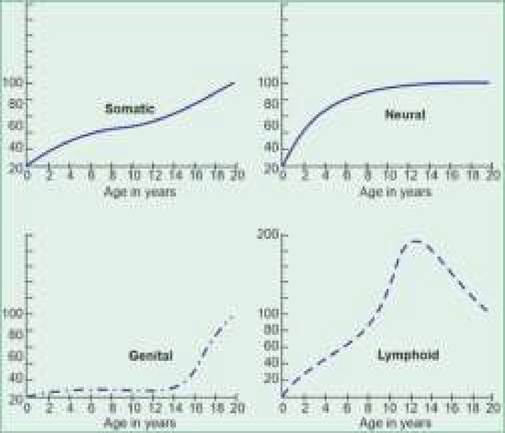
| Chronic infections: TB, worm infestations ♦ Systemic illnesses: CHDs and asthma ♦ Trauma: Head injury ♦ Drugs: Steroids and cytotoxic agents III. Extrinsic (environmental) factors - Socioeconomic factors - Cultural factors/practices - Emotional stimulation - Climatic factors *TORCH: Toxoplasmosis, rubella, cytomegalovirus, herpes simplex. • Hereditary: Children of taller parents are usually tall and vice versa. Age of menarche in daughters usually correlates well with that in their mothers. • Genetic disorders are associated with inherently altered growth potential, e.g. short stature in Turner syndrome, Achondroplasia, etc. and tall stature in Marfan syndrome, etc. • Secular trends suggests very small but consistent rise in normal weight/height values of the children at different ages over the decades, perhaps due to better environmental factors, e.g. nutrition and freedom from infections. Similar trends are noticed in terms of better final adult height and earlier age of menarche in girls. These secular trends are more marked in developing countries due to the scope for improvement and underline the need for periodic revision of reference values. II. Extrinsic (organic) factors are prime determinants of growth and development in developing countries, which directly facilitate or limit the achievement of inherent growth potential. The exact effect of these factors depends on the age, quantum and duration of exposure in relation to the period of growth. Important organic factors affecting growth/development include: • Prenatal factors involving maternal health, e.g. malnutrition, infections and systemic diseases affects growth of offsprings in three different ways: (a) during the period of organ differentiation, i.e. embryogenesis, leading to higher risk of abortions or congenital malformations, (b) during late fetal phase of anatomical and functional maturation, leading to intrauterine growth retardation (IUGR) or stillbirths, (c) during postnatal life, when maternal ill-health may affect emotional attention and quality of baby care during critical phase of growth. • Obstetrical or perinatal factors: Preterms and IUGR babies behave differently than term babies during postnatal growth period—while preterms grow faster in late infancy (catch up growth) than the term babies, IUGR babies are unlikely to show significant catch-up growth and have limited growth potential throughout the life. Other perinatal events, e.g. asphyxia, injuries, sepsis, kernicterus, etc. may also have disastrous effects on subsequent growth and development. • Postnatal factors: Postnatal growth is largely governed by hormonal influences, e.g. growth hormone in pre-pubertal period and sex-steroids during puberty; apart from adequate supply of substrates, e.g. nutrition, oxygen, etc. and freedom from infections. Malnutrition, chronic infections, e.g. tuberculosis and systemic illnesses, e.g. asthma, heart diseases, etc. are important adverse factors influencing postnatal growth and development. Head injury may lead to intellectual disability while growth of a particular limb may be affected after fractures of long bones. Prolonged steroid/cytotoxic therapy are important causes of iatrogenic growth suppression. III. Extrinsic (environmental) factors are important hindrances for normal growth in developing countries, which indirectly affect nutrition, infection rate and quantum of health care. These include: • Socioeconomic factors: Children of affluent parents have better growth due to better nutrition and hygienic conditions than those of low socio-economic status. • Cultural factors: Child-rearing practices vary indifferent communities, which may significantly impact child's growth. Routine practice of breastfeeding is a positive growth-promoting factor, while delayed weaning, food taboos and unhygienic living conditions are important adverse cultural influences in India. • Emotional factors: Adequate emotional stimulation is essential not only for psychosocial and linguistic development of a child but also for growth. Lower growth hormone levels are well documented in emotionally deprived children like orphans. • Climatic factors: Growth is slower in summer than in spring season, probably as infections are common and appetite is poor in hot and humid climate. Climate also affects the food productivity. 2.2 LAWS AND PATTERNS OF GROWTH Although each child has a unique pace of growth, certain principles are applicable to all children, as follows: • Growth is a continuous and orderly process that begins with fertilization of ovum and continues at every moment of intrauterine and postnatal life till puberty, in a fairly consistent order. • Pace of growth in not uniform throughout childhood, with intermittent periods of rapid growth, also termed as critical periods. Various phases or periods of growth (Table 1.1) may be broadly classified as follows: - Embryonic period (0-8 weeks) is the period of explosive growth in the number of cells following fertilization and implantation of the ovum in uterus as well as organ differentiation, i.e. formation of various tissues and organs. Any insult in first trimester is more likely to cause congenital malformations. By the end of this period, a fetus is structurally similar to an adult, except the differences in organ size and function. - Fetal growth (9th week to birth) is characterized by increase in size of organs (anatomical development) and functional maturation of various systems (physiological development). Intrauterine fetal growth follows an S-shaped curve with maximum growth in terms of weight gain during 24-37 weeks of life (15 gm/day) followed by gradual decline to ~6 gm/day between 37-40 weeks. However, growth in fetal length peaks at ~20 weeks with a gain of ~1 cm/month followed by gradual slowdown. Any insult in late pregnancy leads to restrictions in body size and organs, termed intrauterine growth retardation or IUGR. While a fetus is usually capable to survive ex-utero beyond 28th weeks of life (age of viability), adequate functional maturation is achieved only by 37 weeks (full term). - Postnatal growth during childhood (birth to onset of puberty) involves further physiological maturation and anatomical growth, though the pattern and pace of these changes differ in different body tissues and in different individuals, discussed later (see next law below). - Adolescent growth and development from onset to completion of puberty, is the transitional phase between child and adult, characterized by (a) physical growth spurt to attain adult dimensions, (b) sexual maturity, and (c) psychological changes in order to gain emotional and functional independence (Ch 13.3). Girls have an earlier onset of physical growth spurt during adolescence (9-12 years) than boys (˛2-15 years). • Pattern of growth is different in different body tissues. All tissues or organs do not grow at the same velocity at same age. Mainly four types of growth patterns are seen in different body tissues (Fig. 2.1). - Somatic growth is maximum in intrauterine life and follows a sigma-shaped curve in postnatal life, with two distinct growth spurts - during infancy and during adolescence. In mid-childhood, child grows slowly but steadily. Somatic growth completes at 16-18 years (earlier in females) with achievement of adult height. - Neurological growth is maximum in late intrauterine and early postnatal life, followed by rapid deceleration in late infancy and is nearly complete by two years of age. Head circumference reaches to ~95% of adult value by 2-3 years of age and any further increase is due to the increase in bony thickness rather than the brain size. - Gonadal growth is negligible till the onset of puberty, when gonads grow rapidly under endocrinal influences to achieve adult size and function during next 3-4 years of adolescence. - Lymphoid growth is maximum in mid-childhood, during 4-8 years of age. Thus, lymph nodes, tonsils and adenoids are physiologically enlarged in this ![]()
Fig. 2.1: Growth patterns in different body tissues. age group, often confused with a diseased state. Subsequently, these tissues partially regress to adult size after 8-9 years of age. • Pace of growth is unique for every child, despite comparable growth potential, determined by familial and racial characteristics. Each child experiences intermittent periods of growth spurts and stagnation. While some children grow rapidly in early life followed by slower pace, others have initially slower growth followed by late catch-up growth. • Growth progresses in cephalocaudal direction: During intrauterine life, head and upper torso grows faster than limbs as evident from higher upper vs lower segment (US:LS) ratio at birth (1.7:1) and the head being larger than the chest. Postnatally, trunk and limbs grow more rapidly with equalization of Head : Chest circumference at 1 year and US:LS ratio at 7 years. Chest circumference exceeds head circumference beyond first year of life. 2.3 NORMAL CHILDHOOD GROWTH Physical growth during childhood is evident in many dimensions by chronological changes in body size and appearance, i.e. anthropometric indicators (Table 2.2) as well as in others tissues, e.g. dentition, skeletal maturation, and internal body composition. Despite individual variations, most of these changes follow a predictable pattern and any significant deviation from this pattern may be the earliest or only indicator of ill health. TABLE 2.2: Anthropometric indicators I. Anthropometric Primary - Weight1 - Length or height1 - Head circumference1 - Chest circumference1 - Mid-arm circumference1 - Arm span3 - Sitting Height3 - Skin-fold thickness2 Derived - Weight for height2 - US: LS ratio (CR:RH ratio)3 - Stem stature index3 - Body mass index (BMI) 2 II. Clinical - Body build - Dentition - Sexual maturity rating (SMR) III. Radiological: - Bone age Should be recorded in: 1in all children, 2in malnourished/obese children, 3in short/tall stature US: Upper segment; LS: Lower segment; CR: Crown to rump; RH: Rump to heel. This chapter deals with some important patterns of growth during childhood, while adolescent growth and sexual maturity has been discussed in later chapter 13.2. 2.3.1
More on the topic Child Health in India:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- INDIA NEWBORN ACTION PLAN (INAP)
- FREE RADICALS IN HEALTH AND DISEASE
- The Genesis and Principles of One Health
- Child Abuse
- Child custody
- CASE 189: The Son of an Adopted Child
- The Estado da India
- CHASING THE GROWTH MIRAGE
|