdominal discomfort, colic, regurgitation of feeds and rarely, aspiration. Burping by placing the baby over shoulders in upright position for 5-10 minutes with gentle stroking of back after feeds, helps to evacuate swallowed air (Fig. 5.4).
• Expression of breast milk is advised in cases of: (a) painful breast engorgement, (b) any contraindication for breastfeeding (to discard), or (c) separation of mother and baby due to sickness or other causes. (see Ch 5.4.1)
5.2.5 COMMON BREASTFEEDING PROBLEMS
Common BF problems may be broadly divided into three categories: (I) breast and nipple problems, (II) partial or complete lactation failure, and (III) breastfeeding in special situations, e.g. sick mother, sick baby or working mother.
I. Breast and nipple problems are very common and often used as an excuse to start top-feeding, despite adequate milk output. These problems are more common in primipara mothers and include:
• Flat or inverted nipples may prevent proper attachment of baby to the breast. Flat nipples become prominent when pinched at base, while inverted nipples go in. These problems can be easily identified by antenatal breast examination. Flat nipples usually do not pose any feeding problems and can be managed easily by assuring mother and some modification in feeding positions. Persistently flat or inverted nipples may be managed by: (a) nipple-stretching exercises
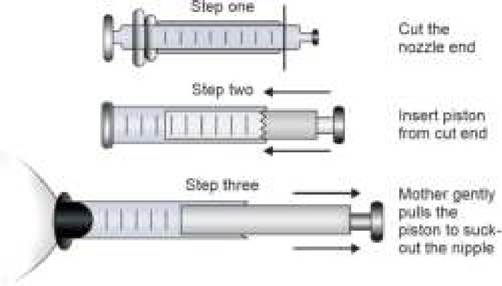
Fig. 5.5: Syringe method for AatZinverted nipples.
(pulling the nipple and rolling it between fingers), (b) use of a breast pump to pull the nipple out before every feed, or (c) syringe method.
Syringe method (Kesri method) is a simple suction device, prepared by cutting the nozzle end of a syringe and inverting its piston (Fig. 5.5). When the smooth end of syringe is pressed against the nipple and piston is pulled gently, the inverted nipple pulls out of the breast tissue. This should be done before each breastfeed.
Sore nipples are painful, tender nipples with or without cracks or bleed, caused by: (a) wrong posi- tioning/attachment of baby on the breast, (b) forcible separation of baby while sucking, (c) repeated washing of breasts with soap solutions before feeds, (d) local fungal infections (thrush).
Sore nipples are managed by: (a) correct posi- tioning/attachment of baby, (b) starting each feed on the less affected breast, (c) application of hind-milk on the nipple as emollient, and (d) local anti-fungal treatment, if necessary.
Breast engorgement indicates inadequate expression of milk despite adequate production, leading to hard, painful, warm and swollen breasts. It is usually caused by infrequent breastfeeding due to: (a) delayed initiation at birth, (b) maternal/neonatal sickness or (c) painful breast and nipple conditions (Fig. 5.6).
Most of these cases are self-limiting and can be prevented or managed by: (a) frequent demand feeding, (b) frequent expression of milk, if baby/mother is sick, and (c) local hot-water compresses to relieve pain.
Breast abscess (mastitis) may develop due to infection of engorged breast, with cracked nipple as a portal of entry for infection (Fig. 5.6).
These cases are treated with: (a) antibiotics and surgical drainage, (b) symptomatic therapy with analgesics and hot compresses (breast massage should be avoided), and (c) frequent expression of milk, which may then be fed to the baby.
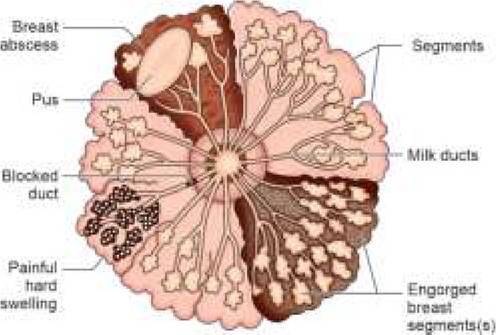
Fig. 5.6: Common painful breast conditions.
II. Lactational failure is defined as low milk output in the mother, inadequate to meet baby's requirements. It may be primary since delivery or secondary after successful initiation of breastfeeding at birth; partial or complete; transient or permanent; and true or perceived.
Causes: True lactation failure is extremely rare. In most cases, it is a consequence of complex cycle, involving temporary delay in the initiation of BM output due to any cause gt; maternal anxiety gt; wrong advice from others gt; initiation of supplementary feeds gt; reduced frequency and duration of BF gt; further decrease in milk-output (Table 5.4).
Management of lactation failure mainly aims to boost mother's confidence in her ability to breastfeeding, eliminate causative factors and advise correct breastfeeding practices. Continuous monitoring is necessary to prevent recurrence of problem. Important steps in lactation management include:
Step I. Assess the BM output, which is probably adequate if: (1) baby is gaining adequate weight, i.e. ~20-30 gm/day after 10th day; (2) baby is passing the adequate urine, i.e. ~6-8 times a day; (3) baby is sleeping comfortably for 1-2 hours after breastfeeding; (4) mother feels a sense of fullness in the breast before next feed time; (5) milk starts dripping from other breast, when the baby is sucking on one breast. Test weighing, i.e. weighing the baby before and after feeds, is rarely required.
Step II. Reassure and counsel the mother, if milk output is adequate. Let her understand the indicators of adequate BM output (as above).
Step III. Identify and eliminate causative factors, e.g. local breast/nipple problems, improper attachment, wrong feeding practices, misguidance from others, partial bottle-feeding or maternal illness. Identification of the cause requires detailed history of family environment and breastfeeding practices, observation at the time of BF and physical evaluation of mother/baby.
Step IV. Boost the milk output: Many galactagogues, e.g. special foods, herbs, (e.g. satavari), drinks or
TABLE 5.4: Causes of lactation failure
I. Psychological causes (4 oxytocin activity)
- Lack of self-confidence
#9830; Primigravidas and teen mothers (inexperience)
#9830; Unsuccessful breastfeeding in earlier pregnancy
#9830; Inadequate antenatal counseling
- Physical or mental stress
#9830; Mental anxiety or worry
#9830; Physical stress, e.g. working mothers
#9830; Wrong advice/counseling from family
II. Incorrect breastfeeding practices (4 prolactin activity)
- Prelacteal feeds and delayed onset of breastfeeding
- Infrequent or less vigorous breastfeeding
#9830; Painful breast or nipple conditions
#9830; Weak or preterm baby
#9830; Schedule feeding
#9830; Wrong positions or attachment
III. Physical causes (true lactation failure)
- Extreme maternal undernutrition
- Extremely sick mother
medications, (e.g. PO metaclopramide 10-15 mg TDS) are claimed to increase milk production by stimulating prolactin secretion. However, most of them have only placebo effect.
The best galactagogue is a nutritious diet to mother and a healthy, exclusively demand-fed baby, vigorously sucking in correct position.
Step V. Re-lactation is possible in some cases of secondary LF, even after many days with following measures:
• Non-nutritive sucking: Simplest measure to establish re-lactation is to place the baby on the breast at least 8-10 times/day for 10-15 minutes every time, even in the absence of milk output, termed as non-nutritive sucking.
• Drip and drop method may be useful to re-establish lactation in mothers even after many weeks. Lower end of a nasogastric tube connected to milk-filled syringe is fixed with an adhesive tape over mother 's nipple and baby is encouraged to suck on nipple while milk is gradually dripped over it. Since baby gets the milk through the tube, she/he is encouraged to suck further, which may help re-lactation.
Step VI. Alternative modes of feeding, e.g. wet-nursing by other lactating mother in family, milk sourced from human milk banking or top-feeding are very rarely indicated, when all efforts to re-establish lactation fail.
III. Breastfeeding in special situations: There are no absolute contraindications for breastfeeding except when mother is on certain drugs (Table 5.5), which are unavoidable, excreted in breast milk and can cause serious problems in baby. However, following situations are common in clinical practice, which requires a considered review of BF advisability, sustainability and modifications.
TABLE 5.5: Medications in lactating mothers
Absolutely contraindicated:
(discontinue breastfeeding, if unavoidable)
• Cytotoxic agents
• Radioactive agents
• Lithium
To be avoided:
(use alternatives, if necessary)
• NSAIDs (use paracetamol)
• Antibiotics: Sulpha, chloramphenicol, tetracycline
• Estrogen/progesterone preparations
• Thiazide diuretics
• Sulfonylureas
• Oral anticoagulants
To be used with caution:
(continue breastfeeding but monitor toxicity)
• Anti-convulsants, e.g. phenobarb, phenytoin
• Sedatives, e.g. diazepam, phenothiazines
• Anti-asthma: Theophylline
• Others: Laxatives, quinine, ethambutol
Cesarean delivery: While some mothers may be apprehensive to breastfeed soon after LSCS due to fear of pain and inappropriate advice, they should be motivated to initiate BF as soon as possible, preferably within 1 hour of birth. Mother must be helped to find a comfortable position to breastfeed, e.g. supine position on first day, side-lying position on second day and sitting position subsequently.
Working mothers: Employers must be encouraged to:
(a) permit longer maternity/lactation leave for at least 6 months after delivery, (b) permit flexible work-timings for lactating mothers, (c) provide a creche at workplace. Even in absence of these facilities, employed mothers can successfully continue BF after joining the duty by: (a) breastfeeding the baby while at home, just before leaving for work and immediately on returning home, as well as
(b) expressing the milk an hour before leaving the home (which can be stored up to 8 hours at room temperature) and fed to the baby later by caretaker with the help of Bondla or katori/spoon.
Maternal infections: Some maternal infections, e.g. HIV, CMV, HBV, etc. may be transmitted to the baby via breast milk, though the risk of transmission is usually less than the disadvantages of top-feeding. HBV positive mothers should continue exclusive BF till 6 months of age, like others. Similarly, BF is default feeding in HIV positive mothers as well in view of universal ART to mother and universal prophylaxis to the exposed baby (Ch 10.28). Top feeding should be considered only if AFASS criteria (Acceptable, Feasible, Affordable, Sustainable and Safe) is fulfilled.
Serious physical illness in mother: Most sick mothers can successfully breastfeeding their baby, either directly or through using expressed breast milk. Manual expression should continue even if breastfeeding is not possible, to prevent breast engorgement. Temporary discontinuation of breastfeeding is required if mother is: (a) seriously sick, e.g. shock, coma, etc. or (b) on contraindicated medications.
Serious psychiatric illness in mother, requires discontinuation of breastfeeding if: (a) mother is on lithium therapy, or (b) baby needs to be separated due to violent/ unstable behavior in mothers.
Maternal medications: Considerable quantities of certain drugs are excreted in BM, which may produce untoward effects on baby (Table 5.5). In these cases, three options are available: (a) temporary or permanent discontinuation of breastfeeding, (b) switch-over to alternate medications, if possible, and (c) continuation of breastfeeding with closer vigil for adverse events. Only the use of cytotoxic or radioactive drugs or lithium in mother are absolute contraindications for BF.
Preterm babies: Mode of feeding in preterms usually depends on their maturity. Most of the non-sick babies gt;1500 gm can be safely fed on breast directly or on EBM by katori/spoon/Bondla. Babies between 1200-1500 gm may need nasogastric EBM during early days. Mother's own milk as EBM is the first choice in babies who cannot breastfeed directly, followed by pasteurized donor milk or preterm formula.
Babies with cleft-palate may not generate enough suction to express breast milk. If required, they may be fed directly on breast by using the obturators or may be given expressed breast milk by katori/spoon, etc. Semi-upright position is recommended in these cases to reduce nasal regurgitation and reflux of breast milk into the eustachian tubes.
Serious physical illness in baby: Unless oral feeding is contraindicated, breastfeeding should continue either directly or through expressed breast milk. In cases when oral feeding is not possible, e.g. due to extreme prematurity, critical sickness or surgery in newborn, manual expression of mother's breast should continue to maintain milk output for future use.
Neonatal death: In this unfortunate situation, the lactation reduces spontaneously due to lack of stimulation, though the drying-up process may be hastened with some anti-galctogogues, e.g. bromocriptine, to prevent breast engorgement and maternal discomfort.
Breastfeeding during travel and social events should continue with minor adjustments in timings and practice.
5.2.5 LACTATION COUNSELING______________________
Breastfeeding plays a crucial role in health growth and development during early infancy. While it is a natural
process, some mothers may need support to successfully establish, maintain and continue BF till desired period. Objectives: Lactation counseling is a process to encourage and support these mothers for successful lactation and includes:
• Informing mothers about advantages of breastfeeding to baby as well as to mother.
• Demonstrating mothers about correct BF practices.
• Assessing the position and attachment during BF.
• Identify and mange breast and nipple problems, which may hinder BF.
• Provide solutions to mothers for BF in special circumstances and encourage them to continue breastfeeding.
Antenatal lactation counseling: Effort to ensure successful BF must ideally begin from the first antenatal visit to:
• Prime the expectant mother about advantages of BF,
• Prepare her to initiate BF immediately after the delivery,
• Assess the general health to convince her in the ability to breastfeed,
• Examine breasts for local problems, e.g. inverted nipples, and advice for corrective manoeuvres, e.g. manipulative pulling or syringe method,
• Identify potential barriers or contraindications for BF, e.g. HIV positive status or drug therapy.
Antenatal lactation counseling should specially focus on: (a) primpara mothers or (b) mothers who did not BF successfully during previous pregnancy.
Postnatal lactation counseling must begin in the delivery room to initiate BF as early as possible and should continue during each visit in postnatal ward as well as on follow-up after discharge. BF problems are more common in LSCS and low birth weight babies. Postnatal counseling must include:
• History related to timing of first feed, use of prelacteal feeds, frequency and duration of feeding, burping after feeds and any problems during BF. History should also include the state of baby after BF, e.g. cry, sleep and urine frequency to assess the adequate of feeding.
• Observation of mother while breastfeeding, to ensure correct breastfeeding position, proper attachment and signs of effective sucking, discussed earlier.
• Examine the breasts for any local breast and nipple problem, if required.
• Examine the baby for any problem as well as the weight gain after first week of life.
• Offered solutions to her problems or apprehension to encourage continuance of BF.
Mother's privacy should always be respected while observing the BF or examining the breasts, which should always be done with her explicit consent and in presence of other female members/nurse, when done by a male health care worker.
Many online and off-line courses are available at present to train health care workers for better lactation counseling practices.
5.3