Contribution of Respiratory Dysfunction to Speech Disorders
Speech disorders related to respiratory dysfunction are often secondary to the presence of tracheostomy and/or ventilator dependence. The primary diagnoses of children requiring chronic tracheostomy and/or ventilator dependence include conditions due to trauma such as brain injury, spinal cord injury and direct injury to the trachea; congenital conditions; progressive neurologic disorders; and acquired nontraumatic conditions such as Guillain-Barre syndrome and anoxic encephalopathy (3).
It is important to note that the causes of respiratory failure and subsequent need for mechanical ventilation are not always respiratory disease or disorder. The lungs themselves may be healthy, but access to them or the systems that contribute to their function may be impaired.A primary means of airway management in the presence of chronic respiratory insufficiency is a tracheostomy. A tracheostomy is an artificial opening created between the outer surface of the neck and the trachea between the second and third tracheal rings. The opening itself is referred to as the stoma, and the tracheostomy tube inserted into the trachea through the stoma serves to maintain the opening, as well as provide means for connecting mechanical ventilatory devices. Tracheostomy provides a secure airway, long-term airway access, and a means for interface with mechanical ventilatory devices, and as such, is the most frequently used method of airway management. Placement of the tracheostomy tube diverts airflow away from the trachea through the tube and out the neck, bypassing the upper airway, including the vocal cords. Depending on the size and type of tracheostomy tube, a portion of the airflow will still pass around the tube and through the vocal cords; this may or may not be sufficient to produce sound. In the event that it is not sufficient, options to facilitate sound include downsizing of the tracheostomy tube to a smaller diameter and use of a unidirectional flow valve such as the Passy-Muir valve (4), which directs greater air flow through the upper airway and out the nose and mouth.
Table 4.2 reviews factors for4.2
Tracheostomy Tube Decision Flow Chart
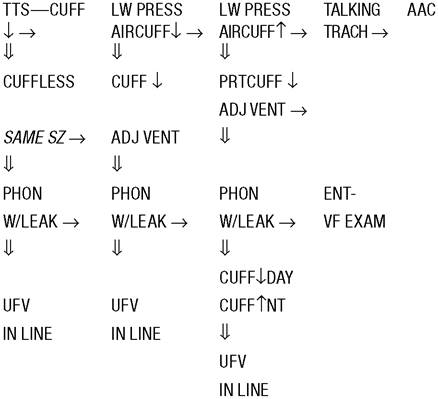
Note: A double-arrow pointing down indicates progression if successful with that step; arrow pointing to the right indicates progression if that step was not successful. Single arrow pointing down indicates deflate/ decrease pressure. Arrow pointing up indicates inflate/increase pressure.
TTS, tight-to-shaft cuff; Same SZ, same size; AAC, augmentative and alternative communication; LW PRESS, low pressure; ADJ, adjust; PRT cuff, partial cuff; ENT, otolaryngologist; VF, vocal folds; Phon, phonation; UFV, unidirectional flow valve.
Source: From Ref. 5.
consideration when determining the most efficient tracheostomy tube to use (5).
Phonation
The phonatory system is comprised of the larynx, and provides the sound source for speech. When this sound source is disrupted, it may result in alterations in voice quality, thus affecting communication.
The larynx is made up of cartilage, ligaments, muscles, and mucous membrane. It protects the entrance to the lower airway and houses the vocal cords (Fig. 4.1) (6).
Sound is generated in the larynx, and that is where pitch and volume are manipulated. The strength of expiration of air from the lungs also contributes to loudness, and is necessary for the vocal folds to produce speech (Fig. 4.2) (6).
Most of the muscles of the larynx receive their innervation via the recurrent laryngeal branch of the vagus nerve. This branch descends downward and wraps around the aorta, and for this reason, children who undergo cardiac surgery can sometimes experience voice disorders. If the recurrent laryngeal nerve is stretched or damaged during surgery, innervation to the vocal cords can be disrupted, and vocal hoarseness can occur.
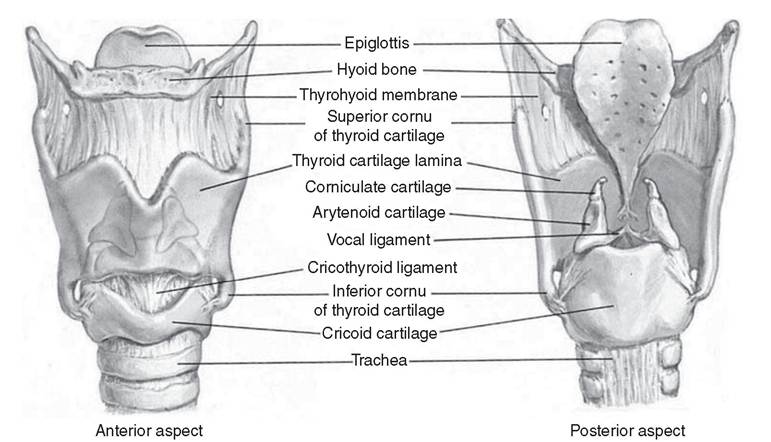
Figure 4.1 The larynx.
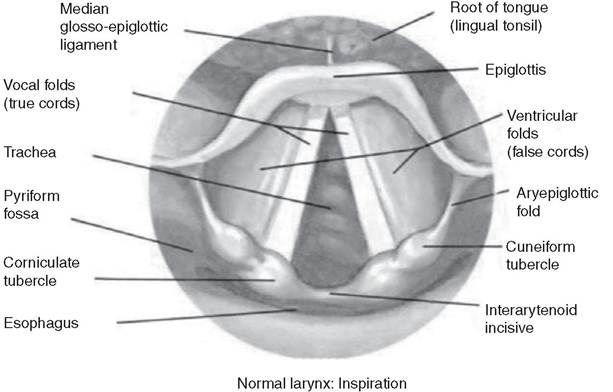
Figure 4.2 The vocal cords.

Normal larynx: Phonation