SOMATIC (ANTHROPOMETRIC) GROWTH
Change in the body size and appearance is most obvious dimension of growth, which can be easily measured by various anthropometric parameters as follows:
Weight is the most sensitive indicator of physical growth, used not only for regular monitoring but also for early detection of diseases/recovery and calculation of drug dosages.
While precise values of body weight in normal children depend on the sex, race and other factors, as reflected in growth norms/charts discussed later, a general pattern is as follows:A normal baby weighs ~3.3 kg at birth and looses ~10% of birth weight during first 7 days of life, which is regained by 10th day. Subsequently, they gain ~20-30 gm/ day during first 3 months, ~400 gm/month during 3-12 month, ~2 kg/year till 7 years and then, ~3 kg/year subsequently till end of puberty.
Birth weight usually doubles at five months (~6.5 kg), triples at one year (~10 kg), quadruples at two years (~12 kg) and becomes seven times by 7 years (~21 kg) of age. A simple method to calculate normal Wt at different ages is given in Table 2.3 (for precise values, see Table 2.6A and B).
Stature, i.e. cephalocaudal distance is measured in terms of recumbent length up to two years of age and standing height in older children. Stature is an indicator of longterm growth, affected only after prolonged growth insult for many months. While precise values of stature in normal children depend on the sex, race and other factors, as reflected in growth norms/charts discussed later, a general idea is as follows:
At birth, a term newborn measures ~50 cm. Subsequently, the length increases by ~ 4 cm/month till 3 months (~62 cm at 3 months), then ~2 cm/month till 6 months (~69 cm at 6 months) and then ~1 cm/month till one year (~75 cm at one year).
A child gains about half of the birth length, i.e. ~25 cm in first year of life (~75 cm), half of the first-year gains, i.e.
~12.5 cm in second year (~ 87.5 cm), half of the second year gains, i.e. ~6.5 cm in third year (~94 cm) and then ~5-6 cm/year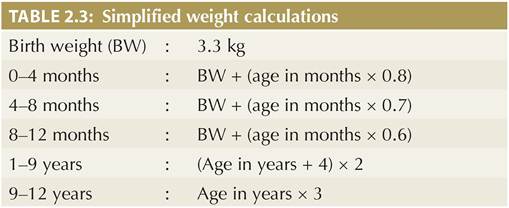
till the onset of puberty. A simple method to calculate normal length/height at different ages is given in Table 2.4 (For precise values, see Table 2.6A and B).
Parental height is an important determinant of children's height. Height of a boy at 2 years and girls at 2.5 years is nearly half of the adult height (+ 5 cm). It is possible to predict the adult height in children from parental heights, using the following formulas:
Adult Ht* (boy) = {(Mother's Ht +13) + Father's Ht}∕2 Adult Ht* (girl) = {(Father's Ht - 13) + Mother's Ht}∕2 (* predicted adult Ht + 8 cm)
Head circumference is the indirect indicator of brain growth and must be measured in all children up to 5 years of age. Brain growth is nearly complete by then and any further increase in head circumference of older children is minor and due to thickening of calvarium rather than changes in brain size. While precise values of head circumference in normal children depend on the sex, race and other factors, as reflected in growth norms/ charts discussed later, a general idea is as follows:
At birth, normal head circumference is ~33 cm, increases by ~2 cm/month till 3 months (~39 cm at 3 months), ~1.5 cm/month in next 3 months (~43 cm at 6 months) and ~0.5 cm/month in next 6 months (~47 cm at 1 year). Subsequently, it increases by only ~2 cm in second year (~49 cm at 2 years), ~1 cm in third year (~50 cm at 3 years) and technique.
Persistence of chest circumference less than head circumference beyond infancy indicates larger head, e.g. hydrocephalus or smaller chest, e.g. malnutrition. Body proportions, i.e. ratio between torso and limbs may be altered in some disorders with short/tall stature. Various terms are used to denote these proportions, e.g. upper-segment vs lower-segment ratio (US:LS ratio), crown-to-rump vs rump-to-heel ratio (CR:RH ratio) and stem-stature index (sitting Ht/standing height ? 100).
To calculate these ratio/ index, measure lower-segment height in standing position from pubic symphysis to the floor and deduct it from total standing height to derive upper-segment height.
At birth, upper segment is longer than the lower- segment. Postnatally, lower-segment grows more rapidly to equalize upper segment by 7-10 years. Thus,
• Normal US: LS ratio is ~ 1.7:1 at birth, 1.3:1 at three years and 1:1 at seven years onwards.
• Normal stem-stature index is ~70 at birth, 66 at six months, 64 at one year, 61 at two years, 58 at three years, 55 at 5 years, and 52 at 7 years.
US:LS ratio is increased in short-limb dwarfism, e.g. achondroplasia, cretinism and severe rickets; and decreased or reversed in short-trunk dwarfism, e.g. spondyloepiphyseal dysplasia, spinal deformities and Marfan syndrome.
Limb span, i.e. the distance between tips of middle fingers of outstretched hands, is another measure of body proportions, being normally 1-2 cm less than the height till 10 years of age and equals or more afterwards. Disproportionate increase or decrease in limb span as compared to height indicates short-trunk or short-limb dwarfism respectively.
Skin-fold thickness is an indicator of body fat and must be measured in selected children over the left triceps area by a Lange or Harpenden's skin-fold calipers. A skin-fold thickness of 5 years of age. Nutritional status may be classified on the basis of BMI as follows: obesity (>27), overweight (>23), normal (18.5-22.9), thinness (Delayed bone age in: (a) prematurity (physiological),
(b) nutritional deficiency, e.g. severe malnutrition, rickets, (c) endocrinal disorders, e.g. hypothyroidism, hypopituitarism, and (d) genetic disorders, e.g. Down syndrome, epiphyseal dysplasias, etc.
• Advanced bone age in endocrinal disorders, e.g. thyrotoxicosis, adrenal hyperplasia, precocious puberty, gigantism, pseudohypothyroidism. Bone age may be advanced only in affected bones in rheumatoid arthritis and arteriovenous malformations.
2.3.4